



INTRODUCTION
The frontal plane projection angle (FPPA) is a two-dimensional (2D) clinical measure that was developed to identify knee valgus during dynamic tasks.1,2 Although the FPPA has been questioned in terms of being able to predict non-contact ACL injury,3,4 this measurement has been shown to distinguish between persons with and without patellofemoral pain5–7 and predict acute lower-extremity injuries (hip, groin, thigh, knee, lower leg, ankle, or foot).8 Given the potential clinical usefulness of the FPPA, there has been interest in understanding its biomechanical utility in relation to traditional laboratory based measures of frontal plane knee kinematics.
To date, several studies have compared FPPA measurements and 3D knee kinematics during various tasks. Across studies, the association (R2) between the FPPA and 3D knee valgus angle has been reported to range from 0% to 64% across a wide range of tasks (i.e., single limb squat, drop jump, single leg hop, single leg land, lateral jump, and cutting).1,5,9–15 Although some authors have found that the FPPA and 3D knee valgus are correlated, the reported agreement between these angular measures is poor.16 More specifically, the FPPA has been shown to overestimate true frontal plane knee motion during a single leg squat,11 drop jump,10 and single leg hop,10 with the 95% limits of agreement ranging from -30° to 17°.10,11
The poor agreement between the FPPA and 3D frontal plane knee valgus can be explained by previous research that has shown that what appears as knee valgus on 2D video actually is a combination of sagittal, frontal, and transverse motions at the hip and knee.5,17,18 For example, studies have reported that individuals who exhibit poor frontal plane knee alignment based on visual assessment during a step down or single leg squat have increased hip adduction,17 hip flexion,17 knee external rotation,17 and hip internal rotation.18 Furthermore, an increased FPPA has been found to be correlated with increased hip adduction, knee external rotation, and hip external rotation during a single leg squat.5
While it is readily apparent that out-of-plane motions at the hip and knee compromise the ability of the FPPA to accurately represent frontal plane knee kinematics, these frontal and transverse rotations of the thigh and tibia segments may influence variables used to calculate the frontal plane knee joint moment using inverse dynamic equations (e.g., joint center location, joint angular velocities, segment accelerations, etc.). To date, two studies have evaluated the relationship between the FPPA and knee valgus moments with mixed results.12,14 Herrington et al. reported a strong relationship between the FPPA and peak knee valgus moment during the single leg step down (R2 = 42%) but not the single leg landing (R2 = 13%).12 Similarly, Mizner et al. reported a strong association between the FPPA and knee valgus moment at peak knee flexion during a double-leg drop jump (R2 = 35%).14 To date, the ability of the FPPA to predict frontal plane knee moments during tasks that involve pivoting and/or change of direction is not known. This is important as such movements have been shown to result in high knee valgus moments when compared to tasks that are more linear in nature.19
The purpose of the current study was to comprehensively evaluate the ability of the FPPA to predict the frontal plane knee kinetics (peak moment, average moment, and moment at peak knee flexion) across a wide range of tasks (stepping, landing, and change of direction). The authors hypothesized that an increased 2D FPPA would be predictive of frontal plane knee moments (i.e., increased knee valgus moments or decreased knee varus moments). Information gained from this study will advance knowledge about the clinical utility of the FPPA in characterizing movement behavior that may expose individuals to lower-extremity injury.
METHODS
Participants
The present study included a sample of 39 healthy athletes from prior studies with different study aims, as previously described.20–22 Athletes between the ages of 13 and 40 years participated (15 males: age = 23.8 (7.3) yrs., height = 1.81 (0.08) m, mass = 78.9 (16.2) kg; 24 females: age = 17.3 (6.3) yrs., height = 1.65 (0.08) m, mass = 56.1 (11.3) kg). All participants were currently partaking in a sport with high levels of jumping, cutting, or lateral movements (such as soccer, basketball, volleyball, lacrosse, football, netball, or tennis). Participants were excluded if they had current lower-extremity pain, any history of ACL reconstruction, lower-extremity injuries/surgeries in the prior six months or indicated any medical condition that would impair their ability to perform the athletic tasks.
A sample size calculation was performed in G*Power (Version 3.1) based on pilot data to determine the number of participants needed to assess the relationship between the FPPA and frontal plane knee moment across six tasks. Using a 5% significance level, 90% power, R2 value of 0.30 (based on pilot data), and 1 predictor, a minimum of 27 participants was deemed necessary.
Instrumentation
Three‐dimensional and 2D kinematic data were collected at 120 Hz using a video-based 8-camera motion analysis system (Simi Reality Motion Systems GmbH, Unterschleissheim, Germany). One of the eight cameras was positioned 80 cm off the ground (perpendicular to the force plate) and was used to collect the required frontal plane images for the 2D analysis.
