BACKGROUND
Musculoskeletal injuries among dancers represent a major concern.1–4 In addition to being associated with serious physical and psychological disabilities in athletes, injuries can represent an extensive financial burden on health care systems.5 In order to better understand the underlying pathokinesiology of non-traumatic injuries among dancers, researchers have focused on specific, segmental impairments identified as potential risk factors in other athlete populations.6–9 These risk factors include lower or delayed activation of the transversus abdominis muscle (TrA),6–8 as well as reduced hip and knee muscle strength.9 However, with prevention of injuries in mind, there has been a continued interest in the evaluation of movement competency in recent years, as opposed to specific segmental impairments assessments.10 This shift in approach has given rise to the development of movement competency screening tools.11–14 Movement competency can be defined as the ability to achieve fundamental movements without any functional deficits.15 Strength and motor control are key to preventing faulty movement patterns. For instance, the activation of the TrA and having stronger lower limb muscles have been linked to movement competency.16 The evaluation of movement competency using screening tools has enabled the identification of athletes and workers at risk of injuries.17,18
Among the multiple movement competency screening tools that have been developed, the Functional Movement Screen (FMSTM) and the Movement Competency Screen (MCS) have been investigated.16–21 The MCS was developed and validated for athletes and dancers.16,17,21 It has the interesting characteristic of evaluating different load levels during the performance of movements used in rehabilitation and training programs. Out of 11 movement competency assessment tools reported in the literature, the MCS was identified among the most promising to assess performance capabilities in terms of applicability and the rigor with which it was developed.22 In the original version of the MCS, Kritz described load grades as being scored using a 5-level scoring system : (1) assisted loading, (2) bodyweight loading, (3) external loading, (4) eccentric loading, and (5) plyometric loading.21 According to the currently accepted method for scoring the MCS, those five levels are regrouped into three levels as follows : (1) assisted and bodyweight loading, (2) external and eccentric loading, and (3) plyometric loading.21
The 3-level scoring system thus collapses the five levels into three levels. For example, a movement performed with certain compensations could be rated as a 3 or a 4 on the 5-level system, while on the 3-level scoring system it would be rated as a 2. This appears to be less than optimal since the merging of load levels results in a loss of detailed information. The 5-level scoring system would allow greater precision and, as a result, would more accurately characterize movement competency. The strength of the MCS compared to other movement competency screening tools is the use of load levels. It should therefore be accounted for in detail in the scoring method.
The aim of this technical note was to investigate, in a sample of dancers, and for each MCS scoring system (1) the internal consistency between items and (2) their association with TrA activation, hip strength, and FMSTM total score. It was hypothesized that the 5-level scoring system would show better psychometric properties in terms of internal consistency and concurrent validity as assessed by association with key components of movement competency and another validated movement competency tool.
DESCRIPTION
Data for this study were gathered at one time point prior to the beginning of the 2018-2019 and 2019-2020 dance season and were derived from a prospective cohort study involving 118 dancers, varying in dance style (ballet and contemporary) and status (professional and pre-professional). Dancers were recruited following a presentation of the research project in multiple dance schools and companies. This study was approved by the institutional review board and each participant gave written informed consent. Participants had to be at least 16 years old and had to dance professionally or pre-professionally for at least 10 hours per week. They were excluded if they were pregnant because of the impact on the lumbopelvic muscles, or if they had a musculoskeletal disorder that restricted dancing at the time of the evaluation. Participants underwent an assessment conducted by an experienced physiotherapist who has been a dancer for 17 years, a dance educator for eight years and who treats dancers in her regular practice. The assessment included the evaluation of TrA activation, hip strength, and movement competency. The evaluation was done on-site in dance schools or companies, either in a dance studio or in a physiotherapist’s office if one was available.
Independent variables
The preferential activation ratio of the TrA was evaluated using ultrasound imaging (GE LOGIQ E, GE Healthcare, Milwaukee, Wisconsin, 13 MHz linear probe in B-mode) in a standardized position.23–25 Dancers were in a supine position with both knees at a 90° flexion. The probe was positioned between the axillary and mamillary lines, at mid-distance between the iliac crest and 12th rib in a transverse plane. The preferential activation ratio is calculated to take into account the activation of the internal and external obliques. This method thus considers the possible compensations of these muscles. Both sides were assessed three times and a mean value was obtained.
Preferential activation ratio= (TrAcontxAbdoLatWallcontx)−(TrArestAbdoLatWallrest)(TrArestAbdoLatWallrest)
The strength of the hip flexors, extensors, abductors, adductors, and external and internal rotators were measured in a standardized position using a handheld dynamometer secured with straps.26 The exact positions used are described in a previous study.16 Both sides were assessed three times with a 30 second break in between each measurement. A mean value was obtained and used for analysis.
