INTRODUCTION
Sport-related concussion has been defined as a traumatically induced alteration of mental status that may or may not involve loss of consciousness1,2 and usually results in impaired mental status, balance, and delayed reaction time.3 Concussions constitute between 3.65 percent and 13.1 percent of all sport-related injuries that occur while participating in collegiate athletics.4 There is also a percentage of concussions that go unreported and undiagnosed each year. Since a number of concussions go unreported, the true annual incidence is likely 40% higher because college athletes knowingly hide symptoms of their concussion and choose not to report it.5
Many different assessment tools and techniques are used to assess and diagnose a concussion and determine readiness for return-to-play (RTP). Traditional evaluation methods, such as static balance tests, may have limited clinical utility for detecting certain physiological deficits concussion patients experience after RTP.2,6,7 While static and responsive balance control must be restored, many individuals recovering from a concussion display an initial improvement in postural sway during balance assessment, but then regress after RTP.8 Furthermore, college football players who sustained a concussion during a season exhibited decreased knee stiffness with increased hip stiffness when competing in athletic competition compared to those who did not experience a concussion.9 Higher levels of overall leg stiffness leads to increased loading rates, thus increasing the risk for bony injuries such as stress fractures, while too small an amount of stiffness may lead to excessive joint motion, thus increasing the risk for soft tissue injury.10–16 These findings raise concerns that athletes who are still experiencing deficits and impairments after being cleared to return to play from a concussion may be at increased risk of lower extremity injury.
Previous authors have investigated the effects of concussion on lower extremity musculoskeletal injury risk. McPherson et al.17 conducted a systematic review and meta-analysis of studies that have examined the risk of musculoskeletal injury following a concussion in recreational, high school, college, and professional athletes. This research identified that athletes with a concussion had approximately two times greater odds of sustaining a musculoskeletal injury as compared to controls. Reneker et al.18 also conducted a systematic review and meta-analysis of studies that have examined the risk of injury following a concussion in athletes. In both military and athletic populations, the risk of any type of injury following a concussion was approximately 2.5 times higher in individuals with a history of concussion than those without a history of a concussion.18
While these systematic reviews offer valuable insights regarding connections between concussion and subsequent lower extremity injury, they are partially limited by their inclusion of broad spectrums of athletic populations and musculoskeletal injuries. It is difficult to group service members and college athletes into one cohort because individuals in the military setting may experience concussions or injuries from high-explosive blast forces,18 which is not an environment college athletes are exposed to. Prolonged military operations and exposure to improvised explosive devices (IEDs) blasts have led to significant increases in the incidence and prevalence of concussion in service members.19 Concussions were a predominant injury of the military operations in Iraq and Afghanistan, and the majority were blast related.20 A focus on a narrower patient population, such as collegiate athletes, would allow for a potentially more targeted application of findings clinically. Additionally, because neuromuscular control, sensory processing, and sensory information impairments persist after concussion, risk of subsequent lower extremity injury risk is of particular concern.21–23 Researchers have indicated that neuromuscular impairments occur following a concussion, including impairments in both gait and dynamic postural control.1,24 Thus, the risk of lower extremity injuries following concussion should be specifically examined. A preliminary literature search indicates that since the previous systematic reviews were published, new original research has been published that would support an updated systematic review with a narrower scope. Therefore, the objective of this study was to conduct an updated systematic review examining the risk of lower extremity musculoskeletal injury following a concussion in collegiate athletes.
METHODS
Search Strategy
Guidelines established within the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement were followed throughout the review. A literature search was performed using the following databases: PubMed, CINAHL, SPORTDiscus. The following search terms were used to identify relevant articles, [“concussion” OR “brain injury” OR “mild traumatic brain injury” OR “mTBI”] AND [“lower extremity injury” OR “musculoskeletal injury”].
Selection Criteria
The following inclusion criteria was applied:
-
Prospective studies examining lower extremity injuries in populations with a previous concussion;
-
Study population consisting of college athletes;
-
Studies that calculated odds, risk, and/or ratio of sustaining a lower extremity injury after a concussion;
-
Studies published between January 2000 and July 2021;
-
Studies published in English;
The following exclusion criteria was applied:
- Review articles.
