BACKGROUND
Acetabular dysplasia, defined as a bony abnormality of the acetabulum with abnormal coverage of the femoral head, is a well-recognized cause of hip pain in young adults.1,2 This structural abnormality leads to a decrease in contact area of the hip, excessive wear on the articular cartilage, and degenerative changes of the acetabular labrum.3–5 Acetabular dysplasia can lead to severe pain, disability, and early onset arthritis without appropriate management.6,7 Treatment of acetabular dysplasia with a periacetabular osteotomy (PAO) has been shown to improve long-term outcomes and is considered the gold standard for symptomatic hip dysplasia.8–11 Although post-operative rehabilitation is important to help patients return to prior level of function, there a paucity of research supporting post-operative rehabilitation guidelines following a PAO.
Inadequate rehabilitation after PAO may lead to poor outcomes, which may include prolonged impairments in hip strength. It is well accepted that adequate strength of the lumbopelvic stabilizers is necessary to provide stability to the hip joint and maintain appropriate pelvic positioning during weight-bearing tasks.12,13 While improvements in isometric hip flexion and abduction are observed at one year following a PAO, strength values were shown to remain 13-34% lower than that of healthy controls.14 Other studies have reported similar improvements in hip abductor, hip flexor, and hip extensor strength values one year following a PAO when compared to pre-operative values, but no comparison was done to healthy controls.15,16 Prolonged impairments in hip strength may lead to decreased performance on functional tasks as hip abductor weakness is associated with impaired hip kinematics during a single-leg squat task when compared to healthy controls.17
Understanding important rehabilitation parameters, including early weight-bearing and range of motion (ROM) precautions, exercise progression throughout recovery, and metrics for clearance to return-to-run and return-to-sport, is crucial to maximize patient recovery following a PAO. The purpose of this study is to present expert-driven rehabilitation guidelines to reduce practice variation following a PAO.
METHODS
Delphi Panel
The expert panel in PAO rehabilitation consisted of sixteen physiotherapists who were purposefully sampled from geographically different institutions spread throughout the United States and Canada. Participants were selected based on multiple criteria, including (1) treating at least 10 patients following PAO per year, (2) identified by high-volume hip preservation surgeons as an expert in the rehabilitation of PAO patients, and/or (3) experts in rehabilitation of non-arthritic hip disorders. All members consented to participate in this IRB exempted study, and participants were blinded to each other for the entire duration of the study.
Delphi Structure and Data Collection
A three-step classic Delphi method was used to establish consensus techniques in the diagnostic evaluation of pediatric ACL injuries.18 Consensus was defined a priori as ≥75%, which is moderate per standard Delphi methods to account for expected variation in a content area with little available evidence.19 Definitions of consensus level are commonly based on accepted standards such as voting percentages (simple majority, two-thirds majority, absolute majority) and a supermajority was deteremine most appropriate for this study.19 This study had the dual objective of achieving consensus and, equally importantly, understanding areas where consensus could not be reached and reasons for disagreement.
Panelists were presented with three iterative rounds of surveys. Questionnaires for rounds one through three were distributed online via an emailed link with responses de-identified for analysis. For each survey round, analysis of the participants’ responses was completed by two study members (AD and KE). Any disagreements were resolved by a third team member (MM).
In the first survey round, panelists were presented with eleven free-response questions regarding their physical rehabilitation practice:
-
What weight-bearing precautions do you use? What objective measures do you use to discharge crutches?
-
What range of motion precautions do you utilize postoperatively? How long do you follow these precautions? When do you expect the patient to achieve full range of motion?
-
How do you begin to rehabilitate the hip flexor complex? When do you begin to rehabilitate the hip flexor complex?
-
Do you limit active long lever hip flexion? If so, how long?
-
What exercises do you utilize to improve lower extremity lumbopelvic control?
-
What exercises do you utilize to strengthen the gluteus medius? What exercises do you avoid when strengthening the gluteus medius?
-
What exercises do you utilize to facilitate lumbopelvic neuromuscular control? When do you begin these exercises?
-
When do you initiate end range stretching?
