
INTRODUCTION
In sports across the globe, some of the most investigated injuries are those related to the head. Most people associate concussions and head-related injuries with American football. However, a study using the National Collegiate Athletic Association Injury Surveillance System found that 8.6% of injuries to women’s soccer athletes were concussions as well as 5.8% of injuries in men’s soccer athletes.1 In fact, this number is potentially much larger considering more than 50% of concussions go unreported.2–6 Therefore, the number of concussions reported during soccer activity is likely a conservative measure of incidence.
In addition to concern over concussion in sport, repetitive head impacts without immediate clinical manifestation may cause long term consequences including negative brain health.7–13 On average, players head the ball six to 12 times in a competitive soccer match where the ball could travel over 22 m/s in amateur games.14 Since soccer is the world’s most popular sport and includes more than 265 million players worldwide, soccer heading is a common cause for repetitive head impacts.15 However, the relationship between subconcussive heading and brain injury remains poorly understood.16–18 There have been multiple studies where researchers have found cognitive dysfunction or negative brain alterations after purposeful heading.2–6,10,13 However, another study has shown that there is no detrimental relationship between the number of purposeful headers and neurocognitive measures.18 Therefore, it remains unknown how repetitive head impacts may affect long term brain health.
Since head impact magnitude has been linked to injury predisposition,19 it is important to understand how to mitigate the energy received when the head is impacted during soccer participation. Purposeful heading includes repetitive low-level impacts and the magnitude transferred to the head can depend on many factors. Of these factors, neck strength is one that has received considerable recent attention in the literature. A correlation has been shown between neck strength and head impact kinematics where individuals with higher neck strength measurements had lower head accelerations upon impact.20–22 Weaker mean overall neck strength was significantly associated with concussion and that for every pound of neck strength that athletes gain, their chances of a concussion decreases by five percent.20 Therefore, the current study investigated a way to minimize head accelerations by testing one possible intervention. The purpose of the study was to determine if a six-week cervical strengthening program affected strength, neurocognition, and purposeful soccer heading biomechanics. The following research questions underpinned the purpose: (1) Would a six-week neck strengthening program improve neck strength in soccer players?, (2) What effect would a six-week neck strengthening program have on head impact biomechanics during purposeful soccer ball heading?, and (3) What effect would a six-week neck strengthening program have on neurocognitive outcomes after a bout of purposeful soccer ball heading? The hypothesis was that the strengthening program would increase neck strength which would in turn decrease the impact magnitude the head experiences upon purposeful heading and maintain or improve (learning effect) players’ neurocognition after purposeful heading.
METHODS
Participants
A total of 20 varsity collegiate soccer players participated in this study (12 female, 8 males, age = 20.15±1.35 years, height = 171.67±9.01 cm, mass = 70.56±11.03 kg). Each participant was over the age of 18 and signed a consent form approved by the host institution’s human subjects review board. The participants also played a variety of positions such as forward (N=4), midfield (N=8), defender (N=5) and goalie (N=3). A breakdown of demographics between the two groups can be found in Table 1.
Procedures
Prior to beginning data collection, the Institutional Review Board at the University of Lynchburg approved the study. All men’s and women’s soccer athletes at one institution sponsoring National Collegiate Athletic Association Division III athletics were sent an email that provided information on the study and were asked to respond if they were interested in participating. To begin the study, participants signed the informed consent form to be made aware of all the risks and benefits of the study. Next, the participants’ height, mass, neck girth, and neck segment length were measured. Participants’ height was measured in centimeters (cm) with a stadiometer (Seca Model 222, Hamburg Germany) and mass was measured in kilograms (kg) using a scale (Tanita BWB-800 Tokyo, Japan). While the participants were sitting straight and looking at an object at eye level, the head-neck segment length and neck girth was measured in cm with a metric tape measure. The participants’ head-neck segment lengths were measured in a straight line using a tape measure from the seventh cervical vertebrae to the most superior region of the head observed in the frontal plane.23 The participants’ neck girth was measured just above the thyroid cartilage.24
After anthropometrics were recorded, half of the male and half of the female athletes were randomly selected for the experimental group while the other half served as the control group. A random number generator was used to determine group membership, and the researcher who collected all data was blinded to group membership. Before completing the baseline tests, the athletes participated in a neck warm up to reduce the possibility of injury. The neck warm up consisted of neck rotations (15 seconds (s) clockwise and 15 s counterclockwise) and neck stretching (two repetitions each of 15 s for flexion and extension).23 Each athlete completed a series of neck strength tests, purposeful heading biomechanics tests, and a battery of cognitive tests to serve as baselines for a comparison later in the study. The experimental group followed a neck strengthening program for six weeks as part of the normal strength and conditioning program, and the control group did not perform neck strengthening exercises. However, both groups participated in the same soccer specific strength and conditioning program as prescribed by the team Certified Strength and Conditioning Specialist. After the six weeks of neck strength training, the participants completed the same series of neck strength tests, purposeful heading biomechanics tests, and battery of cognitive tests to compare to the baseline testing results.