A hand search of articles was performed to find additional eligible studies. References lists of included studies were reviewed.
Article Selection
To determine which articles were to be included in the systematic review, two authors reviewed the article titles and eliminated those that had no relevance to concussion or lower extremity injury. The reviewers then screened the remaining abstracts and eliminated articles that were irrelevant to the systematic review’s topic. Remaining studies’ full text were read and assessed by both investigators, and those that met the inclusion criteria were included in the systematic review. In the case reviewers did not agree, a consensus was reached through discussion. If a consensus was not made, a third reviewer provided the tiebreaker.
Quality Assessment
Included studies were assessed for methodological quality using the Downs and Black Checklist.25 The Downs and Black Checklist was modified prior to quality assessment to eliminate items that were irrelevant to studies within the selection criteria. Items pertaining to study bias and internal and confounding bias, such as items 8 and 16, were removed. Additionally, items referring to follow-up, patient compliance, randomization, and blinding, including items 9, 14, 15, 19, 23, and 26, were removed. The maximum score of the modified Downs and Black Checklist was 19. All studies were assessed independently by two reviewers. In the case reviewers did not agree on initial rankings, a consensus was reached through discussion. If a consensus was not made, a third reviewer provided the tiebreaker.
Data Extraction
Sample sizes, participant demographics, participant inclusion and exclusion criteria, quantities of concussion and lower extremity injury cases, length of injury tracking period, and primary results were extracted from each study. Data were extracted regarding the risk of sustaining a lower extremity musculoskeletal injury following a concussion.
Meta-Analysis
Review Manager software (RevMan, v 5.3; The Nordic Cochrane Center, The Cochrane Collaboration, 2014) was used to perform the meta-analysis. A random-effects meta-analysis produced a pooled relative risk (RR) calculation and 95% confidence interval (CI) that represented the overall results for the studies that provided data that allowed for calculation of relative risk. The relative risk was calculated by using the following formula:
[(number of individuals with a history of concussion who suffered a lower extremity injury/total number of individuals with a history of concussion)/(number of individuals who suffered a lower extremity injury without a history of a concussion/total number of individuals without a history of concussion)].
A relative risk value greater than one indicates that the odds of an athlete suffering a lower extremity musculoskeletal injury with a history of concussion is greater compared to those athletes with no history of concussion.26 A relative risk value less than one indicates that the odds of an athlete suffering a lower extremity musculoskeletal injury with a history of concussion is lower compared to those athletes with no history of concussion.26 The 95 percent CIs were used to determine the statistical significance of the difference in risk; if the CI crosses one, then it is not considered statistically significant. Heterogeneity of studies included in the meta-analysis was examined using the Q statistic. If the Q statistic was found to be significant, study variables that could potentially introduce heterogeneity were further analyzed. No further analysis was conducted if the Q statistic was not found to be significant. The study variable that was analyzed was the injury tracking timeline. The injury tracking timelines took place within the first 90 days of RTP and after one year of RTP.
