


INTRODUCTION
Myofascial trigger points (MTrPs) have been identified as a potential source of musculoskeletal dysfunction.1–5 Myofascial trigger points have been defined as hyperirritable and palpable nodules within a taut band of muscle and are classified as either active trigger points or latent trigger points.6 Active trigger points can cause localized pain that is spontaneous in nature,4,5 while latent trigger points are not spontaneously painful and will only elicit pain when palpated.3–5 Some authors have argued that latent trigger points have the same pathophysiology as active trigger points, just to a lesser extent,3–5,7 which may explain a reduction in nociceptive input without mechanical stimulus.8–10
Most of the research on MTrPs has focused on active trigger points due to their ability to generate spontaneous pain without being palpated, even though latent trigger points are more commonly found in muscle tissue.11,12 Despite a lack of attention in the literature, latent trigger points are not without clinical significance. Regarding function, they have been found to increase muscle fatigability,13 decrease muscle strength,14 and alter muscle activation patterns.1,15 Furthermore, latent trigger points may have the potential to transition into active trigger points if left untreated.7
Trigger point dry needling (TDN) has become an increasingly popular intervention among physical therapists to reverse the effects of MTrPs.16,17 Authors of previous studies have demonstrated a reduction in substance P and calcitonin related peptide levels, while blood flow and subsequent tissue oxygenation increased following the application of TDN to MTrPs.8,18 However, there is still debate surrounding the effectiveness of TDN provided by physical therapists as a viable treatment option for musculoskeletal dysfunction as compared to other physical therapy interventions.19
A potential cause for the formation of MTrPs has hypothesized to be repetitive or unaccustomed eccentric loading of muscle tissue.4,5,7,20–22 Musculature such as the gluteus medius must eccentrically control motion of the pelvis within the frontal plane during the gait cycle23 or during other functional activities where single limb support is required.24 Subtle alterations in frontal plane gait kinematics may lead to excessive loading of the gluteus medius musculature, which in turn may lead to the formation of MTrPs. If latent trigger points are able to affect muscle function, then an asymptomatic individual may have altered stability of the pelvis and the hip during loading response of the gait and running cycles, which then has the potential to alter the alignment of the lower limb relative to the ground.
Despite the increased demand for eccentric control during functional activities, such as ambulation, there are no studies that have investigated the effects of latent trigger points on the strength of the gluteus medius. Furthermore, studies that have investigated changes in strength of lower extremity musculature following the application of dry needling to MTrPs report conflicting results.25–32 The purpose of this study was to investigate whether the application of TDN to latent trigger points within the gluteus medius musculature affected strength measurements and muscle activation levels immediately following intervention.
METHODS
Study Design
This quasi-experimental study used a single group, pretest-posttest, randomized control design (ww.ClinicalTrials.gov, ID NCT03580200). The study was approved by the Human Research Protections Program at the University of Indianapolis and a reliance agreement was enacted with Mount St Joseph University in Cincinnati, OH where data were collected.
Participants
A convenience sample of males and females age 18 to 50 years old were recruited provided they were asymptomatic at the time of screening and data collection. Asymptomatic was defined as experiencing no pain in the lumbar spine, sacroiliac region, pelvis, or bilateral lower extremities while at rest or with activity. Participants were excluded if they had one of the following: were pregnant or attempting to become pregnant; pain intensity greater than 0 out of 10 on the visual analogue scale in the lumbar spine, sacroiliac region, pelvis, and bilateral lower extremities at rest or with activity; positive Flexion Adduction Internal Rotation test (FADIR)33 on either the left or right hip; presented with signs and symptoms consistent with hip osteoarthritis during clinical screening using the criteria proposed by Altman et al.34; diagnosed with a progressive neurological disorder, a chronic pain condition such as fibromyalgia or myofascial pain syndrome, a connective tissue disorder, or osteoarthritis of the hip joint; history of hip dysplasia or Legg Calve Perthes disease.
Informed consent was obtained following eligibility screening but immediately prior to data collection. The primary investigator (PI), a licensed physical therapist with 13 years of clinical experience was responsible for data collection and the application of TDN for all participants throughout the study.
Randomization
A simple randomizing method of flipping a coin was used to assign each participant an intervention side, which was the side of the body that received TDN, and a control side, which was the side of the body that did not receive TDN.