Neck strength testing
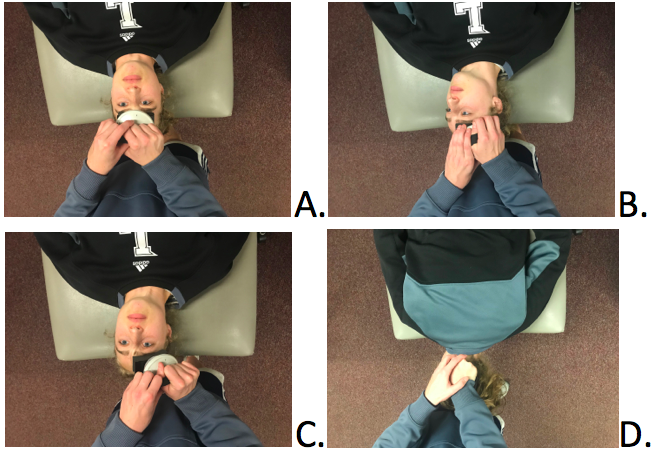
One research team member measured neck strength as described by Kendall et al.25 with an isometric dynamometer (MicroFET®2 Digital Handheld Dynamometer, Hogan Scientific, Salt Lake City, UT). Using an isometric dynamometer has been found to be a reliable and valid measure of cervical muscle strength in a seated position.26 However, strength was measured in a supine or prone position as described by Kendall et al.25 Strength measurements of the anterior neck flexors (Figure 1A; in supine the participants attempted to lift the head straight up), bilateral anterolateral neck flexors (Figure 1B; in supine the participants attempted to lift the head with the head turned completely in one direction/the other direction), bilateral cervical rotators (Figure 1C; in supine the participants turned the head to the left/right), and bilateral posterolateral neck extensors (Figure 1D; in prone participants raised their heads with their head completely turned to left/right) were recorded. In order to familiarize the participants with the testing method, they completed two practice trials followed by three recorded trials for each direction of motion. Participants rested for 30 seconds between each trial and each trial lasted for three seconds. The mean for each position was calculated based on the three trials and used for analysis.
__bilateral_anterol.png)
Purposeful heading biomechanics testing
A JUGS soccer machine (JUGS Inc., Tualatin, OR) was used to simulate a kick that soccer players would be most likely to head in a game or practice. The speed of the ball coming out of the machine was adjusted to two different speeds to simulate low and high velocities of balls that players head during games or practices. A size five soccer ball pumped to 5,624.55 kgf/m² was dispensed out of the JUGS machine 35 m away from participants at 11.18 and 17.88 m/s as described in a previous study.1 Each participant received five balls at each speed with a one-minute rest between balls. The participants were assigned a numbered inertial measurement unit (xPatch sensor, X2 Biosystems, Seattle, WA) that they wore while heading the 10 soccer balls. The sensor was applied over the right mastoid process with an adhesive patch. The xPatch sensor was used to measure the magnitude of the impact of the ball on the head in peak linear acceleration (PLA; g) and peak rotational acceleration (PRA; deg/s2), common metrics used to characterize head impact biomechanics as they are thought to be related to injury risk.19 The xPatch sensor also provided impact duration (time the ball and head made contact), and Gadd Severity Index (GSI). Higher durations would result in greater force transmission which may have clinical implications leading to the inclusion of duration as a dependent variable. The GSI scores provided information regarding the likelihood of an impact causing catastrophic head injury.27 Although the xPatch has been shown to overestimate head impact magnitude,28 it serves to facilitate frequency and magnitude comparisons between groups when all of the participants wear the sensors29 which was the case in the current study. Head mounted sensors like the xPatch have been found to provide an accurate detection of the peak angular acceleration when compared to other helmet mounted systems.29 Once the purposeful heading biomechanics test was completed, the sensor was removed, placed back on the charging dock, and the data were downloaded using a laptop computer (Apple Inc, Macbook Air, Cupertino, California).
