_of_the_ischi.tif)
INTRODUCTION
Avulsion fracture of the ischial tuberosity is uncommon. Patients with this injury typically present with symptoms consistent with hamstring strain. This apophyseal injury has been reported in various sports, especially in adolescent athletes involved in gymnastics, soccer, or running hurdles.1 Among 55 adolescent gymnasts who sustained pelvic avulsion fractures, the location was the ischial tuberosity in 45.1 Avulsion fractures of the ischial tuberosity are treated nonoperatively in 90% of cases, with an expected return to sport after three months.2 To the authors’ knowledge, avulsion fracture of the ischial tuberosity in an athlete with an endocrine disorder has not been reported. The authors present the case of an adolescent gymnast with a history of growth hormone deficiency (GHD) who sustained an avulsion fracture of the ischial tuberosity. The purpose of this case report is to describe an avulsion fracture of the ischial tuberosity and subsequent recovery in an athlete with an endocrine disorder.
CASE DESCRIPTION
The subject of this case report and her parents were informed that the data concerning the case would be submitted for publication and provided consent. A 15-year-old United States of America Gymnastics (USAG) level 9 gymnast presented with right hamstring pain after regular practice. She had been diagnosed with isolated GHD at age 4 and treated with growth hormone replacement therapy until age 14. After cessation of the HGH intervention, she continued to have normal physical growth, as indicated by records from her pediatric endocrinologist. She had delayed menarche at 16 years and had a history of secondary amenorrhea despite normal weight for her age.
Six months before presentation, she experienced the insidious onset of dull, aching pain in her right hamstring, near the junction of the thigh and buttocks, that was believed to be the result of a chronic hamstring strain. The pain increased gradually over a year and was relieved with rest, massage, and dry needling. Two days before presentation, she felt a “snap” and pain while performing a switch leap during regular practice. She had sharp localized pain in the proximal hamstring with walking and sitting.
OUTCOME
Examination
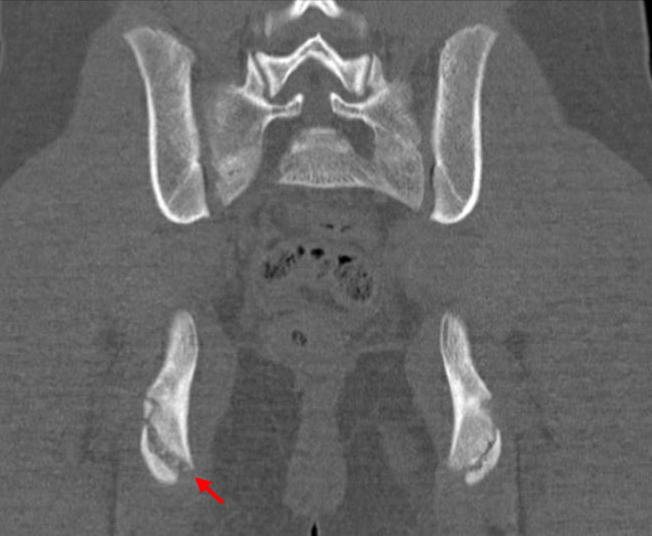
Upon physical examination, the subject had tenderness over the ischial tuberosity and painful restriction of right hip flexion, especially with knee extension in this position. Although radiographs were normal, computed tomography showed an asymmetric 6-mm widening in the right ischial tuberosity epiphysis compared with the other side (Figure 1). Magnetic resonance imaging of the pelvis showed edema of the ischium near the origin of the hamstring tendon at the fracture site (Figure 2). She was diagnosed with a Type 2 avulsion fracture of the ischial tuberosity (displacement of 0–2 cm) according to the classification system proposed by McKinney et al.3 She chose nonoperative treatment and was subsequently treated with rest, ice, and non-weightbearing ambulation with crutches. Her serum growth hormone level (327 pmol/L) was within normal range. Radiography indicated a bone age of 13 years, but her chronologic age was 15 years 4 months.