RESULTS
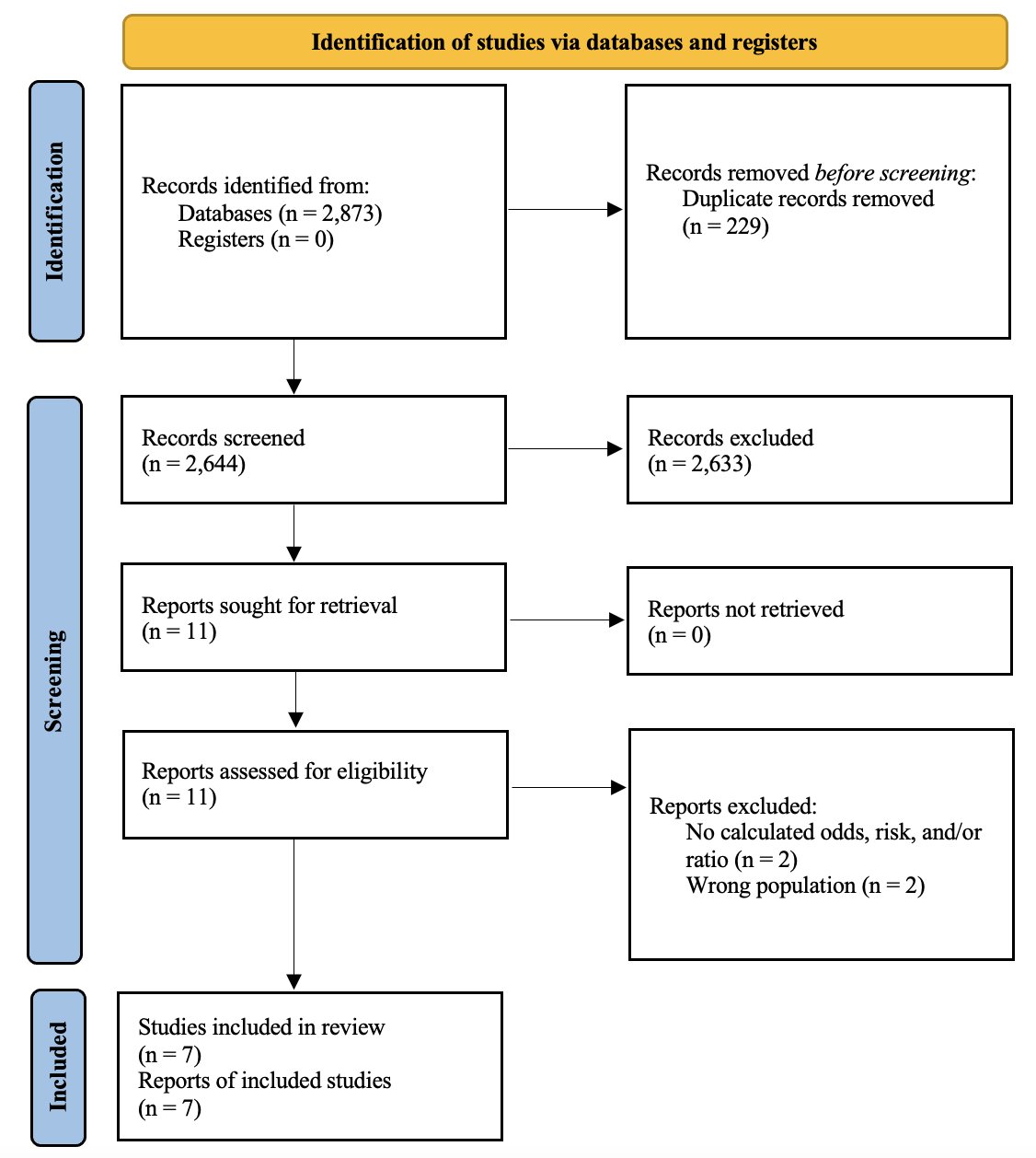
A total of 2,873 studies were identified in the initial database search. The hand search process did not yield any additional results. Duplicates were removed and 2,644 articles were identified for assessment of the title. Following removal of articles with titles that had no relevance or concussion or lower extremity injury, 27 articles remained. Once abstracts and full texts were reviewed by the two authors, seven articles met the inclusion criteria for the systematic review. With the application of inclusion and exclusion criteria, seven eligible studies were included in the systematic review. Results of the literature search are shown in Figure 1. Study characteristics are reported in Table 1.

Quality Assessment
The scores of quality assessment of the included articles ranged from 11 to 18, with five27–31 of the studies scoring 15, 17, or 18. Scores between 16 and 19 were considered excellent quality, scores between 12 and 15 were considered good quality, scores between nine and 11 were considered fair quality, and scores less than nine were considered poor quality. These scores indicate that most of the studies were of good or excellent quality. Some of the reasons for the high-quality scores include clearly describing the study objective, outcome measures, and results, providing the actual probability values, choosing individuals who were representative of the desired population, and matching individuals to controls of the same population. Even though healthy, non-concussed controls were matched for potential confounding factors (i.e., sex, sports, position) in five studies,27–31 two27,28 reported that exposure levels may have not been the same between the concussed athlete group and the matched controls. Sample sizes of the concussed athlete group ranged between studies, ranging from 1227 to 36432 athletes.