Cognitive testing
After participants finished the purposeful heading biomechanics test, they completed the CNS Vital Signs (CNSVS) computer based cognitive test. The test was used to establish the participants’ neurocognitive performance and symptom load. The CNSVS provided data regarding the participant’s verbal memory, visual memory, executive function, reaction time, and symptom severity scores. Higher values indicate better performance for verbal memory, visual memory, and executive function. Lower reaction time scores indicate superior performance and higher symptom severity scores indicate more symptoms. Age adjusted standard scores for verbal memory, visual memory, and executive function were used while reaction time was measured in milliseconds. Symptom severity scores (range=0-144) summed the individual symptom scores on a 0-6 scale (0=none at all, 1-2=mild, 3-4=moderate, 5-6 severe). Scores were reported in the CNSVS detailed test result reports. CNSVS has been found to have reasonable test-retest reliability previously in broad populations.30,31
Neck strengthening protocol
After the baseline testing was complete, the participants in the experimental group participated in a six-week neck strengthening program (three times per week) created by a Certified Strength and Conditioning Specialist. The Shingo Imara™ (Shingo Imara, Ann Arbor, Michigan) was used to provide resistance during neck strengthening exercises. The participants completed the number of repetitions and sets represented in Table 2 for each of four exercises, resisted cervical flexion, extension, and lateral flexion on both sides from a seated position (Figure 2).

A Certified Strength and Conditioning Specialist monitored all exercise prescription, progression, and strength training sessions. The exercises were chosen because they were thought to target the neck muscles most utilized for purposeful heading.
Statistical analysis
The data were collected and organized in an Excel (2013 version, Microsoft Inc., Redmond, WA) spreadsheet for further analysis. In this study there were two independent variables, group (experimental and control, between factor) and time (pre and post, within factor). The dependent variables were neck strengthening measurements for each direction; PLA, PRA, duration, and GSI for heading biomechanics at each of the two speeds; and verbal memory, visual memory, executive function, reaction time, and symptom severity scores from the cognitive testing. Therefore, a 2x2 mixed model ANOVA was used to analyze the data from each dependent variable separately in SPSS (Version 26, IBM, Inc, Armonk, NY). Partial eta squared (ηp2) was calculated as an effect size for the interactions and Cohen’s d as an effect size for post hoc tests. Results were interpreted with ηp2=0.01 indicating a small effect, ηp2=0.06 indicating a medium effect and ηp2=0.14 indicating a large effect32 while Cohen’s d was interpreted as d=0.2 as small, d=0.5 as medium, and d=0.8 as large.33 The alpha value was set to p<0.05 a priori and Bonferroni post hoc tests were used to determine where significant pairwise differences existed for significant interactions.
RESULTS
Neck Strength
Means and standard deviations for strength testing dependent variables can be found in Table 3. The interaction between time and group was significant for anterior (F1,17=41.78, p=0.04, ηp2=0.22), right anterolateral (F1,17=4.80, p=0.04, ηp2=0.22), and left anterolateral (F1,17=6.48, p=0.02, ηp2=0.28) strength measurements. Post hoc tests showed strength improved pre- to post-intervention measures in the anterior direction for both the strengthening (p<0.001) and the control (p=0.02) groups, but only for the strengthening group for right anterolateral (p<0.001) and left anterolateral (p<0.001) directions. The interaction between time and group was not significant for right rotation (F1,17=2.12, p=0.16, ηp2=0.11, 1-β=0.28), left rotation (F1,17=3.20, p=0.09, ηp2=0.16, 1-β=0.39), right posterolateral (F1,17=2.98, p=0.10, ηp2=0.15, 1-β=0.37), or left posterolateral (F1,17=2.86, p=0.10, ηp2=0.14, 1-β=0.36) strength measurements.