Outcome Measures
Strength of the gluteus medius muscle was defined as the amount of force output measured by a handheld dynamometer (HHD) during a maximal volitional isometric contraction (MVIC) break test.35–37 Force output was measured in kilograms (kg) using a microFET2 HHD (Hoggan Scientific, LLC, Salt Lake City, UT) on both the control and intervention sides. The HHD is commonly used to assess force production and has been shown to be a reliable and valid measurement tool for assessing strength of the lower extremity musculature.36,38–40
Surface electromyography (sEMG) amplitude readings of the gluteus medius were recorded at the same time as HHD measurements on both the control and intervention sides. Raw sEMG data were collected using a two-channel sEMG recording system (MP36R, Biopac, Goleta, CA) and were measured in millivolts (mV). Parameters for recording the raw sEMG data included a rejection ratio of > 110 dB at 60 Hz, a gain of 1000 Hz, band pass filtered at 20-450 Hz, and a sampling rate of 2000 Hz.37,41,42 Recorded sEMG amplitude readings can be used as a direct measure of the activation level of a muscle during a contraction43–45 and is a common method of assessing the activation level of the gluteus medius muscle during a MVIC as well as dynamic movements.37,41,42,46–48
Prior to the start of data collection, intrarater and test-retest reliability was established for the PI’s HHD and sEMG measurements during MVIC break testing of the gluteus medius. Ten participants with characteristics consistent with the study’s sample were recruited. A 10-minute break was given between measurements. All calculated ICCs (3, 1) were greater than .75 indicating acceptable intrarater and test-retest reliability49 (Table 1).
Testing Procedure
Bipolar sEMG electrodes were placed 2 cm apart in a position distal to the iliac crest, midway between the anterior and posterior superior iliac spines and in line with the proximal tip of the greater trochanter.41,42 A reference electrode was placed on the greater trochanter (Figure 1). Electrode placement on the intervention side was marked by a sterile surgical pen as electrodes needed to be removed during the application of TDN.

To ensure that the participant understood the position of testing, the leg to be tested was passively moved in to the testing position with verbal cueing. The pelvis was kept from rotating backwards by a manual stabilization force placed on the posterior and lateral iliac crest.35,36 The participant was then asked to assume the testing position without assistance, but with standardized verbal cueing from the PI. After the participant successfully achieved the proper position for testing without compensation on three consecutive attempts, a trial MVIC break test was performed.
Application of TDN to the gluteus medius was not limited to one specific region of the muscle. As such, all subdivisions of the gluteus medius muscle needed to be active during each MVIC break test. Using the recommendations of Otten et al.37 the hip was placed in two separate testing positions that were found to have the highest sEMG activation levels for all three subdivisions of the gluteus medius. Participants were positioned in side lying with their bottom or stabilization leg in a position of approximately 30 degrees of hip flexion and 90 degrees of knee flexion. The first testing position had the hip on the side being tested in a neutral or zero starting position (SL0) at the hip with the knee fully extended. Neutral or zero starting position was defined as a position where the hip is in neutral position with respect to hip flexion and extension, abduction and adduction, as well as internal rotation and external rotation (Figure 2). The second testing position had the hip in a position of neutral hip flexion and extension as well as abduction and adduction, but the hip was maximally internally rotated (SLIR) with the knee fully extended (Figure 3).


The resistance applied during each MVIC break test was applied gradually until maximal resistance was provided for a total of five seconds, or until the participant could no longer hold the testing position.35 To standardize the resistance applied for each trial as well as each participant, the entire body weight of the PI was placed 4 cm proximal to the lateral malleolus.35,36 The exact position of where the pressure should be placed was measured and marked on both the control and intervention sides.
Three MVIC break tests were performed first on the control side and then the intervention side. One minute of rest was given in between each test for both the SL0 and SLIR positions in an attempt to reduce the effects of muscular fatigue.47 If compensatory movements were observed during the recording of a strength measurement, the measure obtained was not recorded, the form was corrected and another test was performed. Once three valid tests were performed on the control and intervention each side, the HHD values were averaged.14,36 Following application of TDN, the same procedure for measuring strength and muscle activation levels of the gluteus medius was repeated.
