INTRODUCTION
Epidemiological studies of injury and illness in sports are essential to protect the health of athletes.1 Definitions and methods of investigating the magnitude of injuries and illnesses have been published in consensus statements for specific sports2–4 and multi-sport events by the International Olympic Committee.1,5 The following injury and illness definitions are recommended: all physical complaints regardless of their consequences (any complaint definition), injuries or illnesses leading to the athlete seeking attention from a qualified medical practitioner (medical attention definition), and injuries or illnesses leading to the athlete being unable to complete the current or future training session or competition (time loss definition).1,6,7 To date, most injury surveillance studies have used time loss, the narrowest of all consensus-recommended definitions.8–10 However, this approach underestimates the full impact of overuse injuries because athletes often continue to participate in training and competitions despite persistent problems.11,12 To address these challenges, Clarsen et al.6 developed the Oslo Sports Trauma Research Center (OSTRC) Overuse Injury Questionnaire (OSTRC-O) in 2013 to record the extent of overuse injuries based on any complaint. Subsequently, the Oslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H) was developed in 2014 to record not only overuse injuries, but also traumatic injuries and illnesses.13
Several authors have investigated the efficacy of the new surveillance methods in comparison with the traditional method, which uses the time loss definition.6,14 Clarsen et al.6 reported that the OSTRC-O captured 10 times more overuse injuries than the traditional method, with 75% rather than 11% of the athletes affected during the study period. Weiss et al.14 assessed professional basketball players throughout one season using the OSTRC-O, and reported 6.5 times more overuse injuries than were reported with the traditional method. Thus, while the efficacy of the new surveillance methods has been examined for overuse injuries, they have not been compared with the traditional surveillance method for other health problems, such as traumatic injuries or illnesses.
The OSTRC questionnaires, OSTRC-O and OSTRC-H, were updated in 2020 to the OSTRC-O2 and OSTRC-H2, respectively.12 These questionnaires have been translated into several languages and have been adopted in both sports injury research and clinical environments.7,12,15–19 It is therefore crucial to distinguish the differences between the new and the traditional methods, not only for overuse injuries, but also for other health problems. The purpose of this study was to investigate the new surveillance method developed by the OSTRC, which is based on any complaint definition (new method), to identify health problems compared with the traditional surveillance method, which is based on time loss definition. It was hypothesized that the new methods capture more health problems than the traditional method not only for overuse injuries, but also for traumatic injuries and illnesses.
METHODS
Participants and recruitment
The university coaches and athletic trainers for a male handball team, a female soccer team, and a female lacrosse team were approached. After presenting the purpose of the study, athletes from the three teams were recruited individually. The inclusion criteria were as follows: 1) at least 18 years old and 2) able to speak and understand Japanese.7,18 Athletes were included regardless of whether they had current or previous injuries.7,18 This study was approved by the Ethics Committee of Osaka Electro-Communication University. All participants signed a written informed consent form. All methods were performed in accordance with relevant guidelines and regulations.
All athletes from each invited team (male handball, n = 27 athletes; female soccer, n = 14 athletes; female lacrosse, n = 23 athletes) consented to participate in the study. Of these, two female lacrosse athletes stopped playing lacrosse during the study period and were thus excluded from the analyses. The demographics of the participants are summarized in Table 1.
Procedures
The study followed the participants prospectively for 18 weeks from April to August 2021. They were asked to complete the Japanese version of the OSTRC-H2 (OSTRC-H2.JP) weekly.7 The questionnaire was prepared using Google Forms, and the hyperlink was distributed via email.7 If no response was received from an athlete after two days at the end of each week, an automatic reminder email was sent.7 In parallel, each team’s athletic trainers registered injuries and illnesses using the traditional method, which is based on a time loss definition.14
Injury and illness registration using the new surveillance method
The OSTRC-H2.JP was used to record the athletes’ health problems based on any complaint.7 This questionnaire consisted of four key questions regarding the symptoms and consequences of injuries and illnesses during the previous seven days.7,12 In case of any health problems, the athletes were asked to define whether the problems were an injury or illness.20 They were further asked to classify any injury as a traumatic or as an overuse injury, and to disclose the body location. For an illness, they were asked to select the major symptoms that they experienced. For both injuries and illnesses, athletes also reported the number of days of complete time loss, which was defined as the total inability to train or compete.13 Based on the players’ responses to the four key questions, the severity score for each health problem was calculated on a scale of 0–100.13
An any complaint health problem was defined as a health problem sustained by an athlete during a match or training, regardless of whether it received medical attention or necessitated time loss from sports activities.2,21 An illness was defined as a health complaint or disorder that is unrelated to an injury.1 An injury was defined as tissue damage or other derangement of normal physical function due to participation in sports, resulting from the rapid or repetitive transfer of kinetic energy.1 An injury was further classified as a traumatic or overuse injury; a traumatic injury was defined as caused by a single, clearly identifiable energy transfer, and an overuse injury was defined as caused by multiple accumulative bouts of energy transfer without a single, clearly identifiable event responsible for the injury.1,12,13,21
Injury and illness registration using the traditional method
The athletic trainers were asked to register health problems based on the time loss definition.6,14 For each injury, the registration form requested information about whether it was a traumatic or overuse injury, the injury location, the type of injury, the number of time loss days, and the diagnosis. For an illness, the form requested information about major symptoms, the number of time loss days, and the diagnosis. The severity of each health problem was classified as minimal (1–3 days), mild (4–7 days), moderate (8–28 days), or severe (>28 days) based on the number of time loss days.22,23
A time loss health problem was defined as a health problem sustained by an athlete during training or a match that caused the athlete to be unable to participate fully in future training or matches.2 Both surveillance methods used the same definitions of injury, illness, traumatic injury, and overuse injury.