_of_the_ischi.tif)
The subject was advised to continue to be non-weightbearing until she was pain-free with radiographic fracture healing, which occurred three months after the injury.
INTERVENTIONS AND OUTCOMES
The subject underwent rehabilitation with the athletic trainer. Starting three months post injury, her rehabilitation was focused on gaining hip range of motion for two weeks followed by strengthening of hip, lower extremity and core muscles, and gait training. Patient also underwent training for proprioception, running, and sprinting. She was then allowed to begin vault training at four months, and running at five months, after her injury. She could perform switch leaps and splits seven months after injury. She participated in a USAG level 9 competition 12 months after the initial injury. At a three-year follow-up, she continued to practice gymnastics and compete in level 10 USGA competitions without any symptoms related to her avulsion fracture of the ischial tuberosity.
DISCUSSION
Although growth plate injuries are common in adolescents performing gymnastics, the present case report suggests that gymnasts who have a history of growth hormone replacement therapy should be aware of the potential delay in clinical recovery after physeal avulsions. Chronic pain in any joint in a competitive gymnast should be evaluated for widening of the growth plate with conventional radiographs. This patient's long recovery may be attributable to her history of growth hormone replacement therapy and delayed physeal maturity.
The most effective treatment strategy for avulsion fractures of the ischial tuberosity is unknown. Eberbach et al.2 conducted a meta-analysis of 14 studies comprising 596 patients with pelvic apophyseal avulsion fractures. The authors recommended surgery for pelvic apophyseal avulsions with displacement >15 mm. The present patient chose nonsurgical treatment because it was expected that she would have a short recovery and rapid return to gymnastics. However, her return to full weightbearing at three months was longer than that reported by Eberbach et al.,2 who found a mean time to full weightbearing of 4.9 weeks (range 3–6 weeks) after nonoperative treatment. They also reported that the time to return to preinjury-level sport was 3.1 months (range 2–6 months) with nonoperative treatment and 2.4 weeks (range 1–6 months) after surgical treatment. In contrast, this patient required 12 months to recover fully from this injury.
The atypical presentation of chronic pain preceding an avulsion fracture of the ischial tuberosity and delayed recovery in this patient may be attributed to her history of GHD. Previous studies have reported on the adverse effects of GHD on bone metabolism and fracture healing.4,5 Other factors associated with stress fractures in female athletes include the concomitant conditions of amenorrhea, osteoporosis, and eating disorders.6 Although this patient did not have a history of eating disorder, she had a history of delayed menarche and secondary amenorrhea and a younger bone age than chronological age, which is common in competitive gymnasts. Estrogen plays an important role in the physiology of bone marrow density (BMD) and bone formation as it inhibits bone remodeling and bone resorption.7 In an estrogen-deficient state, BMD is decreased, thus leading to an increased risk of fragility fracture.6 Several other factors may be responsible for delayed recovery and return to play in athletes after injury; these include the use of a generalized, one-size-fits-all return-to-play protocol rather than an individualized approach based on sport and injury; poor communication between treating physician and trainers; and psychological factors such as anxiety, fear of decreased performance, and fear of reinjury.8,9
CONCLUSION
The authors report an avulsion fracture of the ischial tuberosity in a female gymnast with GHD who had a delayed recovery after nonoperative treatment. This case highlights the importance of a comprehensive evaluation, including for possible endocrine disorders, in adolescent athletes presenting with avulsion fracture of the pelvis including those of the ischial tuberosity.
Acknowledgment
For their editorial assistance, we thank Jenni Weems, MS, Kerry Kennedy, BA, Denise Di Salvo, MS, and Rachel Box, MS, in the Editorial Services group of The Johns Hopkins Department of Orthopaedic Surgery.
Conflicts of interest and source of funding
None.
This study is exempt from institutional review board approval.