


INTRODUCTION
Instrument-assisted soft tissue mobilization (IASTM) is a commonly utilized intervention for musculoskeletal pain and dysfunction.1–4 The use of instruments is thought to provide a mechanical advantage to transmit greater, and more controlled load to mobilize soft tissue restriction or myofascial adhesion than manual massage.1–3 The more targeted force transmission is thought to result in soft tissue healing, collagen repair, resolution of scar tissue, and connective tissue remodeling.1–7 Further, IASTM is also thought to minimize clinician fatigue and enhance clinician detection of soft tissue anomalies.1–7
Multiple theories regarding the mechanism of effect of IASTM have been proposed, with mechanical and neurophysiological theories often being cited. Mechanical theory advocates often suggest that IASTM provides pressure and shearing forces to release and address adhesions, fascial restriction, and scar tissue facilitated through the inflammatory phase of the tissue healing process.6–9 Neurophysiological theory advocates, in contrast, propose IASTM causes stimulation of both the high and low threshold mechanoreceptors.10–12 The stimulation also activates the ascending afferent pathways that signal the natural physiological response of the body, causing blood flow changes and mechanoreceptor activity after an IASTM session.10–12 The selected IASTM approach or tools may also activate different mechanoreceptors (e.g., Pacinian corpuscles, Meissner corpuscles, Merkle’s disks) based on force applied, instrument weight, bevel or angle degree, or stroke variations (e.g., stroke speed).10–12
Clinicians have several IASTM instruments and training programs available to them, including, but not limited to, Técnica Gavilán®, RockBlades®, Edge Mobility System™, Fascial Abrasion Technique™, and the Graston Technique®.2,7 Several IASTM companies offer training programs with specific protocols, while others do not promote specific protocols or require training for instrument purchase.2,7 Little is known regarding how differences in manufactured IASTM instruments (e.g., instrument weight, beveling, number of edges, etc.), variations in IASTM training, or proposed manufacturer IASTM treatment protocols influence force production during treatment or patient outcomes.2–7 The lack of evidence-based guidelines, inconsistencies in required IASTM clinician training prior to instrument purchase, irregularities across training programs, and variations within IASTM treatment variables (e.g., force applied, instrument weight, instrument bevel, treatment goals, etc.) may lead to inconsistencies in IASTM application in research and clinical practice.1,2,7
Currently, research is limited in determining the amount of force and the reproducibility of that force during the IASTM application. Researchers6,8,9,12–14 have more commonly quantified IASTM force application in animal model studies. Studies conducted on rodent ligaments with short durations of approximately 250-300 grams (g; ~2-3 newtons [N]) of downward force have demonstrated enhanced soft-tissue healing.8,9 Gehlsen, Gannon, and Helfst14 also reported short durations of increased forces ranging from 0.5N (50g) to 1.5N (150g) enhanced fibroblast proliferation. However, it is not well understood how the forces used in the animal model studies compare to IASTM forces used in clinical practice, how these published results have influenced clinical practice, or how different forces influence treatment outcomes.
To date, the IASTM forces used in human trials have been less commonly quantified or estimated, and the forces reported have varied more widely than those used in the animal model studies. Light force, as estimated by the weight of an IASTM tool (i.e., ~208g, ~2N) without assessment of the actual force applied during treatment, has been used as an estimate for pressure during treatment; the light pressure was concluded to have improved pain pressure threshold in participants with delayed onset muscle soreness.6 In contrast, Vardiman et al.13 documented force production and reported large treatment force ranges (mean and peak pressure) varying from 2-9N (200-900g) within a treatment session; the use of IASTM in this scenario did not result in significant changes in range of motion, maximum voluntary contraction peak torque, and change in inflammatory markers in healthy participants. As minimal research regarding force used during IASTM exists in human trials to guide evidence-based guidelines for IASTM application, clinicians may be challenged to select an appropriate treatment force and may rely on their IASTM training or personal preference to guide treatment application. Recently, IASTM trained clinicians indicated that it is common to deviate from the recommendations of their IASTM training or to not consider the amount of force applied during IASTM treatment.15 Thus, it may also be challenging to confirm that IASTM force application is consistent within a treatment session or across treatment sessions.
Currently, few researchers have examined the amount of force clinicians utilize while treating patients, the consistency of IASTM force application within or across treatments, or how IASTM force application consistency may vary by clinician experience. Given the lack of IASTM force research, the variability of forces reported in the literature, and the clinician-noted deviations from training recommendations, it is valuable to evaluate clinician-applied IASTM force and the reliability of those forces across treatment sessions. Therefore, the purpose of this pilot study was to assess the intra-clinician reliability of IASTM forces (i.e., mean normal force) during a simulated, one-handed stroke IASTM intervention among clinicians with different levels of IASTM and professional experience.
