INTRODUCTION
Low back pain (LBP) is a debilitating condition that can affect anyone, from the most talented athletes to those beginning to learn fundamental movement skills.1 It is estimated that two thirds of adults will have been or will be affected by NSLBP at some point in their life.2,3 This condition can cause a person to have poor performance in their occupation, sport, or activities of daily living (ADLs) as it limits their ability to maintain basic movement mechanics to ensure optimal performance. LBP can be defined as any painful stimulus in the region between the floating ribs and the gluteal folds that can cause common or even debilitating conditions with or without leg pain.4 LBP can be specific or nonspecific, however only approximately 10% of LBP is actually specific and has a clear answer as to why the pain is present, leaving the remaining 90% as NSLBP.4
While the etiology of LBP is still debated, it is thought that the pain arises from several different factors depending on whether it is specific or nonspecific. Specific LBP will have a diagnosed pathology such as a muscular strain, infection, fracture, or a spinal disease.5 On the other hand, NSLBP has no definitive pathology regarding what is causing the pain but has been theorized to be caused by factors including poor posture, impaired flexibility, previous history of injury, heavy lifting, mental stress, and obesity.5,6 Other potential causes of NSLBP are also common impairments identified in patients, such as deep trunk muscle weakness, poor coordination, and muscular imbalances.6
The treatment approach to manage NSLBP varies depending on clinician and patient tolerance.7 Common treatments have similar goals, as massages aim to promote relaxation of the musculature, while modalities can be used to decrease pain levels. Treatment approaches including massage, medication, and modalities have demonstrated short-term effects of reducing pain.5,8 Each of these management strategies requires specific equipment, recurring healthcare visits, or prescriptions. Additionally, treatment frequency may influence the patient’s financial burdens and a feeling of dependence on the provider and the services provided.
While debate remains surrounding the best management strategy, staying physically active has positive effects in decreasing NSLBP.9 Using exercises to activate and strengthen the core (i.e. CSE) have shown to be a promising method for treating NSLBP.4,6,10,11 The goal of CSE is to improve and recover the ability to control the spine.6 This approach is geared towards reeducating deep trunk muscle function, and coordination of deep and superficial trunk muscles during static, dynamic, and functional tasks.4 CSE place focus on the core musculature that includes the transverse and rectus abdominis, the internal and external obliques, paraspinals, as well as musculature of the gluteals, pelvic floor, and hip. A CSE program may promote patient independence with a home exercise program (HEP). Subsequently, CSE may also represent a cost-effective approach for patients to manage their NSLBP after initial treatments. Allowing a patient who has NSLBP to better manage their own symptoms after rehabilitation sessions and become self-sufficient which may decrease reliance on healthcare providers.
The purpose of this systematic review is to examine the efficacy of CSE in the treatment of NSLBP in adult patients.