Ground reaction forces were collected at 1200 Hz (Model #BP600900-2000, Advanced Mechanical Technology, Inc, Watertown, MA, USA) and synchronized with the motion capture system. The force plate was embedded into the floor and was used for five out of the six tasks evaluated. For the step-down task described below, a portable force plate was integrated into a 22 cm step (Model #O60-7000, Advanced Mechanical Technology, Inc, Watertown, MA, USA).
Procedures
Prior to data collection, participants were informed about the nature of the study and written consent was obtained as approved by the Institutional Review Board of the Health Sciences Campus at the University of Southern California. Once informed consent was obtained, participants warmed up on a stationary bike for 5-10 minutes. For all data procedures outlined below, data were obtained on the right limb.
Participants were instrumented with 17 reflective markers (10 mm diameter) on the right lower extremity, as previously described.21,22 Two-dimensional video and 3D motion analysis were collected during the following tasks: 1) Step Down, 2) Drop Jump, 3) Lateral Shuffle, 4) Deceleration, 5) Triple Hop, and 6) Side-Step-Cut. Details regarding the instructions provided to participants for each of the tasks can found in Table 1.20–22 These tasks were selected based on current knowledge of movements thought to be associated with various sport injuries. A trial was considered successful if all markers remained visible and only the foot of tested limb fully contacted the force plate. Participants were permitted to practice until comfortable with the performance of each task. One to two trials were obtained for each of the tasks.
Data Analysis
The first successful trial was selected for each task and used for data analysis. Marker position data were labeled in Simi Motion and then exported with the force data to Visual3D software (C-Motion, Inc, Germantown, MD, USA). Marker trajectory and analog force plate data were low-pass filtered at 12 Hz, using a fourth-order Butterworth filter.23 Joint angles were calculated using a X-Y-Z (sagittal-frontal-transverse) Cardan sequence.
Inverse dynamics equations were used to calculate net joint moments (external) at the knee. Moment data were normalized to body mass and height. Three frontal plane knee moment variables were extracted (peak moment, average moment, and moment at peak knee flexion). The peak and average frontal plane knee moments were calculated during the deceleration phase of all tasks (initial contact to peak knee flexion). In addition, the frontal plane knee moment at peak knee flexion was identified. For the step down, the peak and average frontal plane knee moments were calculated during the lowering phase (initiation of the movement to the time at which the heel touched the ground). For calculation of the peak moment for trials in which a valgus moment was not present, the minimum varus moment was identified and used for statistical analysis.
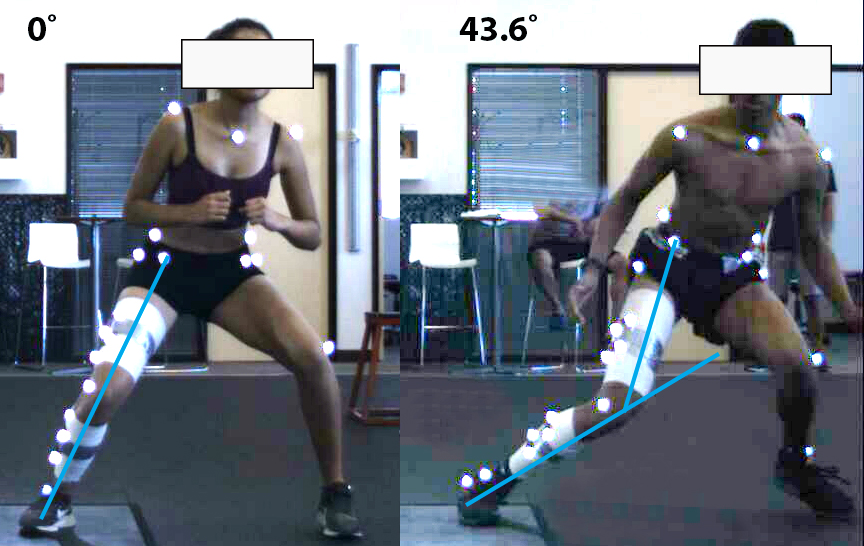
For the 2D video analysis, the image containing peak knee flexion was identified. For the step down, the image at which the contralateral heel touched the ground was used for analysis. Images were uploaded into ImageJ software (Version 1.50i, National Institute of Health, USA) for 2D angle assessments. The FPPA was measured as the angle formed by three points (ASIS, knee joint center, ankle joint center). This value was subtracted from 180 to represent the anatomical frontal plane alignment of the knee.10 A positive value represented knee valgus (knee joint center medial to a line formed from the ankle and ASIS) and a negative represented knee varus (knee joint marker lateral to a line formed from the ankle and ASIS) (Figure 1). All 2D measurements were obtained by a single investigator who demonstrated excellent intra-rater reliability for all tasks prior to the start of the study (ICCs ranging from 0.91 to 1.0).