METHODS
Design
The University of Idaho Institutional Review Board approved the pilot study and informed consent was provided by participants prior to study participation. A repeated measures trial was conducted at a university research biomechanics laboratory. All participants were provided with an identical standardized treatment scenario and instructed to perform the IASTM treatment using the Técnica Gavilán® instrument Ala (Tracy, CA; Ala, mass: 196g) as they would in clinical practice. A total of 15 one-handed strokes were completed across two data collection days; the average normal forces (i.e., the average force perpendicular to the treatment plane from the beginning to end of a single stroke) in newtons (N) were recorded for each IASTM stroke applied.
Participants
This study included a convenience sample of ten participants (five females and five males; six certified athletic trainers and four athletic training students) who had completed at least one professional IASTM course prior to study participation. All participants had completed the introductory course offered by Técnica Gavilán®, while one of the participants had also completed additional IASTM courses (e.g., RockBlades® courses). Participants had a mean age of 32.60 ± 8.71 years and a mean IASTM experience of 3.78 ± 4.10 years.
Participant experience was classified into five categories: 1st Year Professional Student (i.e., student in their 1st year of professional program who completed their first IASTM course within the prior six weeks), 2nd Year Professional Student (i.e., student in their 2nd year of professional program with one year of IASTM experience after completing their first IASTM course), Early Career Clinician (i.e., credentialed clinician with less than five years of IASTM experience post-completion of their first IASTM course), Intermediate Experienced (Exp.) Clinician (i.e., credentialed clinicians with five to nine years of IASTM experience post-completion of their first IASTM course), and Established Clinician (i.e., credentialed clinician with 10 + years of IASTM experience post-completion of their first IASTM course).
Instrumentation
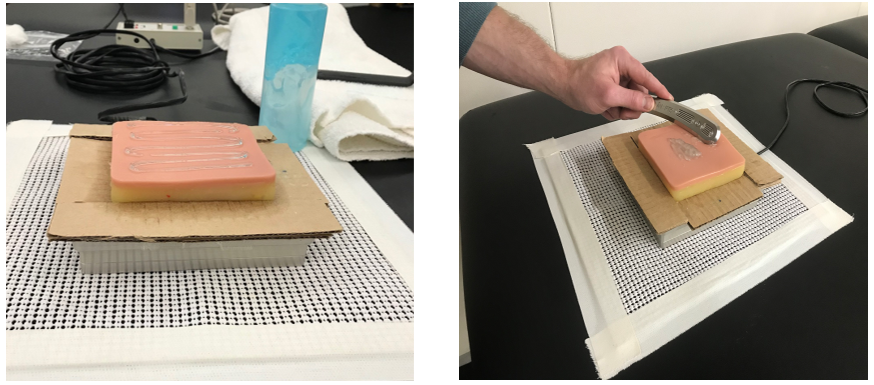
Participants applied IASTM forces to a skin simulant (Complex Tissue Model, Simulab Corporation©, Seattle, WA) of 1-inch thickness designed to replicate skin, subcutaneous fat, fascia, and pre-peritoneal fat that was attached to a 6"x6" force plate (HE6x6, AMTI©, Watertown, MA). The force plate was calibrated between each participant and raw data from the force plate were recorded at a rate of 500Hz using NetForce software (v. 3.5.3, AMTI©, Watertown, MA). Data were processed in MATLAB (v. 2019b, Natick, MS) and filtered using a 10Hz low-pass Butterworth filter to determine the beginning and end of each stroke. The skin simulant attached to a force plate was then stabilized on a treatment table for data collection (Figure 1).