Demographic Data
Participants in two28,30 studies were of one sex. Of the remaining five studies, four27–29,33 provided a sex breakdown of the two groups. Of those studies, there were 265 male and 83 female athletes in the concussion groups while there were 349 male and 133 female athletes in the control groups.27–29,33 Sport and participation levels for each study are included in Table 1. Six27–32 studies provided the sports in which the athletes from the concussion group participated. Not all sports were analyzed amongst the studies; the sports frequently investigated were football, men’s and women’s soccer, men’s and women’s basketball, and swimming. Other sports investigated include hockey, wrestling, volleyball, baseball, softball, tennis, cheerleading, golf, field hockey, and rowing. Control athletes, when implemented, were matched by sport and sex. Some studies matched athletes by exposure and position as well.27,28,31,32 Lynall et al.32 further matched concussed athletes to control athletes by age, height, and weight. As for the lower extremity injury time tracking period following concussion, three studies27–29 tracked concussion patients for 90 days after their concussion, one32 reviewed the injury history of the concussed individuals until the end of their intercollegiate athletic career, and another study31 looked at the time before and after 90 days, 180 days, and 365 days of the concussion.
Individual Study Results
Overall, there was a wide variety of inclusion and exclusion criteria for classifying musculoskeletal injuries. The variability of classification of lower extremity injuries amongst the studies may contribute to the different relative risk and results of each. Herman et al.29 found that the odds of sustaining a lower extremity musculoskeletal injury were 3.39 times higher in concussed college athletes, which was the largest odds ratio of all the studies investigated. Two studies30,31 found that individuals with a history of a concussion displayed higher lower extremity injury rates than the control group after 365 days following RTP from a concussion. It was shown that individuals with a history of a concussion were at increased risk of lower extremity musculoskeletal injury27,28,33; and the odds of sustaining a lower extremity injury during the first 90 days of RTP were 2.48 times higher in individuals with a history of concussion compared to those with a history of concussion.27 Furthermore, the odds of experiencing a lower extremity injury were 3.00 times higher in individuals with a history of multiple concussions compared to individuals with a history of a single concussion or no concussion history at all.32