-
When do you begin low level cardiovascular exercise? (ie. upright stationary biking and elliptical)
-
What objective measures do you utilize to determine if a patient is ready to begin running?
-
What criteria do you utilize to determine if a patient is ready to return to full participation in sports?
Panelists provided detailed descriptions of treatment parameters for each question. Responses were collected and coded for common thematic content. Responses reported by ≥50% of panelists were considered modal, while responses reported by ≥25% of panelists formed a second tier of responses.
In round two, panelists were presented the original questions along with the modal response derived from the first round of responses. Panelists were asked to agree or disagree with the modal response, and those who disagreed were allowed to add or subtract items. The second-tier responses were included as potential additions, but free text addition was also permitted. Resulting responses were again coded for thematic content and modal responses were adjusted as appropriate.
In round three, panelists again received ten of the eleven questions with revised modal and second-tier responses. Similar to round two, panelists were asked to agree or disagree with the modal response, and those who disagreed were allowed to add or detract items. Disagreement prompted a free-response box for the panelist to explicitly detail their disagreement. Analysis of the third-round data provided concepts for which consensus had been gained as well as rationale for disagreement.
RESULTS
The expert panel in this study consisted of sixteen physiotherapists who were identified as an expert in PAO rehabilitation. Overall, 100% participation was achieved with all sixteen therapists completing all three Delphi rounds. The expert panel received eleven questions covering a variety of topics related to rehabilitation following a PAO, and 100% consensus was achieved for all topics of interest by the third Delphi round.
Weight-Bearing Precautions
For weight-bearing precautions that should be utilized immediately following a PAO, 15/16 (94%) panelists agreed that weight-bearing should be limited to 25%, foot-flat weight-bearing for 6-8 weeks. It was noted that concomitant procedures, such as hip arthroscopy or microfracture, may prolong these recommendations.
Discharging Crutches
For objective measures to discharge crutches after 6-8 weeks of protected weight-bearing, 16/16 (100%) panelists agreed that observed gait deviations and surgeon clearance should be utilized. Examples of gait deviations listed in the question included Trendelenburg gait, abductor lurch, and antalgic gait.
ROM Precautions
For ROM precautions immediately following a PAO, 13/16 (81%) panelists agreed that flexion should be limited to 90 degrees and external rotation limited to 20 degrees in 90 degrees of flexion. The 13 panelists agreed that these precautions should be maintained for 4-6 weeks. It was noted that concomitant procedures, such as hip arthroscopy or microfracture, may prolong or alter these recommendations to include limitations in hip extension and hip internal rotation.
Two dissenting panelists had different points of contention. One panelist felt that flexion should be limited to 70 degrees for three weeks, and then limited to 90 degrees for the following week along with avoidance of rotation of the femur in flexion and avoidance of hip extension until the fourth week. The second panelist stated that there should be no flexion past 90 degrees and no external rotation in any range. For achieving full ROM following an isolated PAO, 16/16 (100%) panelists agreed that the patient should achieve full hip ROM by 12-16 weeks (3-4 months).
For the initiation of end range stretching, 15/16 (94%) panelists agreed that it can begin somewhere between 8-12 weeks post-operatively as tolerated. The one dissenting panelist stated that it should only occur as needed after 16 weeks post-operatively.
Protection of the Hip Flexor Complex
For rehabilitation of the hip flexor complex following a PAO, 16/16 (100%) panelists agreed to the general protocol:
-
Long lever active hip flexion in supine should be limited for 8-12 weeks following an isolated PAO.
-
Initiation of therapeutic exercise targeting the hip flexor complex should begin between 4-8 weeks as tolerated by pain.
-
Active assistive ROM (AAROM), heel slides, and/or isometrics should be utilized to initiate rehabilitation of hip flexor complex, progressing as tolerated
Lumbopelvic and Posterior-Lateral Hip Strengthening
For the initiation of lumbopelvic control following a PAO, 16/16 (100%) panelists agreed that a core progression should include supine and quadruped activities.
For strengthening of the gluteus medius following a PAO, 15/16 (94%) panelists agreed to the general guidelines:
-
In general, gluteus medius strengthening should begin with isometrics progressing to non-weight bearing (NWB) progressive resistance exercises followed by double and single leg weight bearing exercises. Other positions and different lever arms can be utilized to progress strengthening exercises.