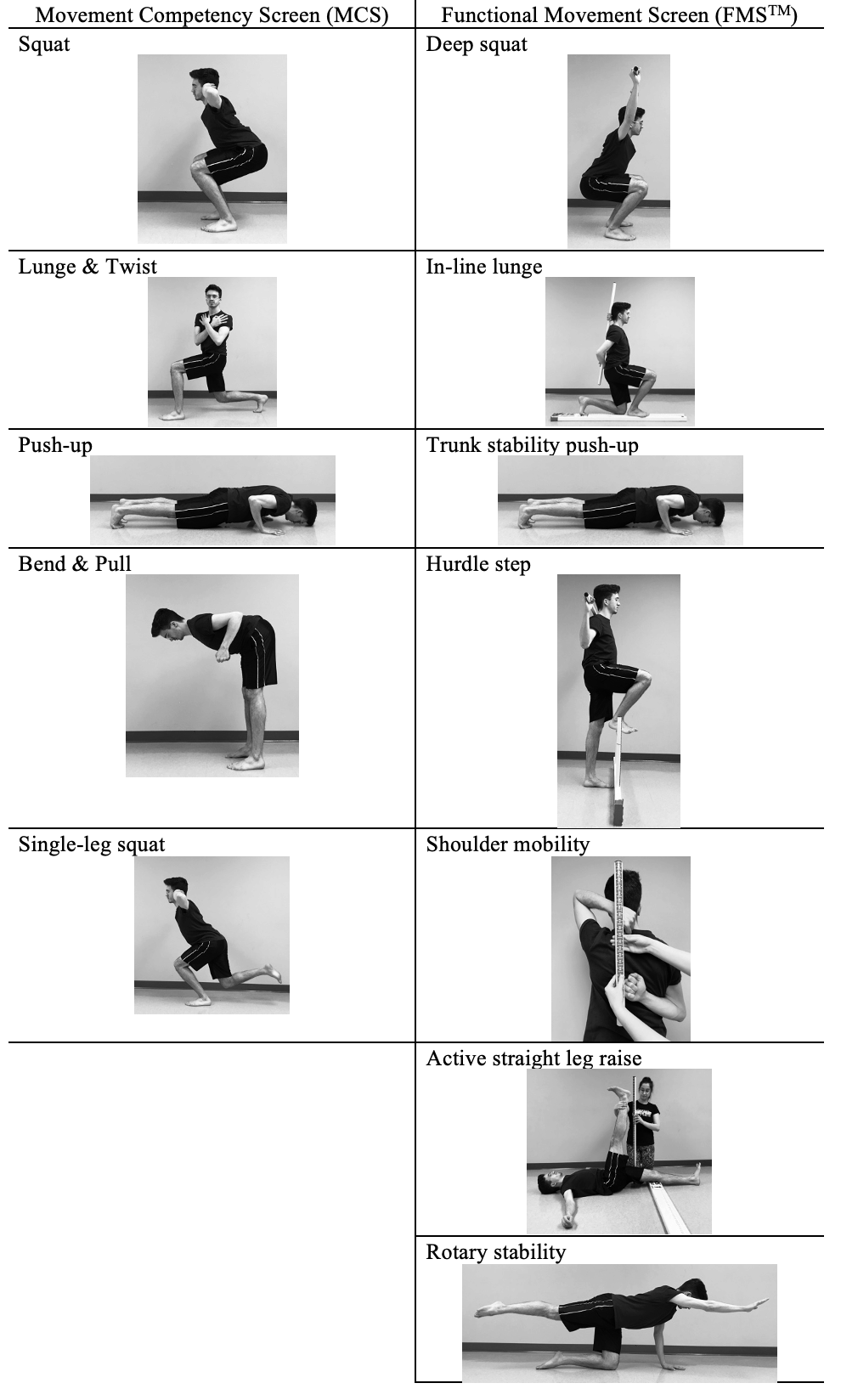
Movement competency was screened using two distinct instruments, the FMSTM and the MCS.17–21 The MCS is composed of five tasks designed to assess global movement competency: (1) squat, (2) lunge and twist, (3) bend and pull, (4) push-up and (5) single-leg squat. The lunge and twist, and the bend and pull are subdivided into the individual components of each movement. Therefore, there are seven items to be evaluated. Each item has a set of possible primary and secondary compensations. The scoring is completed by evaluating the number of compensations observed. More frequent compensations result in a lower score. Additionally, primary compensations are more detrimental to the score than secondary compensations. The tasks of the MCS can be completed with multiple load levels, according to the evaluator’s judgement. The movement can be completed slowly, rapidly, or using plyometrics. As per the accepted scoring system, the 3-level score is attributed only according to the compensations observed, with no discrimination between assisted and bodyweight loading or external and eccentric loading. The MCS was scored using both the 5-level scoring system that uses separate load levels (assisted, bodyweight, external, eccentric, and plyometric) and the 3-level scoring system in which they are grouped as described above. The FMSTM does not include different load levels. Each movement is done at a slow pace. Figure 1 shows a comparison between the movements from the MCS and the FMSTM.