METHODS
Search Strategy
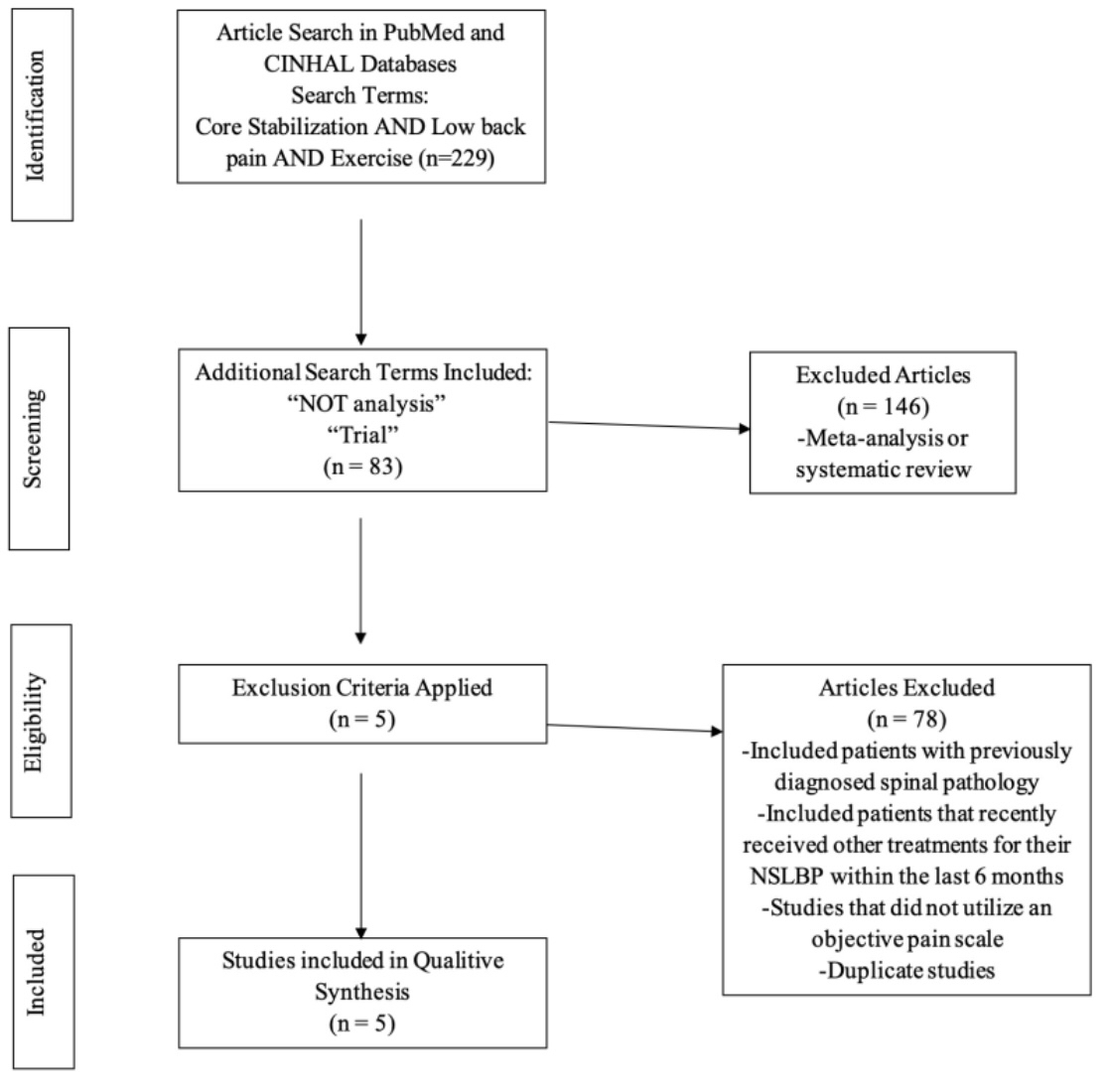
The electronic databases of PubMed, Sports Medicine & Education Index, and CINAHL were accessed on January 20, 2022, to find previous research on the effectiveness of CSE in patients with NSLBP. The search terms utilized were “core stabilization”, “low back pain”, and “exercise”. To funnel the search, “trial” and “NOT meta-analysis” were added in order to target RCTs and reject meta-analyses, in addition to utilizing the inclusion and exclusion criteria to eliminate any meta-analysis and include only clinical/controlled trials.
Inclusion and Exclusion Criteria
A manual review of the remaining article titles and abstracts was performed by two independent reviewers (ZRS, SLW) to exclude non-relevant articles. Consensus was reached on all articles meeting the a priori criteria before methodological quality assessment and any disagreements were resolved by a third party (CJB). For an article to be included, it must have: 1) included patients between 18-64 years old; 2) patients with NSLBP; 3) used CSE as an intervention; 4) been written in English. Exclusion criteria for articles included: 1) studies with patients who had previously diagnosed or current specific spinal pathology; 2) studies with patients who had received other treatment for their NSLBP within the prior six months; 3) studies that did not incorporate a pain scale.