-
Exercises that increase anterior hip activation/pain (ie. hip flexor and tensor fascia lata compensation) should be avoided when beginning gluteus med strengthening.
The dissenting panelist stated that strengthening of the gluteus medius should begin with isometric strength exercises, followed by functional movements, then progress to weight-bearing exercises.
Lumbopelvic and Lower Extremity Neuromuscular Control
For improving lower extremity neuromuscular control following a PAO, 14/16 (88%) panelists agreed to the general guidelines:
-
Double and single leg exercises in the closed chain challenging frontal plane control and femoral IR control (valgus).
-
These exercises can begin in NWB as the patient tolerates and should progress to WB at six weeks or immediately after the patient is cleared for WB.
Only one of the dissenting panelists provided a retort, stating initiation of lower extremity neuromuscular control should begin in passive weight-bearing positions, such as quadruped or tall kneeling prior to double or single leg.
Return to Sport Criteria
For beginning low level cardiovascular exercise following a PAO, 13/16 (81%) panelists agreed to the general guidelines that patients may begin upright stationary biking 6-8 weeks post-operatively and begin using an elliptical by 10-12 weeks. Only two of the three dissenting panelists elaborated on their disagreement. One of the panelists stated that stationary biking may begin at two weeks with no resistance, followed by walking in the pool at four weeks. The other panelist stated that stationary biking may begin at two weeks maintaining 90-degree flexion precautions, and the elliptical may begin when the patient is walking normally, progressing through strength exercises, and can bike for 30 minutes.
For objective measures to begin a running progression, 14/16 (88%) panelists agreed to the general guidelines:
-
Normalized hip strength (with a focus on glute med and ER strength)
-
Performance on functional tasks (SL squat, Y-Balance, etc)
The two dissenting panelists agreed to the above guidelines but thought that quad/hamstring strength and surgeon clearance with radiographic support were needed to progress to running as well.
For objective criteria required to return to sport, 16/16 (100%) panelists agreed to the guidelines:
-
Involved: uninvolved hip abductor strength ratio of >80%.
-
Performance on functional tasks (single leg squat, Y-balance).
-
Performance on sport specific drills chosen based on patient specific demands
DISCUSSION
This Delphi study was performed to establish consensus among physiotherapy experts for post-operative rehabilitation guidelines following a PAO. No studies currently exist supporting specific weight-bearing and ROM precautions, therapeutic exercise prescription, or metrics for clearance to return-run and return-to-sport. Therefore, the Delphi method was utilized to generate expert opinion in a content area where evidence is lacking. Across all three rounds of this study, 100% participation was achieved from the 16 physiotherapists and consensus was achieved across all domains. These post-operative guidelines may reduce unwanted practice variation and help patients achieve more normal hip strength values to maximize functional potential and minimize reinjury risk. A summary of recommendations can be found in Table 1.
Weight-Bearing Precautions
Consensus Point: Patients should ambulate with 25% foot-flat weight-bearing through the affected lower extremity for 6-8 weeks following a PAO. Crutches can be discharged after radiographic evidence of bony healing and a normalized gait pattern.
In the immediate post-operative phase, modified weight-bearing is utilized to allow for bony healing. Post-operative stress fractures have been reported as a complication in the literature with an incidence between 2-18.4%.20–22 Early weight-bearing, pubic non-union, a larger preoperative deformity, advanced age, and a higher post-operative center-edge angle have been identified as possible factors for developing a stress fracture following a PAO. Ito et al.23 reported a higher incidence of postoperative fractures of the ischial ramus and posterior column with full weight-bearing immediately following surgery compared to two months of modified weight-bearing. In a normal pelvis, load transfer is higher through the superior pubic ramus as compared to the inferior pubic ramus. However, following a PAO, increased load transfer occurs through the inferior pubic ramus, ischium, and posterior column.24 These changes in load transmission patterns increase stress and strain through these bony structures and potentially result in a post-operative stress fracture. Therefore, modified weight-bearing in the early post-operative phase is indicated. The current results are consistent with these recommendations as 15/16 participants recommend 25% foot-flat weight-bearing until 6-8 weeks at which point weight-bearing can be progressed only if the patient demonstrates radiographic evidence of bony healing and a normalized gait pattern. It was noted that concomitant procedures, such as hip arthroscopy or microfracture, may prolong these recommendations to protect the healing capsuloligamentous structures and joint cartilage.