Meta-Analysis
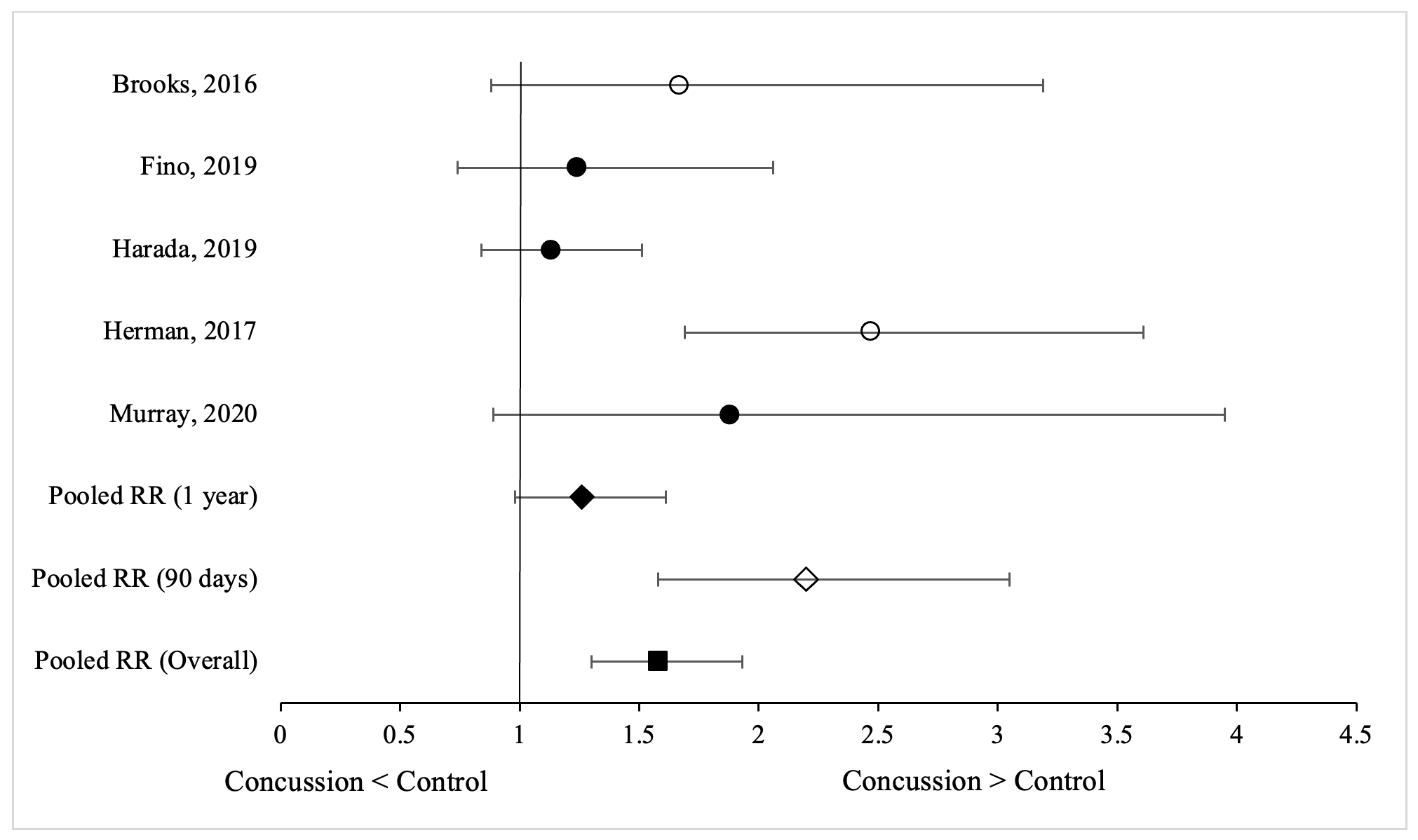
Meta-analysis of relative risk was performed using five27–30,32 of the seven studies. In the studies that provided sufficient information to perform calculations, the risk of athletes sustaining a lower extremity musculoskeletal injury after a concussion was compared with athletes sustaining a lower extremity injury who did not have a history of a concussion. Studies were not included in the meta-analysis portion if the data was insufficient for calculating relative risk. Overall, athletes who sustained a concussion had greater risk of lower extremity musculoskeletal injury compared to athletes without a history of a concussion (RR = 1.58[1.30, 1.93]) (Figure 2). Positive tests of heterogeneity were detected within comparisons of injury tracking timelines amongst the studies (Q = 11.46, p = 0.02). Subgroup analysis of injury tracking timelines revealed that the risk of lower extremity injury is particularly elevated within the first 90 days of RTP following a concussion (RR = 2.20[1.58,3.05]), but it is not significantly elevated one year after RTP (RR = 1.26[0.98,1.61]).

DISCUSSION
This systematic review and meta-analysis revealed that individuals are at greater risk of sustaining a lower extremity musculoskeletal injury following a concussion compared to individuals without a history of concussion. College athletes who suffered a concussion possessed a 58% greater risk of sustaining a lower extremity musculoskeletal injury than those who did not have a history of a concussion. The overall duration of this increased risk is unknown, but this risk may last up to one year from injury. The detection of heterogeneity reveals that the small sample of studies varied in their findings. The sub-analysis revealed that college athletes with a history of concussion appear to be at increased risk of lower extremity injury within the first 90 days of RTP, but not at the one-year mark. Injury risk does not appear to remain elevated in spite of evidence that motor impairments persist.34 The neuromuscular control deficits that individuals experience following a concussion may not be as severe, or even present, at the one-year mark compared to during the first 90 days. The ability of the neuromuscular control system to respond to disturbances may improve over time,35 but further research would need to be conducted to verify this hypothesis and determine an average timeline for recovery of these deficits.