Statistical Analysis
Linear regression analysis was used to assess the ability of the 2D FPPA angle (independent variable) to predict the frontal plane knee moment (dependent variable). This analysis was repeated for each task and was run separately for each dependent variable (peak frontal plane knee moment, average frontal plane knee moment, and frontal plane knee moment at peak knee flexion). R2 values were interpreted as strong (>= 0.50), moderate (0.25-0.49), weak (0.10-0.24), and negligible (0.0-0.09).24 All statistical analyses were performed using SPSS Version 27 (Chicago, Illinois, USA) and a custom MATLAB script (The Mathworks, Inc., Natick, MA) with alpha set at 0.05.
RESULTS
Due to technical issues with the force plate, ground reaction force data were not available for one subject during the drop jump and eight participants during the step-down task. Descriptive statistics for the FPPA, peak frontal plane knee moment, and average frontal plane knee moment for each task are presented in Figure 2. Time series data for the frontal plane knee moment are presented in Figure 3.


Relationship between FPPA and Peak Frontal Plane Knee Moment
The FPPA was found to significantly predict the peak frontal plane knee moment for deceleration (R2 = 0.12, p = 0.032) and side-step-cut (R2 = 0.25, p = 0.001), with a larger FPPA predicting increased knee valgus moments (or decreased knee varus moments). However, the FPPA did not predict the peak frontal plane knee moment for step down, drop jump, lateral shuffle, and triple hop (Figure 4).

Relationship between FPPA and Average Frontal Plane Knee Moment
The FPPA was found to significantly predict the average frontal plane knee moment for drop jump (R2 = 0.25, p = 0.001), shuffle (R2 = 0.40, p < 0.001), deceleration (R2 = 0.20, p = 0.004), triple hop (R2 = 0.15, p = 0.015), and side-step-cut (R2 = 0.31, p < 0.001), with a larger FPPA predicting increased knee valgus moments (or decreased knee varus moments). However, the FPPA did not predict the average frontal plane knee moment for step down (R2 = 0.0, p = 0.775) (Figure 5).

Relationship between FPPA and Frontal Plane Knee Moment at Peak Knee Flexion
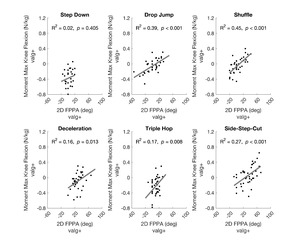
The FPPA was found to significantly predict the frontal plane knee moment at peak knee flexion for drop jump (R2 = 0.39, p < 0.001), shuffle (R2 = 0.45, p < 0.001), deceleration (R2 = 0.16, p = 0.013), triple hop (R2 = 0.17, p = 0.008), and side-step-cut (R2 = 0.27, p < 0.001), with a larger FPPA predicting increased knee valgus moments (or decreased knee varus moments). However, the FPPA did not predict the frontal plane knee moment at peak knee flexion for step down (R2 = 0.02, p = 0.41) (Figure 6).

DISCUSSION
The purpose of the current study was to comprehensively evaluate the ability of the FPPA to predict the frontal plane knee kinetics (peak moment, average moment, and moment at peak knee flexion) across a wide range of tasks (stepping, landing, and change of direction). In general, the FPPA was a better predictor of the average frontal plane knee moment (five out of six tasks) and frontal plane knee moment at peak knee flexion (5 of 6 tasks) compared to the peak frontal plane knee moment (two out of six tasks). For all significant models, an increased FPPA predicted increased knee valgus moments (or decreased knee varus moments) during landing and change of direction tasks (but not stepping). However, the strength of the predictive models was weak to moderate (R2 = 12% to 45%), highlighting that the utility of the FPPA as an indicator of frontal plane knee moments during landing and change of direction tasks is limited.
The current results are in general agreement with the findings of Herrington et al.12 and Mizner et al.,14 both of whom examined the ability of the FPPA to predict knee valgus moments during various tasks. Mizner et al. reported that an increased FPPA predicted the knee valgus moment at peak knee flexion during a drop jump task (R2 = 35%),14 which is comparable to our moment results at peak knee flexion for the drop jump (R2 = 39%). Herrington et al. reported that an increased FPPA did not predict the peak knee valgus moment during a single leg landing from a box (R2 = 13%),12 which agrees with our finding for the peak frontal plane knee moment during the triple hop (R2 = 2%). However, Herrington et al. reported that an increased FPPA predicted the peak knee valgus moment during a single leg squat (R2 = 42%),12 which is in contrast with our findings for the step down for the peak frontal plane knee moment (R2 = 1%). However, the step down and single leg squat differ in a number of kinematic variables,25 which makes direct comparisons difficult.