Statistical analysis
Statistical analyses were conducted in SPSS 28.0. Cronbach’s alpha was first calculated for items scored with the 5-level system and then, for items scored with the 3-level system, to assess internal consistency. To identify the scoring system that best suited the variables, simple linear regressions were first used for the 5-level and then for the 3-level scoring system. FMS scores, TrA activation, and hip strength were used as independent variables. Each independent variable’s association with movement competency was examined, as well as the proportion of variance for the total MCS score that they each explained. A multiple regression model was built which included the variables significantly associated with the MCS score for each scoring system. Therefore, a different model was built for the 5-level and 3-level systems since the results from the simple regression analyses identified different variables as being associated with the dependent variables. Since dance hours could be a potential confounder in the analyses, each linear regression was controlled for this variable. The level of significance for all statistical analyses was set at p≤0.05. Statistical assumptions were met for each linear regression completed.
OUTCOMES
The sample was composed of 118 preprofessional and professional dancers. Table 1 presents demographic information. No adverse events occurred during the evaluations.
Table 2 presents the results of separate linear regressions between each independent variable and the MCS total score, where each item was scored using either the 5-level system or the 3-level system.
The 5-level scoring system as the dependent variable
The internal consistency assessed with Cronbach’s alpha for the seven items of the MCS scored with the 5-level system was 0.548. It was found using simple linear regressions that TrA activation, hip extensor, abductor, adductor, and external rotator strength, as well as FMSTM total score (β=0.455, p<0.001) were statistically significantly associated with the MCS total score as measured by the 5-level scoring system. Given multicollinearity between hip strength variables in the multiple linear regression model, only hip adductor strength was introduced in the model. This variable was chosen since it was the most significantly and strongly associated with the MCS total score. As seen in Table 3, the multivariate model accounted for 24% of the variance for the MCS scored on the 5-level system (F=13.324, p<0.001).
The 3-level scoring system as the dependent variable
Regarding the internal consistency, Cronbach’s alpha for the seven items of the 3-level scoring system was 0.494. Simple linear regression analyses revealed significant associations with hip internal rotator strength and FMSTM total score (β=0.250, p=0.006) with the MCS total scored on a 3-level system. Results showed that the multiple linear regression model built accounted for 13.3% of the variance for the MCS on a 3-level scoring system (F=9.959, p<0.001).
DISCUSSION
The purpose of this study was to examine the internal consistency for the items scored with each system and to explore if the association of TrA activation, hip muscle strength, and FMS score was higher with the 5-level scoring system, as opposed to the 3-level scoring system.
Although both point systems did not have a Cronbach’s alpha that exceeded the generally accepted value of 0.7 as acceptable internal consistency,27 the 5-level system showed a moderate internal consistency (≥0.5) and the 3-level scoring system showed a poor internal consistency (<0.5).28 This supports the hypothesis that the 5-level scoring system would show higher internal consistency than the 3-level scoring system.
Findings from a previous study on the correlations between the MCS total score (3-level scoring) and TrA activation, hip strength, and FMS showed significant associations.16 However, linear regressions for the 3-level scoring system in the current study did not reveal significant association with TrA activation or hip strength, with the exception of internal rotators.16 In the present study, the model with the 3-level system as the dependent variable explained only 13.3% of the variance. In a previous model using the 3-level system, similar independent variables could explain only 10.8% of the variance.16 In the current study, it was found that 24% of the variance for the total MCS score using the 5-level system could be explained by the independent variables selected. These results are of particular interest because they show that the variance of the 5-level scoring system is explained in a greater proportion by components that have been identified as key to movement competency. This supports the assumption that the 5-level scoring system shows higher concurrent validity.
This study is not the first to reconsider the MCS scoring. Instead of using the common 3-level scoring for only the weaker side, Lee et al. used the 3-level scoring system for both sides and added up the points, giving a 6-level score for each task.17 The reasoning behind this choice is unfortunately not explained in the article. Considering both sides when evaluating each MCS item could lead to a higher score and to an overestimation of the athlete’s physical abilities when one side scores higher than the other. This method using the 3-level scoring system still presents the problem of grouping the five initial load levels. Results from the current study support the use of a 5-level scoring system to obtain more precise measurement of movement competency. Taking both sides into account when evaluating athletes could be considered; but to group this information in a total score could also mean overestimation of the athlete’s movement competency. Future research should consider the benefits and risks associated with an inflated movement competency score when considering both sides.
The main limitation of this study is the inclusion of dancers practicing various types of dance. Indeed, the inclusion of ballet and contemporary, as well as preprofessional and professional dancers could lead to increased heterogeneity in the dancers’ characteristics that are inherent to dance style and/or level of experience. The sample size could not allow analysis of these subgroups. However, this heterogeneity increased external validity.
CONCLUSION
The items scored with the 5-level system showed higher internal consistency of the test scores than with the 3-level system. Simple and multiple linear regressions used in the present technical note indicate that a 5-level system is more representative of the essential components of movement competency than the commonly used 3-level system because of its higher and more significant association with TrA activation, hip strength, and FMSTM score. For these reasons, health professionals and researchers should consider using the 5-level scoring system of the MCS in future clinical settings and research.
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
FUNDING
This study was funded by a partnership between the Institut de recherche Robert-Sauvé en santé et sécurité du travail (IRSST) and REPAR (03SNT007).