Range of Motion Precautions
Consensus Point: Hip flexion and external rotation ROM should be protected for 4-6 weeks followed by progressive, pain-free restoration of ROM. End range stretching can be initiated between 8-12 weeks as tolerated with full ROM achieved by 12-16 weeks post-operatively.
Restoration of hip range of motion is essential to allow for participation in both daily and recreational activities. Similar to a hip arthroscopy, end ranges of motion should be protected in the early post-operative period. This includes end range flexion, which approximates the femur and the acetabulum, and hip external rotation, which stresses the anterior hip capsule. After a period of protected motion allowing for a reduction in inflammation and bony healing, a gradual approach to improving range of motion is essential to limit joint irritation. Consensus regarding all passive and active ROM precautions was achieved as panelists agreed that hip flexion and external rotation ROM should be limited for 4-6 weeks, with normal passive hip motion being achieved by 12-16 weeks. Panelists agreed the upright stationary bike can be initiated between 6-8 weeks and the elliptical trainer between 10-12 weeks to facilitate early-stage passive range of motion as well as cardiovascular endurance. In the setting of concomitant procedures, such as a hip arthroscopy, panelists indicated that ROM precautions may be altered to include extension or internal rotation to further protect healing soft tissue structures.
Protection of the Hip Flexor Complex
Consensus Point: Progressive loading of the hip flexor complex should be done cautiously, with isometrics and short-lever active assistive hip flexion exercises beginning between 4-8 weeks as indicated by pain. Long-lever active hip flexion should be avoided for 8-12 weeks following a PAO.
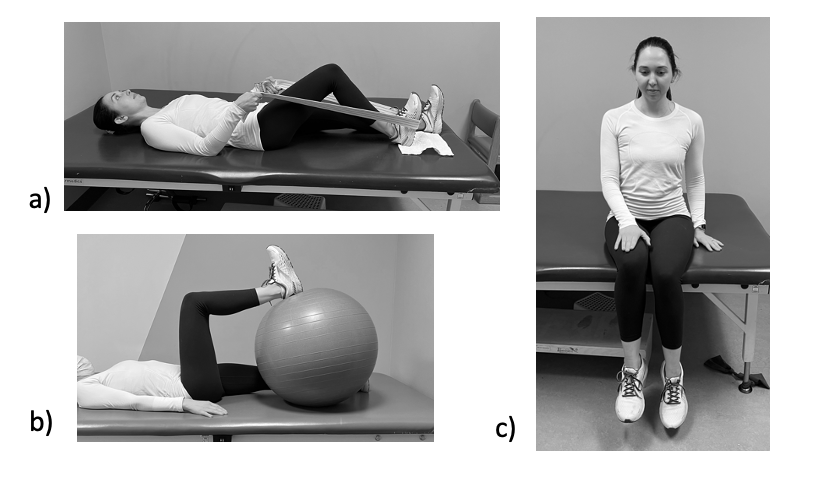
The iliopsoas courses directly anterior to the femoral head and acts as a secondary stabilizer to the hip joint.25 In the setting of hip dysplasia, the iliopsoas may overcompensate for the lack of bony stability and result in tendinous overload, inflammation, and pain.26,27 Furthermore, anecdotal evidence has linked weakness of the gluteus medius, which is a common finding in patients with dysplasia and a consequence of a PAO, to iliopsoas tendinitis.28 Following a PAO, the iliopsoas can impinge on the pubic osteotomy further predisposing these patients to hip flexor irritation.29 Extreme care should be taken to avoid additional hip flexor irritation in the early post-operative phase and therefore toe touch weight-bearing or non-weight-bearing during gait should be avoided. Instead, patients should ambulate with a foot-flat gait pattern to reduce activity of the iliopsoas. Progressive isometrics and short lever active assistive hip flexion exercises are recommended at 4-8 weeks to progressively load the iliopsoas tendon while all long lever hip flexion activities should be avoided for 8-12 weeks post-operatively. Recommended exercises to progressively load the hip flexor can be found in Figure 1. Additionally, strengthening exercises for the gluteus medius that also activate the anterior hip should be avoided, especially in the setting of iliopsoas pain. Philippon et al.28 reported sidelying hip abduction in external rotation and the clamshell exercises demonstrated considerable EMG activation of hip flexor. These findings support a recommendation that these exercises should be avoided or prescribed with caution in the presence of anterior hip pain.