Assessment of Methodological Quality
Each of the articles was assessed for quality using the PEDro scale. The PEDro scale is an article rating system used to help determine the validity of studies based on work by Verhagen and colleagues.12
RESULTS
The results of the search can be found in Figure 1. The initial search yielded 229 articles which were screened for further inclusion. Additional search terms were included to identify only clinical trials and exclude reviews leading to a total of 83 articles. After full text review, five studies remained that fit the inclusion and exclusion criteria and were used for this systematic review.

Methodological Quality
Two independent reviewers (ZRS, SLW) separately assessed each article for quality using the PEDro scale. The PEDro scores for the five studies had a mean value of 6.40, with a range from 5 to 8 (Table 1). All five studies were unable to blind the subjects or therapists due to the nature of the study itself. Another common limitation was not employing an intent-to-treat analysis. The research identified consistent, moderate-quality evidence supporting the efficacy of CSE in people with NSLBP. This would be considered grade B using the strength of recommendation taxonomy.
Synthesis of Results
Five RCTs were included in this systematic review that included total of 275 patients ranging from ages 18-60, with a total of 123 patients receiving a CSE treatment compared to either a control group or another intervention (Table 2). Four of the five studies used pressure feedback and used the Visual Analog Scale (VAS) for pain,4,10,11,13 with Areeudomwong and colleagues using the Numerical Rating System (NRS) for pain.6 Both pain scales have been seen to be reliable and effective measures of rating pain.14
Akhtar et al. compared CSE versus general physical therapy (PT) exercises in the treatment of NSLBP.4 The treatment of the CSE group aimed at targeting deeper muscles of the abdominals, including transversus abdominis and multifidus, which was combined with tactile feedback. The routine PT group did not use any biofeedback and their intervention consisted of flexibility exercises. In the comparison group, subjects were given baseline ultrasound and TENS treatment in addition to performing exercises three times a week for six weeks, one day a week with a physical therapist and the other two days using a HEP. The researchers concluded both techniques proved to be effective in managing LBP, but CSE displayed greater reductions in pain scores compared to general PT, with a mean VAS change of 3.08 (CSE) vs 1.71 (PT group).4
Bhaduria and Gurudutt compared lumbar stabilization, dynamic strengthening, and Pilates as exercise interventions for LBP.10 According to the authors, lumbar stabilization focused on improving neuromuscular control, strength, and endurance to promote pelvic and lumbar stability.10 The goal of dynamic strengthening was to strengthen the spinal column and supporting structures. Pilates focused on maintaining a neutral spine and pelvis through activation of the core using controlled breathing. They used the VAS for pain, the Modified Oswestry Disability Questionnaire (MODQ) to measure disability, and pressure biofeedback to measure core strength. After completion of 10 sessions, pain and disability were significantly decreased in the lumbar stabilization group by 6 and 32 points for the VAS and MODQ, respectively. Although all three forms of therapy were beneficial, lumbar stabilization was superior.