Statistical analysis
The participants’ basic information was presented as the mean and standard deviation. The weekly response rate of the OSTRC-H2.JP was presented as a percentage and 95% confidence interval (95% CI) for all athletes and each team. The prevalence of health problems based on the OSTRC-H2.JP responses was calculated weekly by dividing the number of athletes reporting any type of problem by the number of questionnaire respondents.6,12,13
To assess the differences between data collected by the new and traditional surveillance methods, the numbers of health problems were calculated and compared.6,14 Statistical analyses were performed using Microsoft Excel for Mac (version 16.54, Microsoft Corporation, Redmond, WA, USA) and SPSS (version 26.0, IBM Corporation, Armonk, NY, USA), with the significance level set at p < 0.05.
RESULTS
The new surveillance method
During the 18 weeks, the average weekly response rate to the OSTRC-H2.JP among all participants was 82.1% (95% CI, 79.8–84.3); responses were provided by 72.9% (95% CI, 68.9–76.8) of the male handball team, 90.1% (95% CI, 86.4–93.8) of the female soccer team, and 88.6% (95% CI, 85.4–91.8) of the female lacrosse team.
From the responses to the OSTRC-H2.JP, 120 health problems were identified in 48 athletes (77.4%), of which 106 were injuries and 14 were illnesses (Table 2). Of these injuries, 64 were classified as traumatic injuries and 42 as overuse injuries. The average weekly prevalence of health problems was 31.2% (95% CI, 28.2–34.2) among all three teams. The average weekly prevalence of injuries and illnesses was 28.0% (95% CI, 25.1–30.9) and 3.8% (95% CI, 2.6–5.1), respectively. The average weekly severity score for health problems was 56.1 (95% CI, 54.7–57.6). The severity score for injuries was 51.6 (95% CI, 50.1–53.2), and the severity score for illnesses was 81.0 (95% CI, 72.4–89.7). Table 3 shows the average weekly prevalence and the severity scores of health problems during the course of the study.
The traditional surveillance method
A total of 39 health problems that resulted in time loss were identified from 31 athletes (50.0%) by athletic trainers from all three teams (Table 2). Of these, 34 were classified as injuries and five as illnesses. Among the injuries, there were 26 traumatic injuries and eight overuse injuries. The most affected body parts were the ankle (n = 11), the knee (n = 7), and the lumbo-sacral spine/buttock (n = 5) (Table 4).
Comparison between the new and traditional surveillance methods
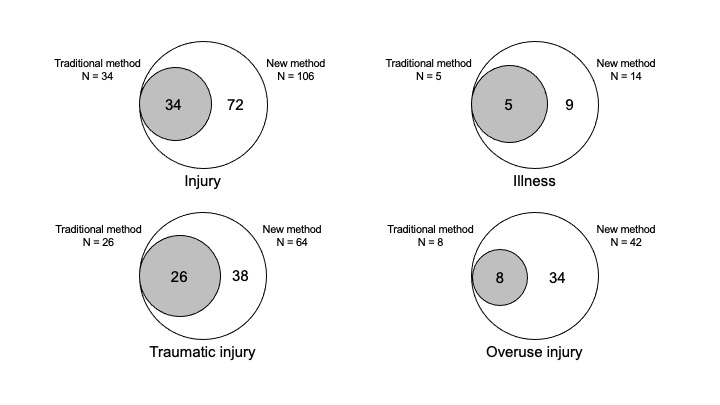
Throughout the study period, the new method recorded 3.1 times more health problems than the traditional method (new method: n = 120, traditional method: n = 39). These health problems were reported by 48 athletes (77.4%) using the new method and 31 athletes (50.0%) using the traditional method. For injuries and illnesses, the new method found 3.1 times more injuries (new method: n = 106, traditional method: n = 34) and 2.8 times more illnesses (new method: n = 14, traditional method: n = 5) than the traditional method. For injuries, the difference between methods was greater for overuse injuries (new method: n = 42, traditional method: n = 8) than for traumatic injuries (new method: n = 64, traditional method: n = 26). The differences between the new and the traditional method are shown in Table 2 and Figure 1.