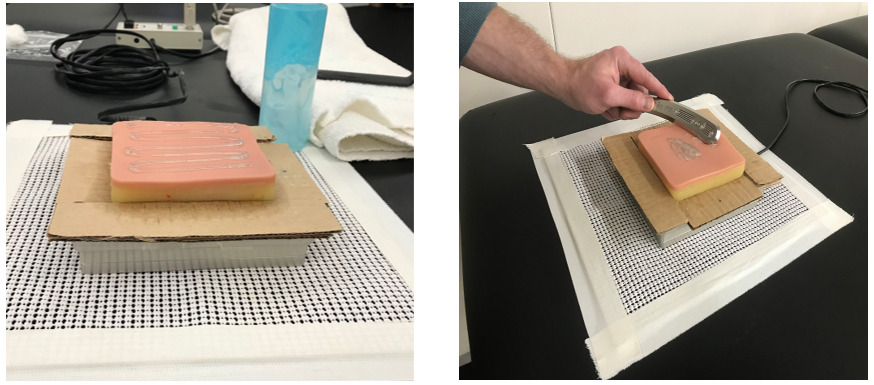
The Técnica Gavilán® instrument Ala has also been used in prior studies.1,2,7,16 The weight of the instrument is 196g. The Técnica Gavilán® instrument is a stainless-steel tool with a single beveled edge which allows unilateral strokes by the clinician (Figure 2). The same instrument was used for consistency among clinicians and sessions.
_(front___back).png)
Procedures
All participants completed a familiarization protocol (i.e., practiced five one-handed strokes with the instrument on the skin simulant) before beginning the testing protocol. Participants were allowed to add their desired amount of emollient to the skin simulant and to practice strokes on the simulant/force plate until the participant reported feeling comfortable applying an IASTM treatment on the apparatus. Participants were then provided with a standardized treatment scenario for the medial gastrocnemius: an otherwise healthy patient experiencing gastrocnemius tightness who they examined to confirm that an IASTM application was indicated.
Once the familiarization protocol was completed, participants then applied five one-handed, unilaterally directed sweeping strokes (distal to proximal) to the skin simulant with the IASTM instrument, emulating as closely as possible a typical patient treatment application for the simulated scenario. Participants lifted the instrument off the simulant between strokes to identify individual strokes more efficiently during data processing. The participant selected the direction (i.e., distal-to-proximal or proximal-to-distal) that felt most natural to them, and ultrasound gel could be added as emollient as needed during treatment.
The testing protocol was repeated three times, for 15 total strokes with the Técnica Gavilán® instrument (Figure 2) on two testing days. A total of 30 complete treatment strokes per participant were collected over the two treatment sessions. The second treatment session occurred between 24 and 48 hours after the initial testing session for all participants.
Statistical Analysis
Coefficient of variation (CV) and descriptive statistics were calculated in Excel 16.46 (Microsoft©, 2021). The mean force (Newtons N) was defined as the average of the vertical forces produced across the entire length of a single stroke and divided by the number of trials (Table 1). Coefficient of variation ([SD/Mean]*100) was calculated over two days for individual participants and the total strokes with the Técnica Gávilan® instrument (Table 1). Lower CV values corresponded to higher reliability; CV values ≤ 20% were preferred,17,18 but values ≤ 30% were also considered low enough to indicate data homogeneity.19 Box and whisker plots were created to compare average (mean) forces between two treatment session days (Figure 3).

Bland-Altman (BA) plots (Figure 4) were constructed for each participant to determine the agreement between the average (mean) forces applied over the two-day treatment sessions. The BA plots were created with data points from the Técnica Gávilanâ instrument. The BA plots were constructed with R 3.6.2 (The R Foundation for Statistical Computing Platform, 2019) and the BlandAltmanLeh (v0.3.1; Lehnert, 2015) software package. The BA plots were presented with mean differences, 95% limits of agreement (LOA), and the precision of those limits (e.g., 95% confidence intervals).
.jpeg)
RESULTS
The average forces produced across all 10 participants ranged from 1.6 to 9.0N (~160-900g). The highest average force was produced by Participant D (7.1-9.0N; 720-900g). The sample of participants demonstrated relatively small standard deviations (SD) in their mean force application for day one (≤ 1.2N; 120g) and day two (≤ 1.6N; 160g). The highest mean differences value for average force was also found with Participant D (1.9N; 190g), while the other participants had mean differences of 1N (100g) or less. Box and whisker plots also support similar force application among participants across Day 1 and Day 2 (Figure 3).
Only one CV value was above 20% (i.e., 23%) for any participant across either of the two treatment sessions, with the other 19 values ranging between 8 to 20% (Table 1). The CV values indicate acceptable consistency among the forces within an IASTM treatment session. The BA plot analysis suggested that all ten participants demonstrated agreement with average force production over Day 1 and Day 2 treatment sessions. Forces from all participants reflect that 98% of the data points were within the LOA. When assessing each participant, the LOA for average forces were narrowest for participant E (-0.6N, 0.3N; 60g, 30g) and widest for participant D (-3.7N, -0.2N;37g, 20g). The consistent findings within the box and whisker plots in a simulated model with a single stroke, combine with low CV values and acceptable BA plot results supports acceptable IASTM force application reliability.