These findings suggest that it is important to evaluate these individuals at different time points following RTP. It is not common to re-evaluate individuals who have been cleared to return to sport following a concussion. The findings suggest that re-evaluation may be beneficial and could possibly reduce future injury risk. Even though athletes are no longer experiencing concussion-like symptoms, they may still be experiencing motor abnormalities following return to play. However, these abnormalities may not be detected if the individuals are not re-evaluated.
This systematic review expands on the review performed by McPherson et al.17 by including three additional studies published since the publication of their research. One29 of these studies was included in the current meta-analysis. With the addition of the one study, the meta-analysis revealed similar results to the one performed by McPherson et al.17 Thus, this systematic review further emphasizes that collegiate athletes who have suffered a concussion are at increased risk of lower extremity injury compared to those without a history of concussion.
This meta-analysis strictly examined intercollegiate athletics; whereas the meta-analysis performed by McPherson et al.17 examined professional, recreational, and intercollegiate athletes. The included recreational athletes spanned from 18 to 29 years of age, which may serve as a confounding factor for the increased injury risk. Older individuals generally possess decreased musculoskeletal strength compared to younger individuals, which may serve as a risk factor for future injury.36 On the other hand, an increase in the number of years of experience in a specific sport may reduce an individual’s injury risk because they are an “expert” with better movement patterns and biomechanics.37 The meta-analysis performed in the current study included articles with a specific population, one of strictly college athletes. Since male college athletes were more frequently represented in the included articles, the findings are most applicable to this population. It is difficult to make a determination about the effects of concussion on lower extremity injury risk for males and females of different age groups.
The mechanism behind the increased risk of experiencing a lower extremity musculoskeletal injury is not yet fully understood, but several potential explanations exist. One explanation, which was not assessed with this study, is that a previous history of lower extremity musculoskeletal injury may place these individuals at increased risk of suffering a future injury. It has been shown that previous injury serves as a risk factor for future musculoskeletal injury.38,39 Strength imbalances between muscles have been suggested as risk factors for lower extremity injuries, and may be a consequences of a previous injury.38 Muscle imbalances may affect the efficiency of movements that involve quick accelerations and decelerations, which are common actions in athletics.38
Concussions can involve multiple and varied regions of the brain, including those associated with orienting and executive components of visuospatial attention.40 The regions of the brain that are responsible for these attentional networks include the parietal, frontal, and temporal regions, the cingulate cortices, and the midbrain.41 When one suffers a concussion, these regions may become damaged or impaired, which compromises the ability to process stimuli in terms of disengagement, movement, and re-engagement.42 Even after classic concussion symptoms resolve, there is a possibility that neural and neuromuscular impairments are still present. There is ongoing research in this area that has revealed that individuals continue to experience neuromuscular, neurocognitive, sensory processing, and balance deficits related to concussion well after RTP.
Research has indicated that degradation of neuromuscular control, sensory processing, and sensory information can lead to increased injury risk.31,32 With regions of the brain associated with the executive components of visuospatial attention being most susceptible to damage following a concussion, individuals may possess deficits in processing important information while ignoring extraneous stimuli.35,40 Reduced speed of response to peripheral visual stimuli after concussion may negatively affect anticipatory muscle activation that relies on peripheral visual awareness.43,44 If individuals utilize improper or delayed muscle contractions, they may perform movements that place them in vulnerable positions, which could potentially increase their risk of musculoskeletal injury.
Which specific deficits and how they interact within the individual to increase injury risk has not yet been determined. It has been shown that neuromuscular impairments are risk factors for future injury45,46; and with individuals still experiencing such deficits after return to activity, they may be influential risk factors for sustaining a future musculoskeletal injury.35
Research has shown that individuals still experience lingering gait deficits, including decreased gait speed, cadence, and stride length during dual-task activities following resolution of concussion symptoms.19,47 When these impairments are linked with dual-task conditions, athletes may not be able to coordinate or focus as easily as they were able to prior to their concussion. The addition of a cognitive load may further compound the neurocognitive deficits these individuals already possess and experience. This may lead them to compensatory movement patterns that place stress on body structures that are unable to support this force, and thus make the individual more susceptible to injury. Research indicates that concussed individuals change their gait strategy by spending more time in double-leg stance compared to single-leg stance and possess lower mean gait velocity at 72 hours post-injury compared to non-concussed athletes.48,49 Furthermore, research has shown that individuals with a history of a concussion possess gait abnormalities up to 90 days following a concussion.50,51 With these individuals possessing an altered gait strategy days or weeks after experiencing a concussion, this may serve as a possible indication of the systems of movement that continue to be affected by the injury.