Intervention
Following the pre-TDN measurement of gluteus medius strength and muscle activation levels, latent trigger points were identified in the gluteus medius musculature on both the control and intervention sides using the methods proposed by Simons et al.20 Each participant was positioned in side lying with the hip on the side that was assessed in a slightly adducted position so normal muscle fibers were still on slack while the taut bands of muscle were placed under tension, which made them more easily palpable.11,12,14,15
Participants needed at least two latent trigger points in the gluteus medius muscle on the intervention side in order to receive TDN.14 Trigger point dry needling was applied to each of the identified latent trigger points in an attempt to elicit a localized twitch response (LTR). Once a LTR was elicited, the needle was manipulated either further into the muscle tissue or at a different angle until no more LTRs were elicited, or if the participant verbally requested the intervention to stop. Once the needle was removed, manual pressure was held at the site of needle insertion for a total of 30 seconds to achieve hemostasis.25,29 The same process was repeated for all identified latent trigger points within the gluteus medius muscle. The application of TDN was stopped when no more LTR were elicited and there were no more palpable latent trigger points.
Following the application of TDN, each participant was asked to stand up and walk for two minutes in an attempt to assess each participants’ level of soreness with functional movement. Time was managed by the PI for standardization purposes. Following the two minutes, participants were asked to rate their level of soreness on a 0 to 10 scale with a response of 0 representing, “No soreness at all” and a response of 10 representing, “The worst soreness imaginable”.
Data Management
Biopac Student Lab software (Biopac, Goleta, CA) was used to analyze the recorded sEMG data. Raw sEMG readings were visually inspected and the peak amplitude that occurred during each MVIC was identified. Readings were then transformed using a root mean square calculation. Data were smoothed over 1000 points representing a 500 ms window around the identified peak amplitude, 250 ms prior to the peak and 250 ms following the peak.43 If the 500 ms window included readings that were not part of the MVIC, the next closest peak within the MVIC was identified and used. The mean amplitude within the 500 ms window was recorded for each trial.
Once a mean sEMG amplitude was found for each trial, the three trials in the SL0 and SLIR positions were averaged and recorded for both the intervention and control sides. The recorded HHD force measurements for all three trials in each position were also averaged and recorded for both sides. This process was performed for all measurements recorded prior to and following the application of TDN. The averaged values for the sEMG and HHD measurements were used for statistical analysis.
In order to be compared between trials or between individuals, sEMG readings must be normalized.44,45 The method of normalization has been debated, but normalization using a MVIC is a widely used44 and reliable method47 of comparing sEMG readings of the gluteus medius. The resultant sEMG data for measurements recorded prior to the application of TDN were used as the 100% MVIC reference for both the intervention and control sides. Averaged sEMG measurements recorded following the application of TDN were expressed as a percentage of the 100% MVIC.
Statistical Analysis
An a priori sample size estimation was conducted based on using a repeated measures ANOVA, analyzing the between-within interaction effect of four measurements between two groups and the following parameters, two-tailed test, alpha of 0.05, power of 0.80, a moderate effect size of 0.20. A minimum sample size of 36 participants was needed. To account for a potential participant dropout rate of 10% as well as individuals not presenting with latent trigger points in the gluteus medius when palpated, 40 participants were recruited.
All data were analyzed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY). Normality of the data was determined using the Shapiro-Wilk test. All comparisons were two-tailed and an alpha level of less than 0.05 was considered statistically significant unless otherwise noted. Effect sizes were interpreted using the recommendations of Cohen.50 Descriptive statistics were used to describe the baseline characteristics of the sample.
A two-way repeated measures ANOVA was used to assess if there was a significant interaction between time (pre-TDN and post-TDN) and groups (intervention side and control side) for HHD force measurements for the SL0 and SLIR positions. Post hoc analysis using paired t tests with a Bonferroni correction (alpha level of p < 0.013) were used to identify which pairs had a significant difference. Effect size of the interaction between time and groups were calculated (partial eta squared).
