INTRODUCTION
Handball is one of the most popular Olympic team sports in Europe with an increased number of players over the past decades.1 It is now considered as one of the sports with the highest injury rates2,3 as it requires high-intensity skills including intermittent sprinting, jumping and landing, and one-on-one dual tasks with fast changes of direction.4 These are all considered to be high-risk demands associated with lower limb injuries since they require challenging technique and coordination elements like catching, throwing, passing, and dribbling.5 In handball aggressive contacts are also often used not only to stop the opponent but also to intimidate opposing strikers from approaching the goal. Unlike most other team sports, an unlimited number of fouls are allowed to neutralize opponents and disrupt the attacking team’s strategy.2,3,6 Injury incidence has been estimated at 89–129 injuries per 1,000 match hours for males and 84–145/1,000 match hours for females during elite competition.7 Knee and ankle joint injuries represent 50% of all injuries in handball1 including lateral ankle sprains (LAS) and anterior cruciate ligament (ACL) ruptures.8 Young female players (16-18 years old) are considered to be at higher risk for lower limb injuries compared to their male counterparts.1,9
For the sports health care staff and coaches of a competitive team, injury risk reduction remains a central issue, especially among young female athletes.10 The rehabilitation process and the decision to return to sport also require objective criteria to mitigate the risk of recurrence and allow athletes to return to the field at the same level of play.11,12 In order to effectively reduce the risk of injury, it is first important to identify risk factors that predispose athletes to injuries.10 Normative data or preseason baseline characteristics from healthy similar populations are therefore needed to first understand what is considered to be normal.13 A careful approach to the selection of relevant test protocols is needed for the health and performance staff around the handball player.14
The Star Excursion Balance Test (SEBT) is a reliable and accessible test to assess lower body dynamic postural control.15,16 It is a common clinical assessment tool to detect functional deficits15 associated with chronic ankle instability (CAI)17 and ACL deficient athletes.18 It has also demonstrated predictive value for identifying those at greater risk of lower limb injuries in team sports.19,20 A recent meta-analysis12 also highlights its relevance to assess lower limb injury risk factors among female team court sports. A modified version (mSEBT) using only three (anterior, posteromedial and posterolateral) of the eight original directions was proposed to simplify the execution of the test and avoid redundancy without decreasing accuracy and reliability of the test.15 This functional test is now considered as one of the most useful clinical tools to assess dynamic postural control among various injured populations.21
Recent evidence suggests that there are several factors that influence performance on the mSEBT, including the type of sport, level of expertise, age, and sex.13,15,22,23 Because of these factors, it is difficult to generalize performance values from one specific sport population to another. While the mSEBT is frequently performed and advocated in handball population,24 to our knowledge, no specific database of normative data for this sport exists. Values obtained from healthy athletes at baseline examinations are lacking. In order to assist clinicians when interpreting mSEBT scores from their teams, there is a need to create a large database of performance on this test among healthy players. This would help to target athletes who are at increased risk of injury. Indeed, if the player is below the ranges established for the healthy population, it could be considered that they have a deficit in dynamic postural control of the lower limb, which is now considered as an important risk factor for injury. The primary objective of this investigation was to establish normative ranges of mSEBT performance in young, healthy female handball players.
Handball is considered as an asymmetric sport due to frequent single-leg jumps, landing, side cuts and motor skills performed on the support limb.25 As mSEBT reach distance and asymmetry are considered potentially important risk factors for lower limb injury especially in team court female athletes,12,20,26 it is necessary to evaluate the normally-occurring level of asymmetry among young uninjured players. Consequently, a secondary aim of this study was to investigate whether there is a limb performance bias (dominant vs non-dominant) and establish normative values of the level of asymmetry in this population. Despite several studies from other sports16,23 that did not reveal limb dominance on the test, it was hypothesized that based on the asymmetrical nature of handball motor tasks, female players would exhibit higher values with their dominant limb. Finally, a handball team is composed of several player positions that exhibit various physical profiles and motor skills.27 Recent evidence has highlighted differences on injury incidence across player positions6,28 and it could be argued that specific trends exist regarding lower body dynamic postural control when comparing athlete position profiles.25 The last objective was then to establish estimates of healthy performance and the normally-occurring asymmetry across handball player positions.
MATERIALS AND METHODS
Design
This cross-sectional study was conducted using a large and homogenous sample of young elite female players recruited during a major women’s national tournament which is the highest-level tournament for this age group.