Areeudomwong and Buttagat compared CSE, proprioceptive neuromuscular facilitation (PNF) training, and standard therapy regarding their effects on pain intensity, functional disability, and trunk/neuromuscular response during maximal voluntary contractions of the trunk flexors and extensors.6 CSE focused on recruitment of the deep abdominal muscles by utilizing abdominal hollowing techniques and pressure biofeedback. The PNF group progressed exercise difficulty over the course of four weeks starting with isometric contractions and ending with dynamic concentric and eccentric contractions of the trunk flexors and extensors. Lastly, the standard therapy group only did general trunk strengthening with 5-10 minutes of ultrasound performed (1MHz, continuous, frequency: 1.5-2.5 W/cm2); the authors did not specify if the ultrasound was provided before or after the exercises. Each group participated in three weekly sessions that were 30 minutes each for a duration of four weeks. After four weeks of intervention the PNF group demonstrated positive short term pain outcomes assessed as well as long-term pain outcomes assessed at a three month follow up (using the NRS pain scale). Both PNF and CSE showed greater reductions in pain and disability scores and improved patient satisfaction compared to the control, although the authors did not indicate how patient satisfaction was measured. Overall, Areeudomwong and Buttagat found that CSE had greater short-term effects on pain and function with better levels of muscle activation than the control group.6
Inani and Selkar compared the effects of CSE versus conventional exercises on lumbar joint position sense in patients with LBP using the VAS, MOQD . These outcome measures were performed at baseline and after three months.11 One group received four phases of CSE that started with activation of deep muscles and progressed to functional re-education exercises. The other group performed conventional stretching and isometric exercises. Both groups also received equal number of treatments of short-wave diathermy and intermittent lumbar traction. Both groups improved over time, but the CSE group had greater reductions in pain and disability outcomes (change scores: 4.93 on VAS, 14.6 on MODQ).11
A randomized controlled trial by Hlaing et al.13 compared CSE to strengthening exercises and evaluated proprioception (joint repositioning), balance (Romberg test), muscle thickness using ultrasound, and patient-reported outcomes such as VAS (pain) and MOQD. A total of 36 patients with NSLBP completed the four-week clinical trial. The CSE protocol was broken into two phases (weeks 1 & 2, weeks 3 & 4), with the first phase focusing on activating the transversus abdominis and multifidus using drawing-in exercises. The second phase focused on incorporating transversus abdominis and multifidus activation during functional exercises in the quadruped position and standing. The strengthening group completed exercises that targeted the anterior and posterior musculature (trunk flexors and extensors) in prone and supine positions. The CSE group showed significantly better improvement than the strengthening group in proprioception, balance, and increase in muscle thickness. However, reduction in pain was not significantly different in the CSE group compared to the strengthening group.
DISCUSSION
Each of the five included articles reviewed examined similar outcomes of pain, disability, and function. In addition, each article had similar treatments that focused on core stabilization. The results of the included five studies gave valuable insight on the effectiveness that CSE offers patients who suffer with NSLBP. While there is still no definitive superior treatment for NSLBP, one can conclude that CSE is an effective method for treating NSLBP. All five studies indicated that CSE resulted in lower pain ratings, improved self-reported function, and muscular function.4,6,10,11,13
With this knowledge of the effectiveness of CSE provided in this review, healthcare providers may be better equipped to effectively treat patients with NSLBP. In addition to reducing pain and improving patient-reported outcomes such as the MODQ, CSE may also influence neuromuscular control.6 Muscular activation and cross-sectional area of the transversus abdominis and multifidus were improved, as was proprioception and balance, after patients completed various CSE protocols.6,13 Placing proper attention to muscle activation, strengthening the spine and core can help to build a strong base of support for the body to aid an individual’s ADLs. Using the findings of this systematic review to influence treatment plans with emphasis on earlier CSE intervention to improve NSLBP symptoms of pain, disability, and function may be beneficial. It is worth noting that most of the included studies combined modalities with CSE. This may suggest that while CSE can lead to improved outcomes, it is unclear if the modalities or exercises were driving patient improvements. While some providers may think rest is the best medicine based on previous literature and clinical knowledge, the incorporation of CSE has been associated with greater benefits than being inactive.11
One key consideration with CSE is varied pain tolerance and ability to perform exercises that exists in patients. Older populations may require supplementary supervision to ensure proper form, engagement and safety as fall concerns may arise when progression occurs. Additionally, older populations may require exercises to be adjusted based on previous history, mental capacity and overall stamina. The studies included in this review indicate that both pain and disability are reduced following CSE across various age groups. Further analysis revealed that similar effect sizes were observed for pain reduction in NSLBP patient samples in their mid-twenties6 as well as their mid-forties (Table 2).4 This indicates efficacy of CSE across various age ranges. Nevertheless, the concept of engaging and strengthening the spinal and core muscles is a critical component that should be included in CSE interventions for NSLBP.14