Among injuries, the greatest difference between the new and traditional methods was for the head/face (6.0 times), followed by the shoulder (4.0 times) and the hand (4.0 times) (Table 4).
DISCUSSION
In this study, Japanese athletes were prospectively followed to assess differences in the number of health problems identified with the new method, which used an any complaint definition, and the traditional method, which used a time loss definition. The new method recorded more than three times as many health problems as the traditional method. Overuse injuries were identified as much as five times more often with the new method compared than with the traditional method.
Throughout the study, 120 health problems were identified using the new method, which was 3.1 times more than when using the traditional method. Among the health problems, the differences between the two methods were similar for injuries and illnesses. A study investigating the characteristics of injuries and illnesses among elite Norwegian athletes using the new method reported that out of 262 recorded injuries, 124 injuries resulted in time loss.13 This indicates that 2.1 times more injures were identified when using the any complaint definition than when using only the time loss definition.13 Although this is the first study to investigate differences between the new and traditional methods for determining health problems, not only for overuse injuries, but also for traumatic injuries and illnesses, the results obtained from this study are comparable to those of previous studies on both injuries and illnesses.13
The differences in injuries identified when using the new and the traditional methods were greater for overuse injuries (5.3 times) than for traumatic injuries (2.5 times). Overuse injuries are caused by repeated microtraumas without a single, identifiable event, and in many cases, do not result in time loss with absence from training or competition.11,12 Symptoms such as pain or functional limitation often appear gradually and may be transient; thus, it is likely that at least in the early stages, the athlete will continue to train and compete despite having overuse conditions.12 In fact, the severity scores for overuse injuries in this study were significantly lower than those for traumatic injuries and illnesses, and overuse injuries were less likely than traumatic injuries and illnesses to be accompanied by an absence from training or competition.
The difference between the two methods among overuse injuries in this study was similar to that of for targeted male professional basketball players,14 but lower than that of for targeted Norwegian athletes.6 Weiss et al.14 examined overuse injuries in professional basketball players using the new and the traditional methods, and showed that the new method recorded 6.5 times more overuse injuries than the traditional method. Clarsen et al.6 also investigated overuse injuries using both methods, and found that the new method identified 10.1 times more overuse injuries than the traditional method. The study included athletes participating in handball, floorball, volleyball, cycling, and cross-country skiing.6 While the majority of participants (66.5%) were involved in non-contact sports such as volleyball, cycling, and cross-country skiing,6 the majority of participants in our study (66.1%) were involved in contact sports such as handball and soccer. It has been reported that overuse injuries occur more frequently in non-contact sports than in contact sports.24,25 Hence, it is possible that the differences between the previous6 and current study are due to the characteristics of the sports in which the athletes participated.
This is the study to investigate the differences between quantification of health problems, such as traumatic injuries and illnesses, by the new and traditional surveillance methods. The study does have some limitations. First, as the participants from only three university teams were enrolled; thus, it was not possible to extract a sufficient numbers of health problems for detailed examination of the differences between their quantification by the new and traditional methods in terms of the locations of injuries and illnesses. Additionally, although the questionnaires are intended to be used for a variety of sports, only responses from athletes participating a few sports (handball, soccer, and lacrosse) were analyzed. In particular, the results might differ between contact and non-contact sports. Furthermore, the athletes self-reported their injuries and illnesses in the new method. As most athletes do not have adequate medical knowledge, erroneous information regarding their conditions might have been reported. To minimize erroneous responses, the athletes were familiarised with the definitions of health problems during the pre-study meeting.
CONCLUSION
This study found that the new surveillance method, which uses an any complaint definition, could capture more than three times as many health problems, including traumatic injuries, overuse injuries, and illnesses, as the traditional method, which uses a time loss definition. In particular, the methods differed more in their quantifications of overuse injuries than they did for traumatic injuries.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.