Participants
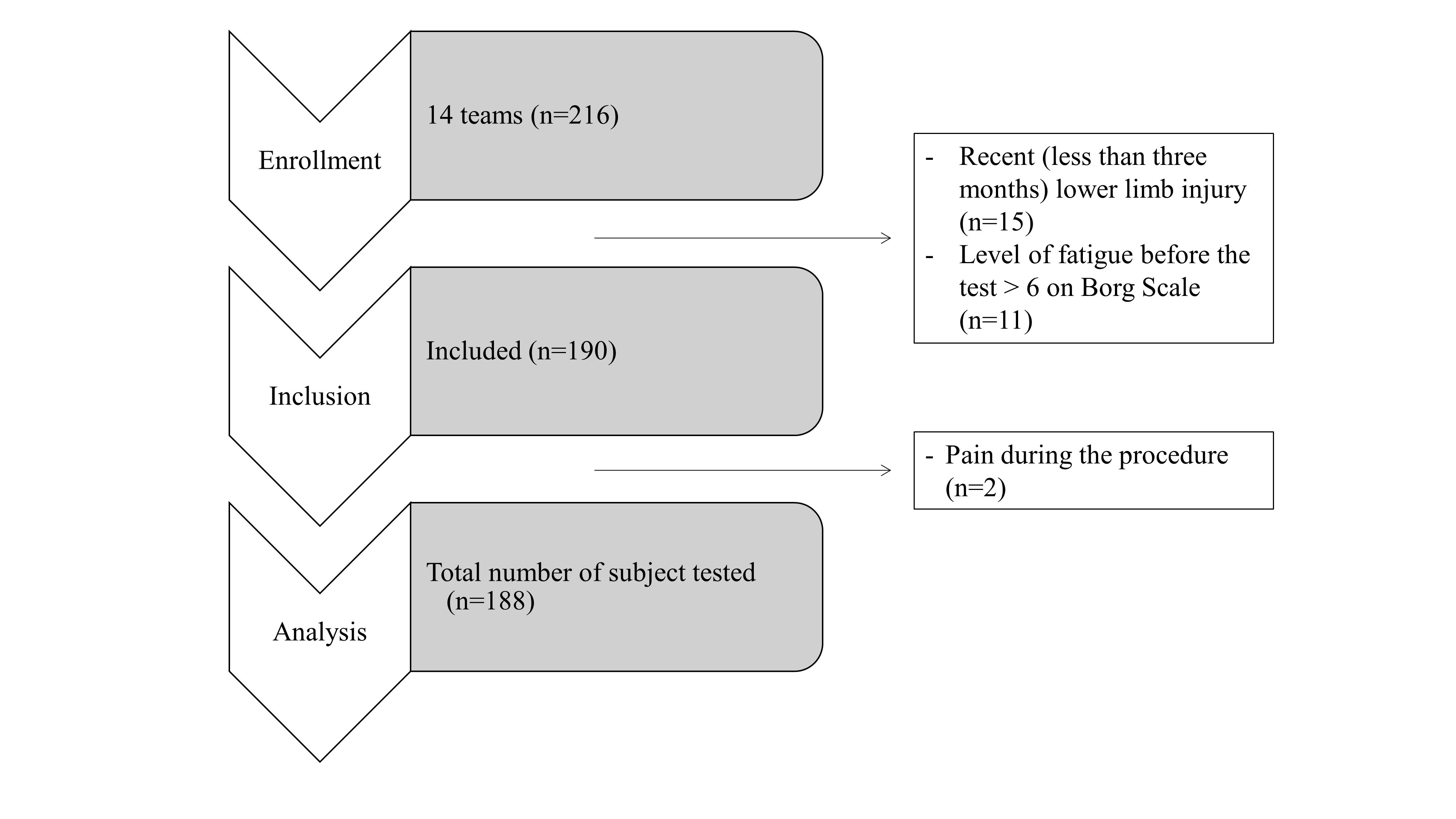
Two hundred and sixteen female handball players from fourteen elite female handball teams participated in this study (Figure 1). This study was approved by the Regional Ethics Committee of the University. Informed consent was obtained from all participants and the rights of athletes were protected. As all of them were under 18 years of age, parental or guardian received and signed the institutionally approved informed consent. Athletes were informed of the benefits and risks of the investigation.

As previous injury influences mSEBT performance,15 a clinical examination was performed by a certified sport physiotherapist and injury history was recorded before completing the testing session. Only healthy athletes were selected (e.g. pain free, cleared for full participation, not receiving medical treatment) to create a reliable database of mSEBT performances for handball female players. Players with recent injuries on lower limbs (i.e. less than three months) were not included in the study.