_heel_slides__b)_physioball_hip_flexion__.png)
Lumbopelvic and Posterior-Lateral Hip Strengthening
Consensus Statement: Lumbopelvic strengthening should begin in the early post-operative phase in non-weight-bearing and progress to double and single leg weightbearing exercises as tolerated.
The relationship with lumbopelvic and posterior-lateral hip muscle function to lower extremity injury has been demonstrated in the literature.30–35 One-year following PAO, patients demonstrate improvements in isometric hip flexion and abduction strength, however, these values were shown to remain 13-34% lower than that of healthy controls.14 Other studies have reported similar improvements hip abductor, hip flexor, and hip extensor strength values one year following a PAO when compared to pre-operative values, but no comparison was done to healthy controls.15,16 Additionally, it has been well established that females exhibit less hip strength, particularly in their hip abductors and external rotators, compared to males.33,36 Given that hip dysplasia is more prevalent in females and lumbopelvic strength lags post-operatively, extensive lumbopelvic strengthening is crucial for improving hip joint mechanics and maximizing outcome. Snyder et al.37 reported a strengthening program targeted at the hip abductors and external rotators altered lower extremity joint loading. In patients with hip dysplasia, strengthening of the hip abductors was shown to reduce dynamic instability during ambulation.38 Without normalization of strength, muscle imbalances in the hip and core can lead to altered force couple relationships and faulty joint arthrokinematics.39,40
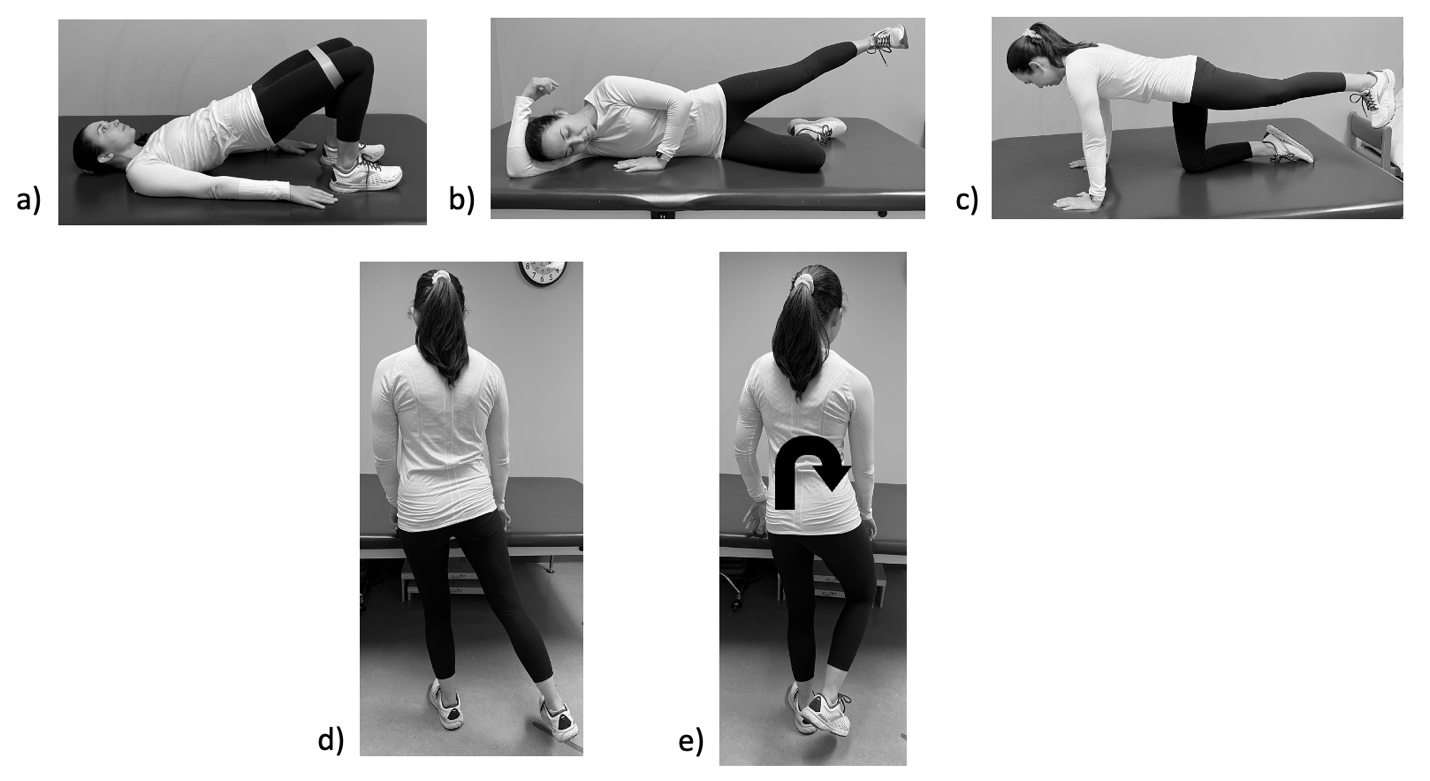
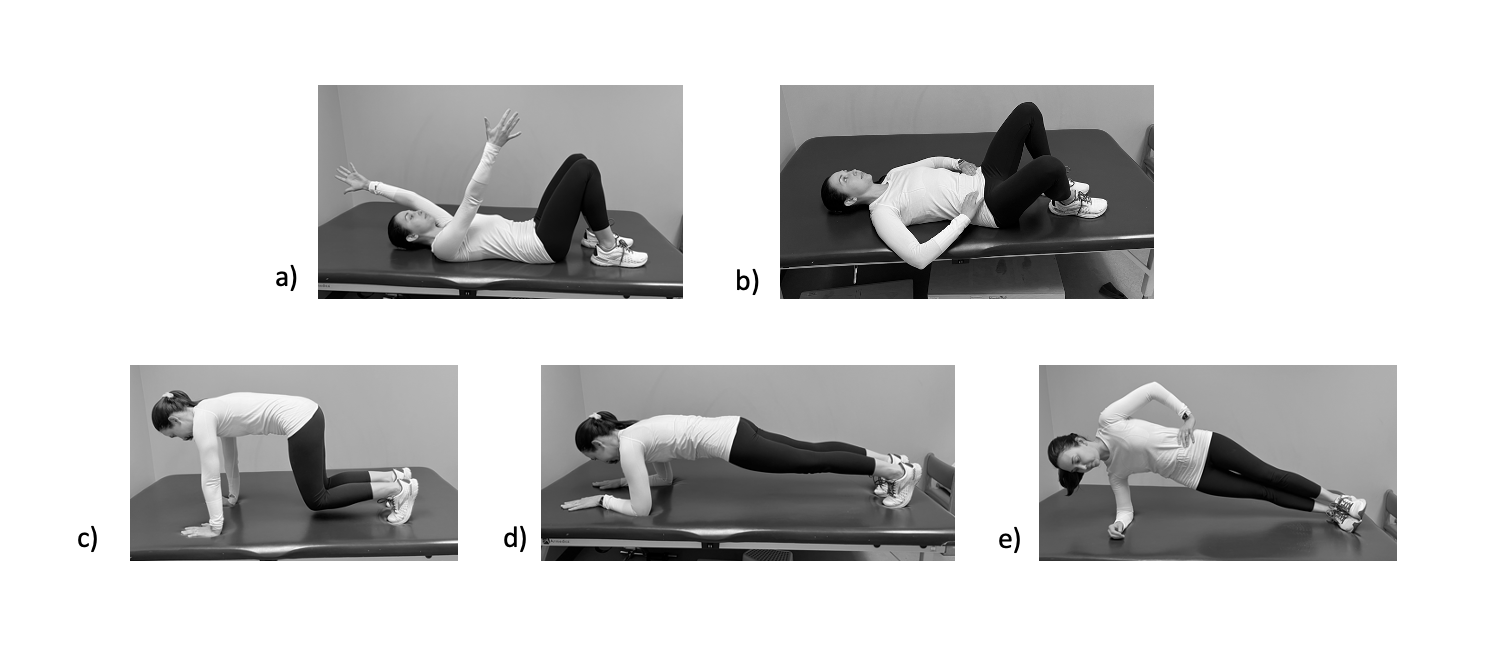