Purposeful heading biomechanics
Means and standard deviations for heading biomechanics dependent variables can be found in Table 4. There was no interaction present between group and time for PLA at 11.18 m/s (F1,11=0.66, p=0.43, ηp2=0.06, 1-β=0.12) or PLA at 17.88 m/s (F1,11=0.98, p=0.34, ηp2=0.08, 1-β=0.15). There was also no interaction present between group and time for PRA at 11.18 m/s (F1,11=0.003, p=0.96, ηp2<0.01, 1-β=0.05) or for PRA at 17.88 m/s (F1,11=0.002, p=0.97, ηp2<0.001, 1-β=0.05). There was no interaction present between group and time for head impact duration at 11.18 m/s (F1,11=0.41, p=0.53, ηp2=0.04, 1-β=0.09) or at 17.88 m/s (F1,11=0.08, p=0.79, ηp2=0.01, 1-β=0.06). Finally, there was no interaction present between group and time for GSI at 11.18 m/s (F1,11=1.03, p=0.33, ηp2=0.09, 1-β=0.15) or at 17.88 m/s (F1,10= 0.55, p=0.48, ηp2=0.05, 1-β=0.10).
Cognitive test
Mean values and standard deviations for cognitive dependent variables can be found in Table 5. When determining the effects on neurocognition and symptoms, the interaction between time and group was significant for visual memory (F1,17=5.16, p=0.04, ηp2=0.23). Interestingly, post hoc results revealed visual memory decreased for the control group from pretest (46.90±4.46) compared to posttest (43.00±4.03; mean difference=3.90, 95% CI=0.77-7.03, p=0.02, Cohen’s d=0.92). The interaction between time and group was not significant for verbal memory (F1,17=0.01, p=0.91, ηp2<0.001, 1-β=0.05), executive function (F1,17=0.71, p=0.41, ηp2=0.04, 1-β=0.13), reaction time (F1,17=1.05, p=0.32, ηp2=0.06, 1-β=0.16), or symptom severity score (F1,17=2.40, p=0.14, ηp2=0.12, 1-β=0.31).
DISCUSSION
The purpose of the study was to determine if a six-week cervical strengthening program affected strength, neurocognition, and purposeful soccer heading biomechanics. The neck strengthening program only significantly improved strength for the muscles in the anterior and anterolateral (right and left) directions. In the second part of the study, there were no significant findings for the heading biomechanics portion of the experiment. Finally, the single significant finding for the neurocognitive component was a decrease in visual memory from pretest to posttest only in the control group.
Neck Strength
The neck strengthening protocol significantly increased anterior and anterolateral neck strength. Rotational strength and posterolateral strength failed to improve despite strong effect sizes that indicate clinically meaningful strength improvement. The exercises selected may be the reason for the finding. Rotation, anterolateral, and posterolateral movements were not specifically targeted because the movements were not considered as important during purposeful heading. However, the protocol exactly as described by Kendall et al25 was used. Despite the lack of significant improvement in rotational and posterolateral strength, the Shingo Imara™ device was successful in improving neck strength with targeted exercise prescription and supervision by a Certified Strength and Conditioning Specialist. Improving neck strength may be important in athletic performance enhancement, even if the positive effect on head injury prevention remains not fully understood. Details regarding the findings related to the three purposes are provided in the sections below.
Purposeful heading biomechanics
Similar to the current findings, Mihalik et al.34 also found that increasing neck strength failed to lead to lower linear and rotational accelerations of the head during impact. We also reported small to medium effect sizes suggesting limited clinical meaningfulness. It remains unknown why the increases in cervical strength observed failed to alter head impact biomechanics. Although neck musculature activity while performing the purposeful heading trials was not measured, the head impacts were anticipated by the participants as they knew the ball was coming toward them in both groups (experimental and control). Perhaps deep neck stability exercises would provide different results.