The progression of CSE treatments that were identified in this review demonstrate that the appropriate progression may be a critical factor for NSLBP treatment success. Most of the included studies used a two-phase approach to CSE with the first stage focusing on activating the deep abdominal musculature and the second focusing on integrating this activation into functional movements. When beginning, programs should begin with aerobic activity and stretching to warm-up musculature. The next step is educating patients on paying attention to a neutral spine and activation of the core during exercises.15 Once core activation is mastered, advancement to exercises that strengthen the surrounding muscles of the spine in varied positions should commence. The exercises progress from supine, to hook lying, to sitting on a physioball and then to standing and functional movements a patient would use every day.15 During advanced progression, additional emphasis should also be placed on balance and coordination during movements.15 Further information on the principles guiding CSE can be found in Aukuthota et al.15
Patients may benefit from reduced financial burdens and improved self-efficacy in managing their symptoms with CSE. One study incorporated an HEP into their CSE plan of care, finding that CSE was effective at decreasing pain and had greater core activation.4 Those results aligned with the findings of this systematic review that CSE is effective at reducing pain. This SR also established that CSE has the potential to increase the long-term cost effectiveness for patients as it allows them to perform CSE outside of a rehabilitation setting once properly instructed. During initial sessions, clinicians should work towards improving a patient’s ability to self-manage their symptoms to decrease unneeded visits and costs for patients. Clinicians should also consider educating patients on appropriate posture, ergonomics and what to do if their NSLBP recurs after discharge. In turn, it may be possible that CSE could decrease cost to third party payers and patients. However, costs of treatment were not evaluated in any of the studies and cost-effectiveness remains an important unanswered question in this field.
While the long-term effects of CSE are still unknown for patients with NSLBP, the positive short-term results found in this review provide optimism for long-term results. The lack of long-term studies may be due to the inability to follow patients through life along with conflicts with schedules, or compliance with long-term HEPs. Future studies should further evaluate the effects that CSE may have on long-term NSLBP regarding pain and function. In addition to long-term effects, future studies should examine the role of CSE in short and long-term effects for specific LBP as beneficial results were seen in patients with NSLBP.
Many treatment options exist for LBP, and only a handful were compared to CSE in this systematic review. While some methods such as the McKenzie Method may have greater success in reducing pain with chronic LBP, this method has not been shown to be superior for treatment of patients with acute LBP.16 The McKenzie Method also requires clinicians to take costly classes that may not be reasonable at the time for some providers. Pilates is another technique used for treatment of NSLBP, although the evidence does not support that it is better than CSE for the treatment of NSLBP.8,17 Another intervention strategy for NSLBP is Tai Chi, which may be a better solution for elderly patients due to the slow movements and benefits of reducing depression symptoms.18 While stretching and strengthening have seen success as well, these are commonly recommended to be combined with CSE for improved patient outcomes.10,19
A major limitation of the current literature is that results for CSE are only supported for the short term. Very few studies have looked at the long-term effects of CSE at treating NSLBP with most studies following patients for less than three months with no future follow ups. There is a critical gap for long-term outcomes in future research as the longest follow-up was three months in the studies that were identified.9,11 Many of the included studies (4 of 5) paired CSE with another modality, limiting the ability to draw conclusions specific to the efficacy of CSE in isolation. Since most modalities were used to control pain, it remains a possibility that the modalities were a driving factor in the reduction of pain following CSE interventions. Future research should aim to investigate the efficacy of CSE in isolation. Lastly, the five studies also had no blinding of the subjects or therapists. This may be due to the similar treatment approaches between the control groups and the experimental groups for each. Future researchers may want to consider employing more rigorous experimental designs to better understand the short- and long-term impact of CSE on patients with NSLBP.
CONCLUSION
Core stabilization exercises have been widely used and become more popular over the years with healthcare providers for treatment of NSLBP. Based on the results of this systematic review, there is grade B evidence to support the use and efficacy of using CSE to decrease symptoms and improve patient function in patients with acute NSLBP. While the clinical benefit of CSE has was demonstrated in the short term, the long-term effects remain unclear.
Conflicts of Interest
None to declare.