A graded approach to therapeutic exercise allows for improvements in strength while minimizing musculotendinous overload and joint irritation. This is an important concept following a PAO as the reorientation of the acetabulum affects the torque-generating capacities of the surrounding musculature which could may affect muscle strength and activation.41,42 Panelist consensus indicated that strengthening of the core muscles and gluteus medius should begin with non-weight-bearing isometrics and progress to single leg weight-bearing exercise as tolerated. The gluteus medius has been shown to demonstrate high EMG values in a single leg stance position.43,44 Therefore, when appropriate, exercises performed in a single-leg stance position should be a focus of post-operative rehabilitation to increase hip abductor strength. Recommended lumbopelvic strengthening exercises can be found in Figures 2 and 3.
_double_leg_brid.png)
_hooklying_transversus_abd.png)
Lumbopelvic and Lower Extremity Neuromuscular Control
Consensus Statement: Lumbopelvic neuromuscular control exercises should begin in non-weight-bearing in the early post-operative phase with progression to weight-bearing exercises at 6-8 weeks or immediately after the patient is cleared for weight-bearing. In weight-bearing, exercises should consist of double and single leg exercises challenging frontal plane and femoral internal rotation control.
Neuromusuclar control training is utilized to improve functional performance, lower extremity biomechanics, and muscle activation patterns. Decreased neuromuscular control of the lumbopelvic region leads to uncontrolled trunk movement and lower extremity valgus, increasing the risk of lower extremity injury.45,46 During