Another possible explanation for the increased injury risk is that individuals with a history of concussion may adopt new movement patterns,22 which may help them “pass” the clinical assessments, such as static balance tasks, in the RTP concussion protocol. It has been suggested that individuals with a history of a concussion maintain upright posture by using more top-down control than bottom-up control compared to individuals without a history.33 Even though the athletes are able to complete the clinical evaluation, it does not necessarily mean that they performed it with the same skill level or motor strategies prior to their concussion. Stride length during gait is significantly shorter for up to 14 days after concussion with a dual-task condition compared to a single-task condition, and gait velocity is significantly slower for up to 28 days post-injury with a dual-task condition compared to a single-task condition.52
Concussed athletes also demonstrate lasting balance impairments following RTP, particularly deficits in dynamic balance48,50,51,53–55 Authors have shown that athletes with a history of a concussion, upon RTP, are able to perform static balance tasks without any difficulty, but struggle to perform dynamic balance tasks.56 Reduced balance performance indicates that an individual is less capable of responding to perturbations and sensing their body’s position in space, potentially leading to mispositioning of the lower extremity. Thus, a balance deficit can place athletes at an increased risk of sustaining an injury. Reduced single-leg balance performance is associated with eight times greater risk of ankle sprain injury.57,58 Returning to baseline values for single-leg balance is an assessment that may not be sensitive enough to detect lingering impairments in concussed athletes.
Future Directions
Healthcare professionals should be aware that collegiate athletes are at increased risk for lower extremity musculoskeletal injury following a concussion, even after being cleared for RTP. Many of the RTP concussion protocol tests are important, but some are subjective, such as the symptom checklist. Research has suggested that current concussion evaluation methods may not possess sufficient sensitivity to detect any lingering concussion-related abnormalities that persist after symptom resolution.59,60 Research should work to identify new methods to evaluate athletes during the RTP concussion protocol to ensure that they are fully prepared to return to their sport and are not experiencing subtle or lingering deficits when returning to participation. It also needs to be determined which lingering deficits or impairments are the cause of this increased risk of injury. If a history of concussion is the factor responsible for increasing the injury risk in these athletes, future research should look to further investigate the neuromuscular changes that are brought about by concussions. Per the sub-analysis findings, it is also important to evaluate college athletes at different time points following RTP after a concussion.
Finally future research can place a larger focus on female collegiate athletes and examine the effect of concussion on lower extremity injury risk on these individuals. Studies can also investigate the effect of concussion in other populations, such as athletes in the secondary school setting and those in recreational or community leagues.
Limitations
This systematic review had a few limitations. Even though the concussed athletes were matched with control groups by sport and position, there are other factors, such as behavior or personality traits of the athletes that could have affected the results.32 If an athlete is more aggressive or partakes in riskier athletic behavior, it may place that athlete at a higher risk of sustaining a musculoskeletal injury.32 Many different sports were explored in each study, thus limiting the ability to draw conclusions regarding the effect of concussion on lower extremity injury risk in specific sports. Not all studies examined athletes of both sexes, making it difficult to make a determination about the effect of concussion on lower extremity injury risk for males and females separately. Another limitation is that the criteria for classifying a lower extremity musculoskeletal injury differed across studies. This could affect the injury risk reported in the included studies, as some studies may have included an injury that another study excluded.
CONCLUSION
The results of this systematic review and meta-analysis indicate that history of a concussion appears to increase the risk of suffering a lower extremity musculoskeletal injury in college athletes. Although not statistically significantly different, following RTP, increased risk is strong at three months post-concussion, but not at one year. Further research is needed to explore and determine the neuromuscular mechanism behind this increased risk of injury and to develop return-to-play criteria that are capable of identifying those at increased risk of lower extremity injury after concussion.
Conflicts of Interest
The authors report no conflicts of interest.