Across tasks, the highest R2 values were found for the average frontal knee moments and frontal plane knee moments at maximum knee flexion. Given that the FPPA was measured at peak knee flexion, it is logical that the FPPA was predictive of the frontal plane knee moment at that point in time. Additionally, the fact that peak knee flexion was used to indicate the end of the deceleration phase for each task may explain why the FPPA predictive models for the average moment during the deceleration phase were similar to those observed for the frontal plane knee moment at peak knee flexion. The ability of the FPPA to predict the peak frontal plane knee moment was limited to two of the six tasks (deceleration and cutting), with R2 values being lower than the other two variables examined. The limited ability of the FPPA to predict the peak frontal plane knee moments may be explained by the fact that the peak moment did not always occur at the same time point at which the FPPA was measured (Figure 3). As such, the timing of the kinetic variables of interest should be considered when measuring the FPPA at a single point in time.
With respect to the strength of the predictions across tasks, the step down exhibited non-significant results for all three frontal plane knee moment variables (R2 = 0-2%) ( Figure 4-6). This finding may be related to the fact that 100% of participants exhibited average knee varus moments during this movement, and this task had the lowest average frontal plane knee moment (Figure 2, Figure 5). In contrast, the strongest significant relationship was observed for the shuffle task, which had the second highest average frontal plane knee moment and a relatively large prevalence of average knee valgus moments (69% of participants) (Figure 2, Figure 5). It appears that the FPPA may be a stronger predictor of frontal plane knee kinetics when a knee valgus moment is present, with the strength of the predictability contingent on the observed frequency and magnitude of knee valgus moments. This is logical as the FPPA is indicative of inward collapse of the knee and therefore would be expected to be indicative of the variables that would be related to a knee valgus moment (i.e., medial positioning of the knee joint center, etc.).
Previous studies have reported that the FPPA is an inconsistent predictor of frontal plane knee kinematics1,5,9–15 and that the general agreement between 2D and 3D frontal plane knee angles is poor.16 Based on the current study and the work of previous authors who have evaluated the ability of the FPPA to predict frontal plane knee moments,12,14 it appears that the FPPA may be a better indicator of knee kinetics as opposed to knee kinematics. It is possible that the clinical utility of the FPPA as a predictor of injury8,26 or the ability of the FPPA to differentiate between healthy and clinical populations5–7 may lie in the fact that this measure is a predictor of frontal plane knee moments. An argument could be made that the frontal plane knee moment is more suggestive of knee loading as opposed to frontal plane knee motion.
Regarding clinical application, the current results suggest that obtaining measures of the FPPA from hand-held mobile devices (i.e.., phones, tablets, etc.) may be of value. However, it is important to note that the 2D video data obtained in the current study were captured from a fixed camera that was aligned perpendicular to the force plate. As with all measurements obtained from 2D video, there is potential for parallax error owing to the camera being positioned at an angle to the patient. Such error would influence the measurement of the FPPA and the ability to infer frontal plane knee moments as described in the current study.
There are several limitations within the current study that warrant discussion. First, these data were obtained from healthy individuals. As such, our results may not be applicable to those with specific knee conditions (i.e., patellofemoral pain, ACL injury, etc.). Second, only the deceleration or lowering phase of each task was considered in our moment analysis. Therefore, our results may not apply to the acceleration phase of the tasks evaluated. Third, the current study was cross-sectional in nature. The current results cannot be interpreted to suggest that increased FPPA angles are predictive of knee injury. Lastly, for all regression models, only a single predictor (FPPA) was examined. The R2 values reported could be improved by including other 2D measurements such as frontal plane motion at the hip, pelvis, or trunk.27
Conclusion
In summary, the results of the current study suggest that the FPPA is a predictor of frontal plane knee loading during landing and change in direction tasks, specifically when the frontal plane knee moment is calculated as the average moment or the moment at peak knee flexion. For all significant models, an increased FPPA (indicative of medial knee collapse) predicted increased knee valgus moments (or decreased knee varus moments) during landing and change of direction tasks (but not stepping). However, the ability of the FPPA to predict frontal plane knee kinetics appears to be task dependent, with the strength of the prediction improved with increased frequency and magnitude of observed knee valgus moments. In addition, the strength of the prediction was weak to moderate, highlighting that the validity of the FPPA as a predictor of frontal plane knee moments during landing and change of direction tasks is limited.
Conflicts of interest
The authors have no conflicts of interest to disclose.