Prior to the test, age, level of play (club division and experience at that level), position on the field and limb dominance were recorded. Athletes were asked to determine their level of fatigue using a Borg scale ranging from 0 to 10.29,30 Then, after the completion of the test, athletes had to report any perception of pain during the test. Athletes who presented a level of fatigue greater than 6 (i.e. strong fatigue) or/and perception of pain were excluded from the analysis. Athletes were also split into four position groups (wing, back, goalkeeper and pivot) according to their usual match and training positions. The dominant limb was defined as the preferred push-off leg during handball tasks such as jumping and shooting.31
There was a homogenous level of competition and practice (8h of training plus one match per week) across athletes as they were considered as the best national handball players under 18 years of age (Elite National 1).
Procedures
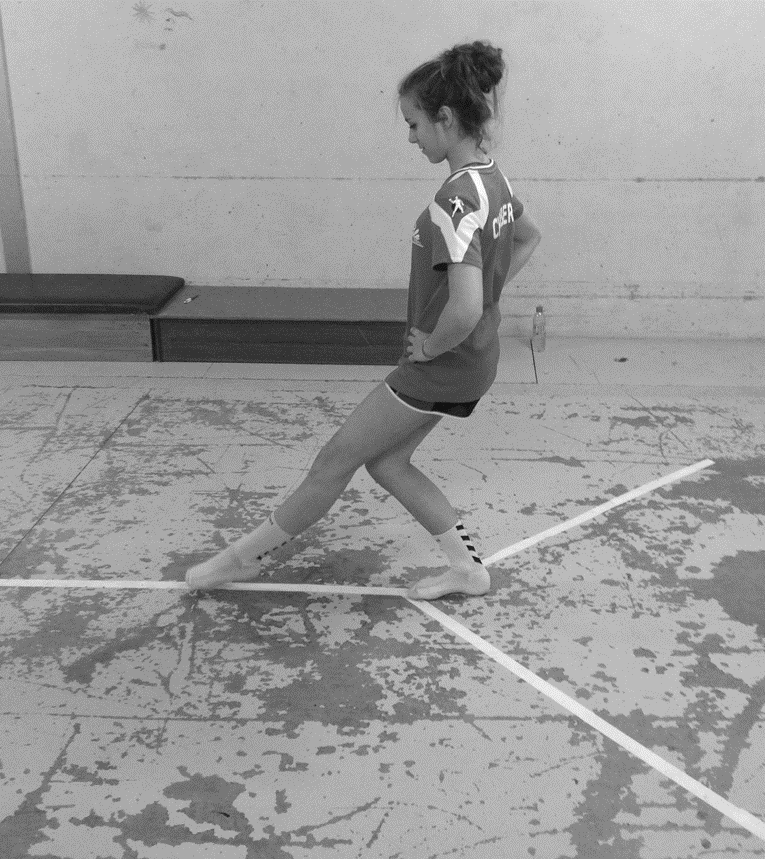
The mSEBT procedure followed recently published guidelines16 and methods described in large cohort studies in order to assess dynamic postural control among athletes.13,15,32 Dynamic postural control refers to the taskt that the subject while standing on a single limb, has to reach as far as possible with the opposite limb along several lines on the floor and return to the initial position without losing balance.15 It therefore reveals the athlete’s postural ability during a dynamic movement of the opposite lower limb. Athletes performed a standardized mSEBT training session prior to the testing session which consists of four practice trials on both legs in each direction.33 No technical skill is needed for implementing the mSEBT, as anyone can administer the test with appropriate training regardless of their qualification. Indeed, Van lieshout et al. showed that if the evaluator is trained properly, test reliability remains good to excellent.34 The instructions for performing the mSEBT were given by the same trained investigator who demonstrated and the test and feedback was provided during the practice trials in accordance to the established guidelines. Athletes performed the mSEBT on each lower limb, starting with the right limb and alternating side for each direction in order to avoid fatigue. They stood barefoot in double limb stance (i.e. feet together) in the middle of the testing grid. In order to ensure an equal position across the measured trials, athletes placed with the most distal aspect of their great toe at the origin line (Figure 2). This foot position remained constant between all testing directions, in accordance with previously published standards.13,15,26

Athletes were asked to reach the maximal distance along each direction with the most distal portion of the reaching foot touching the directional line and regaining double limb stance. For each trial, athletes were required to maximally reach in the respective test direction, slightly touch the tape measure with the toe of the reaching limb without shifting weight to it. During the test, athletes were asked to keep their hands on the hips and were not allowed to move or lift the stance foot.35 Three trials were then recorded for each leg in the three directions.15 In order to avoid fatigue, the measured limb was alternated between each direction. Performance was assessed by the same investigator with a measuring tape directly placed on the floor.