Others have shown that there is a correlation between neck strength and head impact kinematics where individuals with higher neck strength measurements had lower head accelerations upon impact.20–22 Weaker mean overall neck strength has been significantly associated with concussion and for every pound of neck strength that athletes gain, their chances of a concussion decreases by five percent.20 Lamond et al.35 found that anticipated headers, such as the ones in the current study, had lower linear and rotational head accelerations than unanticipated deflections or hits. Despite whether they were anticipated or not, head impacts to the front of the head, the maneuver used in the current study, have been found to create linear and rotational accelerations that were well below those associated with traumatic brain injury.35 The magnitudes in the current study align similarly with the literature for similar impact types.35
Cognitive Test
Kaminski et al.17 used a test similar to CNSVS called Automated Neuropsychological Assessment Metrics (ANAM) to evaluate youth soccer players’ neurocognition after purposeful soccer heading over a season and found that there was little to no relationship between heading and measures of neurocognitive performance. In another study by Kaminski et al.,18 collegiate and varsity high school women’s soccer athletes had their cognitive function and balance evaluated before and after the course of a season while heading frequency was recorded. The study used the two-part Wechsler Digit Span test to determine cognitive function which included two of the same neurocognitive sections as the testing used in the current study, visual memory and verbal memory.18 Their results showed that there were no statistically significant changes in cognitive function or in balance. The researchers in these two studies did not determine if neck strength played a role in neurocognitive performance, but findings did show that repetitive heading showed no change in neurocognitive performance. However, one study found cognitive and vestibular impairment immediately following a bout of 20 purposeful headers within three minutes.36 The current findings suggest maintenance of visual memory (statistically significant differences and large effect size) for the neck strengthening group but no effect of group on verbal memory, executive function, or reaction time (no statistically significant differences and small effect sizes) immediately after 10 purposeful headers with longer rest periods between headers. On average, participants’ visual memory scores decreased by 3.90 (95% CI=0.77-7.03) points in the control group. However, these decreases are within one standard deviation of normative data and would be unlikely to flag a patient as impaired.30 Symptom severity score also did not change despite a medium to large effect size. The symptom severity score was included although it is not a measure of cognition because it is often used as part of concussion examination, either as part of the SCAT5 or computer-based neurocognitive testing.37
Limitations and Future Directions
The results could be explained by many different factors, but there are some that could be addressed and modified in future research. The goal was to observe the effect of strengthening exercises for the neck on heading biomechanics and neurocognition from pre- to posttest. However, the protocol to strengthen the participants’ necks only strengthened the subjects’ necks in the anterior and left and right anterolateral directions. In the future, researchers may obtain different results if the strengthening exercises are selected to attempt to strengthen all directions of the neck. Neck strength was measured in either a supine or prone position as described previously.25 However, reliability and a validity of strength measures has only been measured in a seated position,26 and cannot be assumed for measurements taken in supine or prone positions. Also Lamond et al.35 found that unanticipated heading resulted in larger linear and rotational accelerations of the head than anticipated heading. It would be interesting to study the effects of neck strengthening during unanticipated head impacts as they are likely more concerning since they deliver higher accelerations to the head. Finally, neck muscle activation timing was not tested during purposeful heading impacts. Future research should determine if the timing of muscle activation is an important consideration with regards to reducing impact magnitude during purposeful heading.
CONCLUSION
The strengthening program the participants completed resulted in statistically significant improvements in anterior and anterolateral neck strength, but not in rotation or posterolateral strength. The neck strengthening protocol did not affect heading biomechanics of the collegiate soccer athletes in this study. Improving strength in the two anterior directions allowed maintenance of visual memory scores but did not alter other neurocognitive measures following repetitive soccer heading. More research should be completed to determine the role neck strength plays in reducing head injury risk.
Conflict of Interest
The authors have no conflicts to disclose.
Acknowledgments
Funded by the University of Lynchburg through the Percy Wootton Student-Faculty Research Award and the Schewel Student-Faculty Research Fund.