landing and pivoting movements, females demonstrate increased lower extremity valgus resulting in increased load through the lower extremity.47–51 The gluteus medius, gluteus maximus, and deep external rotators are responsible for maintaining stability of the pelvis in the closed chain while the core is responsible for providing a stable base for force transfer between the trunk and the lower extremity.39,52–56 The goal of rehabilitation is to improve dynamic stabilization of the hip, especially during single-leg weight-bearing tasks when loads within the hip are the highest.12,13,57 Myer et al.58 reported a 15% increase in hip abduction strength in healthy individuals with a 10-week targeted neuromuscular control training compared to no increase in strength in the control group. Similarly, Hewett et al.59 reported a significant improvement in hip external rotation moments and moment impulses, increased peak trunk flexion, and decreased peak trunk extension following a 10-week targeted neuromuscular control training program.
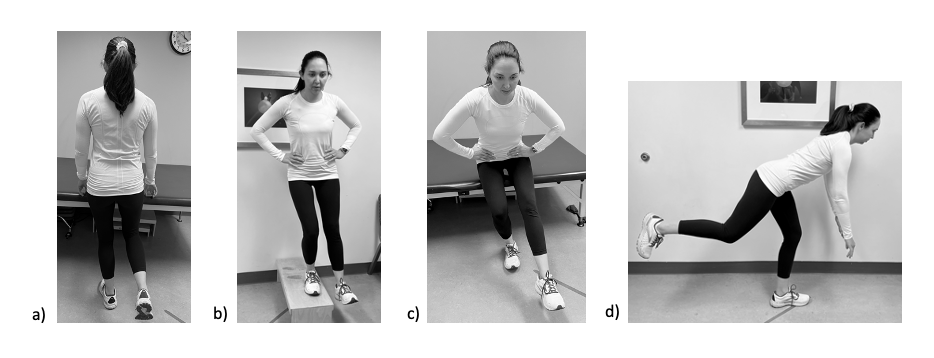
Panelists agreed that an emphasis should be placed on lumbopelvic and lower extremity neuromuscular control beginning in the immediate post-operative phase. Early education on the importance of the transversus abdomonis, which contributes to spinal stability during weight-bearing tasks, will set the foundation for appropriate lumbopelvic control for the later stages of recovery.60,61 These exercises should begin in supine during the immediate post-operative phase progressing to quadruped, tall-kneeling, and double and single leg stance as indicated. Recommended lumbopelvic and lower extremity neuromuscular control exercises can be found in Figure 4.