For between-athlete comparisons, reach distances were normalized to lower limb length.15 The leg length was measured in supine position, from the anterior superior iliac spine to the medial malleolus by the same investigator.
The average of the three trials was used for analysis of each outcome measure.13 Normalized reach distances (i.e. percentage of limb length) for the anterior (ANT), posteromedial (PM) and posterolateral (PL) directions were calculated from the following equation.15,34
Normalized “Given” score (%)=mean of the three trials in “Given” direction (cm)Limb length (cm)×100
Mean of those directions were used to calculate the composite score (COMP) for each athlete from the following equation:
Composite score(%)=ANT(%)+PL(%)+PM (%)3
Statistical Analyses
Assessment of Limb Performance Asymmetry: To assess the level of side-to-side asymmetry, pairwise t-tests were used to compare the dominant and non-dominant limb for each direction as well as the composite score. Limits of agreement were calculated using Bland Altman methods36,37 for each direction and COMP score in the overall sample. The asymmetry values were then contextualized based on the established minimum detectable differences (MDD) for each direction in the published literature.16 Indeed, even if the differences may appear significant, it is necessary to verify that they can be identified with the test by exceeding the MDD.
Overall mSEBT Performance: After checking that no side-to-side asymmetry existed, both limbs were pooled to create overall estimates of mSEBT performance for each participant. Means, standard deviation (SD) and 95% Confidence Intervals (95% CI) were used to provide a point estimate and measure of variability of what is considered to be “normal” for female handball players.
The Influence of Position on mSEBT Performance: Finally, means and 95% CI were calculated for player position. Forest plots were then generated to visually appreciate any trends associated with player position and mSEBT performance. As well, asymmetry scores were further stratified to player position and the asymmetry upper and lower limits were compared to the established MDD.
All statistical analysis were performed on JASP (Amsterdam 0.16.2.0). Before carrying out the statistical tests, normality was checked using the Shapiro–Wilk test. For all analyses, statistical level of significance was fixed at p < 0.05 and effect size (i.e. Cohen’s d) were calculated if necessary for all the comparison.
RESULTS
After exclusion criteria were applied, 188 (16.8 ±0.9 years) of the 216 original athletes were included in this study (Figure 1). Baseline characteristics for the participants are reported in Table 1.
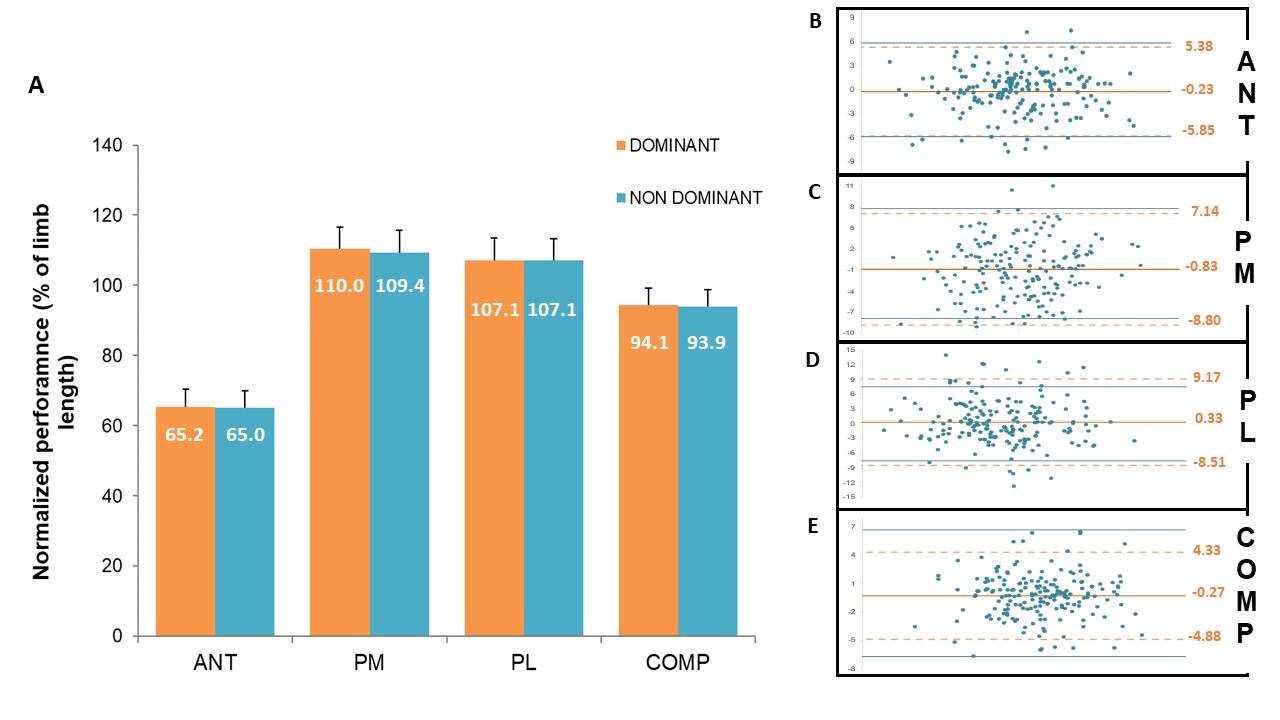
Normalized performance for the overall sample and estimates for the population (95%CI) can be found for each direction and the COMP score in Table 2. The ANT direction had the lowest normalized reach distances across participants. Performance in both posterior directions was similar and confidence intervals did not overlap with ANT values.