DISCUSSION
The researchers investigated the ability of clinically experienced (i.e., licensed professionals) and non-clinically experienced (i.e., professional-level student) participants to reliably apply IASTM forces during a simulated treatment scenario. Participants who had at least completed the same IASTM training courses (i.e., the introductory IASTM Técnica Gavilánâ basic training course) were able to produce consistent treatment forces within and across the two treatment sessions. The box and whisker plots, CV values, and BA plots indicated the IASTM trained clinicians in this sample developed and maintained sufficient force consistency after completing an IASTM training course irrespective of their clinical experience levels.
The IASTM force ranges found in the study of 1.6N (160g) to 9N (900g) are similar to prior reported ranges of 2N (200g) to 9N (900g) to the posterior leg of human particicipants.13 The force ranges are also consistent with a descriptive study where researchers analyzed IASTM forces using similar methodology (i.e., analyzed IASTM stroke application on a skin simulant affixed to a force plate for mean and peak normal forces) and reported an average mean normal forces of 6N (600g) and peak normal forces of 8.9N (890g) across various instruments and professional clinicians.16 Evidence elucidating how IASTM force differences (e.g., force range, force peaks) influence physiological outcomes in human trials is not available. Animal models8,9,14 suggest a relationship between increased tissue healing and higher levels of force; however, the scenarios (e.g., enzyme induced injuries, smaller and more superficial tissue) and the IASTM forces (i.e., substantially lower) may not serve as good models for potential human trial results.
These pilot study results provide initial support that clinicians who complete similar IASTM training may produce similar force across IASTM treatment sessions. However, these results are limited to similarly trained IASTM clinicians. Thus, it would be beneficial to confirm IASTM force consistency in a larger sample of clinicians and to examine how different training influences IASTM force production ranges and consistency. Determining how IASTM force treatment ranges and IASTM training differences may or may not result in different physiological responses or patient outcomes at different IASTM dosages (e.g., amount of force, length force is applied) would help guide best-practice recommendations for IASTM application.
The pilot study results also expand on previous findings13,16 that provided insight into the amount of force that may be produced during an IASTM intervention to the medial gastrocnemius in otherwise healthy people by reporting the reliability of those forces and if clinician experience substantially influenced force reliability. The current data suggests that trained Técnica Gavilánâ IASTM clinicians produce consistent forces within 1N (100g) of force application without requiring extensive experience post-IASTM training. Although current research is indeterminate regarding an optimal force application for IASTM, the current findings and previous research13,16 indicate that IASTM trained clinicians may produce similar and consistent forces within and across IASTM treatment sessions. While clinicians have indicated that they may not try or know how to quantify forces during an IASTM treatment,15 the results provide some data to indicate that clinicians may still be able to apply a relatively consistent force during the treatment session.
There were a few limitations identified in the pilot study. One limiting factor was the relatively small sample size of ten participants with similar training background (i.e., Técnica Gavilánâ basic course), which may have influenced the forces participants applied during treatment sessions. Another limitation was using a single IASTM instrument and a single IASTM stroke; using different treatment strokes or IASTM instruments may influence force production and reliability. Additionally, the researchers methodology included the use of a simulated tissue on a force plate versus actual patients; while force measurement may be more accurate with the use of force plate technology, the amount of force used on the skin simulant may differ from human tissue that is pathological or healthy. Further, force application may vary by other clinical variables (e.g., table height, treatment goals, etc.) and the reported values may not be representative of all clinical scenarios or all clinicians. Future research should explore how different IASTM training, length of experience using IASTM, and clinicians’ perceptions of IASTM mechanisms or treatment effects influences IASTM force production and reliability. Finally, as a standardized IASTM optimal force recommendation does not exist in practice, future research should also explore the ranges described in the literature to determine how different amounts of IASTM force application and instrument technique affect treatment outcomes in clinical practice. This exploratory study provides insight and guidance for future studies on IASTM force application with patients.
CONCLUSION
The results of this pilot study provide insight into the amount of force and the consistency of forces during IASTM applied by trained clinicians with different levels of professional experience within a simulated treatment scenario. The participants demonstrated acceptable consistency within and across the two treatment sessions. Thus, clinicians who complete similar IASTM training may be able to quickly develop consistent force production during IASTM treatments and may be able to maintain that consistency across their careers.
Conflicts of interest
The authors report no conflicts of interest.