_s.png)
Return to Sport Criteria
Consensus Statement: The upright stationary bike can be initiated between 6-8 weeks and the elliptical trainer between 10-12 weeks to facilitate early-stage cardiovascular endurance, as well as passive range of motion of the hip. Panelists recommend utilizing a combination of strength, endurance, and functional performance measures during return to play testing, including but not limited to hip abductor to adductor strength ratios, the Y-Balance test, and various hop tests.
Return to sport is a goal of many patients undergoing a PAO, as these patients tend to be young, active individuals. Heyworth et al.62 found 80% of patients undergoing PAO procedures returned to play at a median of nine months post operatively with increased pain being the only independent predictor of delayed return. Of these patients, 73% returned to their previous level of sport. Takahashi et al.63 reported similar findings, with 72.2% of patients able to participate in both low and high impact sports following a PAO. It should be noted that no details were provided regarding rehabilitation protocols utilized in these studies. The importance of return to sport metrics to reduce reinjury rates has been well documented in the ACL literature, however, specific guidelines continue to remain elusive.64–69 Following hip arthroscopy, these guidelines are less defined with recommendations including the absence of pain and appropriate control during sport specific activities such as running, lateral agility, and single leg squats.70 These recommendations can serve as a guide when discussing return to sport following a PAO as none currently exist in the literature. Psychological readiness should also be considered during the return to sport phase as this may affect their ability to return to previous level of play and increase the risk of reinjury.71–74 A recent systematic review found positive psychological responses pertaining to motivation, confidence, and fear were associated with greater likelihood of returning to previous level of participation.73 It can be assumed that patients following a PAO will exhibit signs consistent with low confidence and fear given the longstanding nature of dysplasia symptoms and the extensive surgical procedure. These factors should be considered along with functional performance and strength measures when determining readiness to return to sport.
Panelists recommend utilizing a combination of strength, endurance, and functional performance measures during return to play testing, including but not limited to hip abductor/adductor strength ratios, single leg squats, and the star excursion balance test . Recommendations for objective measures for return to straight line running and return to full participation in sports can be found in Table 2.
Limitations
There are several limitations to our current study. There is a paucity of research supporting post-operative PAO rehabilitation guidelines. Ellis et al.75 published a rehabilitation protocol for use after concomitant PAO and hip arthroscopy, however, this Delphi study was focused on an isolated PAO. Therefore, initial study questions were generated by expert opinion which could result in bias. To minimize resultant bias in the modal responses, the authors recruited a diverse expert panel. It should be noted, however, that all panelists were from North America which may limit the international generalizability of our findings. Additionally, panelists completed all survey rounds on-line which does not allow for clarification or open discussion regarding survey items. Lastly, this Delphi study included recommendations pertaining to an isolated PAO, which does not cover the spectrum of possible concomitant procedures performed to address soft tissue injuries or revision procedures.
CONCLUSION
Although post-operative rehabilitation is important to help patients return to prior level of function, there a paucity of research supporting post-operative rehabilitation guidelines following a PAO. Inadequate rehabilitation after PAO may lead to poor outcomes, which may include prolonged impairments in hip strength. This Delphi study established expert-driven rehabilitation guidelines for use following a PAO. The standardization of rehabilitative care following PAO is essential for achieving optimal outcomes despite other factors such as geographical location and socioeconomic status. Further research on patient-reported outcomes is necessary to confirm successful rehabilitation following the guidelines outlined in this study.
Conflict of Interest Statement
The authors have no conflicts of interest.
Acknowledgements
We want to acknowledge all physiotherapists who put time and effort into answering all survey questions and provided feedback during this Delphi study. Their work was essential to creating this consensus statement.