When analyzing side-to-side asymmetry, no significant differences were found regarding limb dominance for any direction (p>0.05). Performance of the overall sample for dominant and nondominant limb as well as means of differences and limits of agreements for each direction are presented in Figure 3. Across all mSEBT directions, there was less than 1% asymmetry between limbs, which indicated that there was not a limb bias in mSEBT performance. The difference between the dominant and non-dominant limb (with 95%CI) averaged -0.23% [-5.95; 5.38] for the ANT, -0.85% [-8.80; -7.14] for PM, 0.37% [-8.51; 9.17] for PL and -0.27% [-4.88; 4.33] for the COMP score (Figure 3B, C, D, E). When comparing to the established MDD values for each direction,16 the majority of the asymmetries would not be considered meaningful (Figure 3).
__posteromedial_(.jpg)
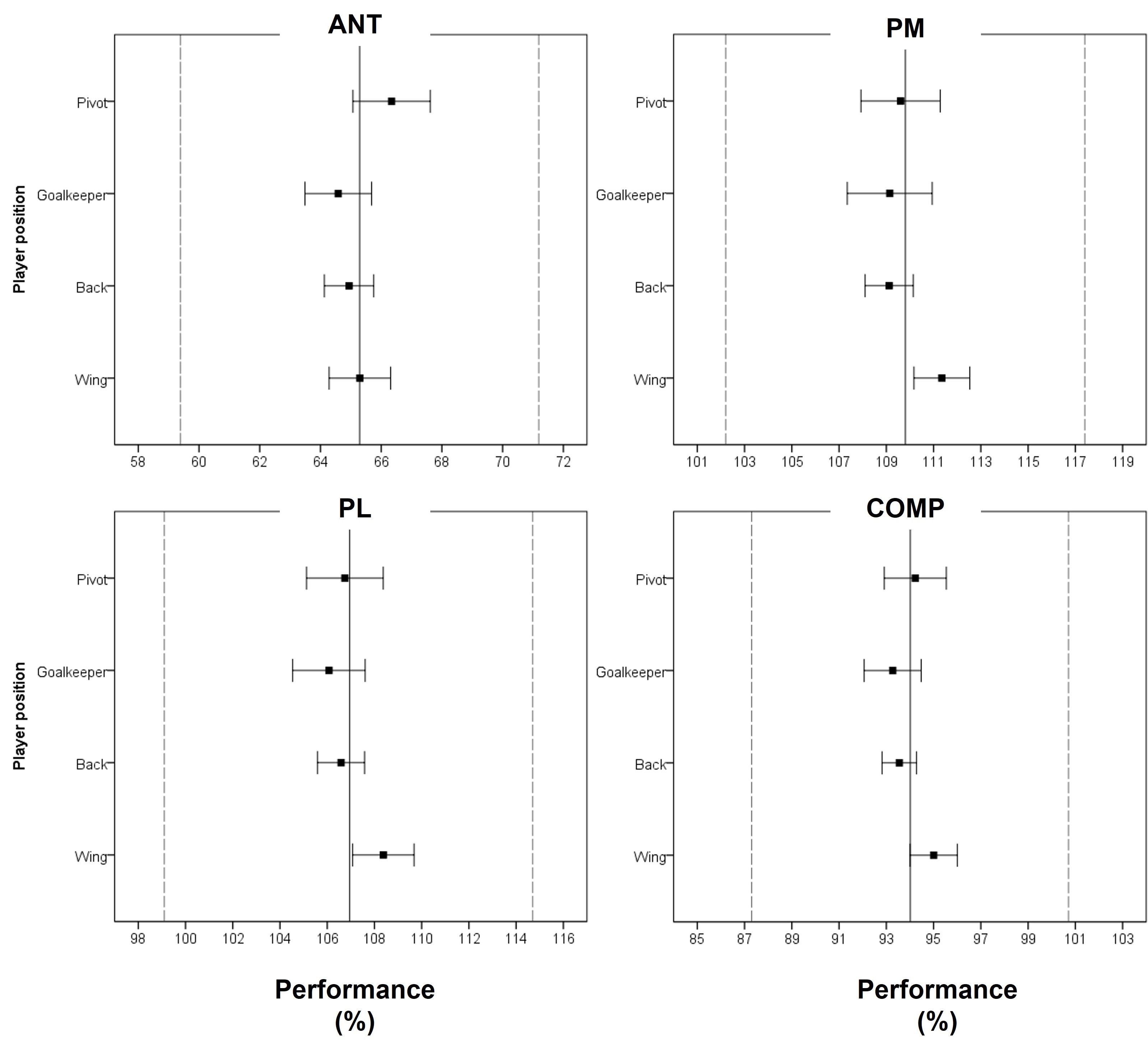
Figure 4 illustrates means and 95% CI performance per direction for the overall population and each of the four player positions.
_and_95__confident_intervals_of_normalized_performances_in_anteri.jpg)
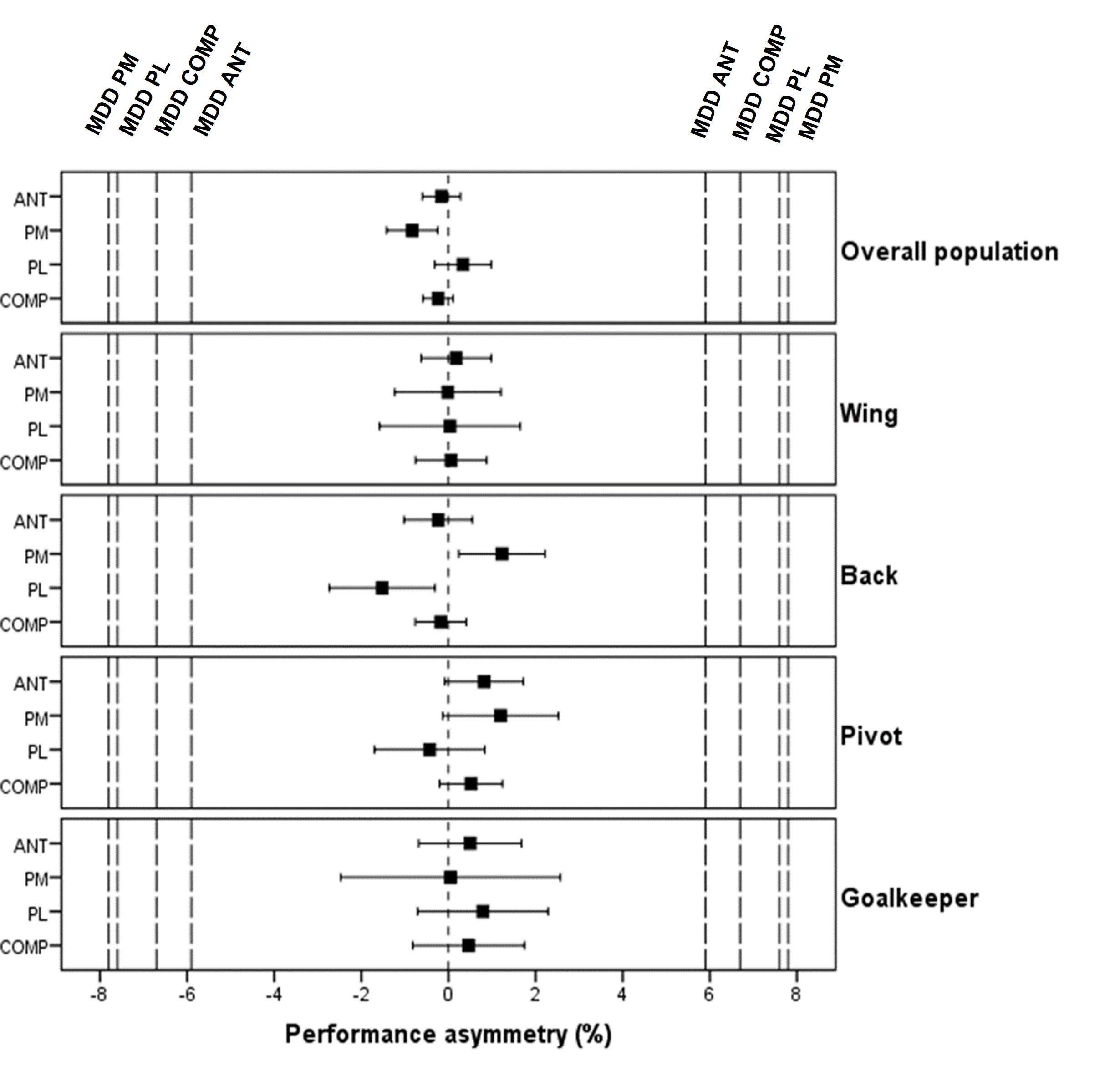
Mean and 95% CI asymmetry of performance for the overall population and across player positions are represented in Figure 5. for each direction.
_and_95__confident_intervals_of_performance_asymmetry_for_each_pl.jpg)
DISCUSSION
The primary purpose of this study was to provide normative values for performance on the mSEBT in young elite female handball athletes. This is the first large sample cross-sectional study investigating mSEBT performance among this at-risk population. Considering the narrow range of 95%CI, clinicians can assume that healthy players from their team should have comparable mSEBT performance (65% for ANT, 110% for PM, 107% for PL direction and 94% for the COMP score) when performing the same testing procedure. Based on the overall trends uncovered, both the PM and PL directions exceed 100% of limb length. When comparing to National Collegiate Athletic Association (NCAA) Division I female players,13 this population exhibited higher COMP scores than athletes from all sports that have been previously evaluated (basketball, golf, hockey, soccer, softball and volleyball). Interestingly, the 95% CI reported from this study did not overlap with those calculated from this sample. Those differences seem to be highly influenced by much greater scores in the PL direction compared to others sports.13 Comparable performances were observed, especially in basketball, for ANT (64.3% and 63.4%), and in hockey for PM (110.3 and 113.1%) on the dominant and non-dominant limbs respectively. Results from handball female players are also very similar in PM and PL direction but considerably lower ANT scores than those previously reported (71 to 81%) among high school basketball and older soccer female players.23,26 When comparing results from this study with elite and semi-professional female volleyball players,32 ANT scores were also lower (73.5% and 68.6% respectively) while all others performance values were much higher (90.4 and 83.7% for PM, 89.3 and 83.6% for PM, 84.5 and 78% for the COMP score) despite similar testing procedures. These results confirm that mSEBT performance appears to be influenced by the type of sport. Those discrepancies may be related mainly to anthropometric differences, physical demands, and movement patterns specific to handball. This sport is indeed characterized by intense body contact and demanding coordination skills, like catching, throwing and dribbling while being pushed by an opponent. Maximum intermittent sprints followed by explosive sidestep cutting maneuvers are also very frequent.
The second objective of this study was to evaluate side-to-side asymmetry according to lower limb dominance on mSEBT. Limb dominance does not appear to be a factor related to mSEBT performance in this group of athletes. This result aligns with evidence from other sports16,23 where side-to-side asymmetries on the test were not revealed. Handball female players from this study performed very similarly on their dominant and non-dominant limbs. Indeed, the upper and lower limits of the 95% CI for the level of asymmetry were very similar to the reported MDD (i.e. 5.7 vs 5.87%, 8.79 vs 7.84%, 8.8 vs 7.55% and 4.6 vs 6.7% for ANT, PM, PL direction and COMP score respectively).16 More precisely, none of the 188 athletes exceed the MDD for limb asymmetry in the COMP score, while only 6.9% (13 athletes) overlap it in the ANT and PM direction and 10.6% (20 athletes) in PL direction (Figure 3). These results validate the external validity of the limits found in this sample. Thus, although handball is a sport that is considered highly asymmetrical in nature,25 there does not appear to be a pattern of differences in performance between the two lower limbs. A major side-to-side asymmetry should therefore be carefully addressed as it may reveal a potential risk factor (see below) for future lower limb injuries.20,26 It should be noted that in most studies, the dominant limb is defined as the one used to kick a ball while in handball it systematically refers to the preferred push-off leg.5
The third objective of this study was to determine more specific mSEBT performance and amount of asymmetry according to the player position. This is the first study investigating dynamic postural control across playing position in handball. Team handball is composed of seven players on the court exhibiting various physical profiles.27 For example, wingers are the fastest (15 and 30 m sprint), strongest (counter-movement jump), and most enduring players on handball teams compared to other player positions.27 In addition, female wingers show different physical and anthropometric characteristics than other positions as they are typically lighter and shorter.38 The differences in performance observed in this study could also be explained by positional demands - wing players require more intensive locomotive activity patterns and motor skills such as sprinting, jumping and complex landing with unbalanced distribution than other playing positions.39 Conversely, goalkeeper activity skills could be considered more static than other players. However, differences across player positions did not exceed the MDD with all 95% CI overlapping. Those results indicate trivial differences between player positions so that practitioners can be confident when comparing athletes from several positions on the field. When focusing on pattern of asymmetry, the narrow range of 95% CI obtained after splitting athletes (Figure 5) confirms the homogeneity of the results.
There is consistent evidence that the mSEBT is a relevant test in the context of injury risk.12 Indeed, this test is widely used by sport clinicians to target individuals with higher risk of injury.20,21,26,40–42 Similarly, numerous studies supported the use of this test in the return to sport decision following lower limb injuries such as ACL reconstruction43 and lateral ankle sprains.44,45 While injuries were not prospectively monitored in the athletes included in this study, several results appear to be relevant for clinicians. As previously mentioned, the obtained COMP score in the overall population (94.1%) and each player positions were higher than most reported studies from various sports. Very interestingly, this value was previously described as an important cut-off score, as female basketball players exhibiting a COMP normalized reach distance lower than 94.0% were 6.5 times more likely to sustain a lower extremity injury.26 It appears therefore important for medical and technical staff to consider this value as a minimum target for female handball players in the context of injury prevention and the process of return to sport. Similarly, side-to-side asymmetry is a key factor for injury risk,15,20,26 normative values were therefore calculated in this populations. Results show that 95%CI of normalized asymmetry never exceed 3% regardless the direction and player position. Stiffler et al.20 showed higher risk of lower limb injuries when normalized asymmetry was > 4.5% in the ANT direction, with athletes in the injured group demonstrating 1.9% limb length greater anterior asymmetry on average than those in the healthy group. When applying the cut-off score of 4.5% normalized asymmetry in the ANT direction it represents 22 athletes (11.7%) in our population. Similarly, basketball players exhibiting absolute asymmetric performance greater than 4 cm in the ANT direction were 2.5 times more likely to sustain lower limb injuries.26 In handball, wing players were more likely to sustain injuries than other positions.28 Handball coaches and clinicians should be alerted when their players fall outside the reported 95%CI of mSEBT scores and limb asymmetry (Figure 4 et 5). However, prospective studies are needed to confirm and clarify current results and estimates for the population and determine specific asymmetry cut-off scores for team handball players.
Limitations of this study include the players’ background regarding sports activities before handball.25 It can be argued that practice history before handball could allocate skills that influence performance on mSEBT. Furthermore, the tournament lasted three days and some teams were evaluated at the beginning and others at the end of the competition. Moreover, performance is also influenced by age and sex.13,23 Since participants were all recruited from young elite women’s handball teams, the results may not be generalizable to other age groups, participation levels or sport disciplines. Further studies are therefore needed for male handball athletes and across different age groups and ability levels.
CONCLUSION
In this study, a large normative database of mSEBT performance among young, elite, healthy handball players was established. Female handball players are considered a high-risk population for lower limb injuries. Clinicians can use these results as a comparison for preseason baseline testing, to evaluate the rehabilitation process when baseline characteristics are missing or as return to sport criteria. Limb dominance did not influence performance so side-to-side asymmetry that exceeds established MDDs should alert clinicians and coaches as a potential risk of future injuries. These findings should be used with caution when comparing athletes from different sport populations. Further prospective studies are needed to establish accurate cut-off scores for injury risk.
ETHICS APPROVAL
This study was approved by the Regional Ethics Committee from Savoie-Mont Blanc University.
CONFLICTS OF INTEREST
The authors have no conflicts of interest
ACKNOWLEDGMENTS
The authors would like to thank Aurélie Collomb-Clerc for her precious help during the experimentation, the technical and medical staff of each team for their time and confidence, and all the volunteers who worked for the organization of the competition. The authors also thank all the athletes who volunteered to participate in this study as well as the French Handball Federation.