To assess whether there was a significant difference in sEMG measurements within the intervention side and the control side over time as well as between sides prior to and following the application of TDN, pairwise tests were conducted for both the SL0 and SLIR positions. Since sEMG data were not normally distributed, Wilcoxon signed-ranks tests with Bonferroni correction (alpha level of p < 0.013) were conducted. Effect sizes for the results of the Wilcoxon signed-ranks test were calculated (Cohen’s d) using the recommendations of Field.51
RESULTS
Description of Sample
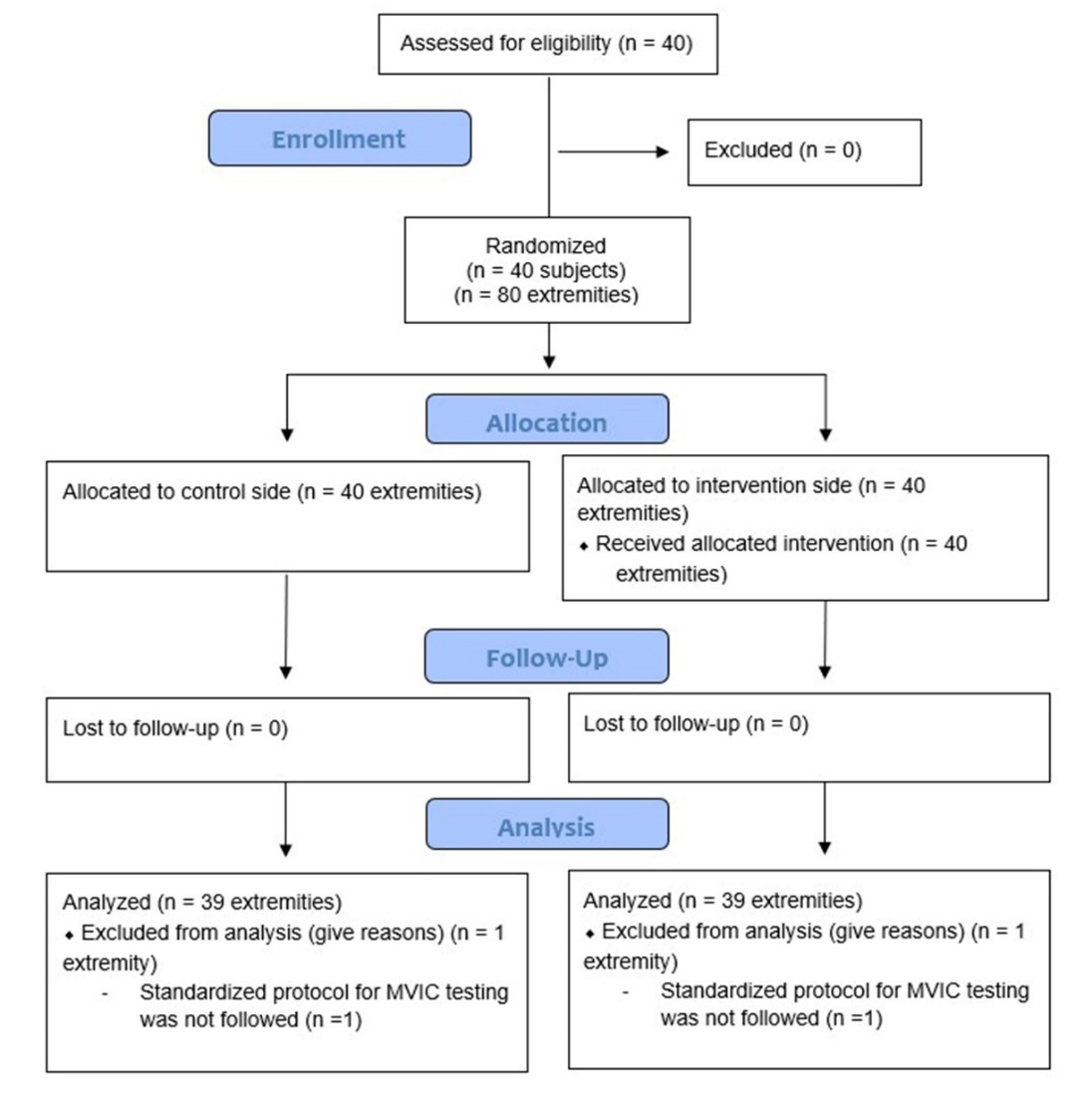
Forty participants were recruited and met the inclusion criteria for the study. One participant’s results were excluded due to the protocol for data collection not being followed (Figure 4). Therefore, the total sample size for the study was 39 participants. Descriptive statistics for the baseline characteristics of the sample can be found in Table 2.

Hand Held Dynamometer
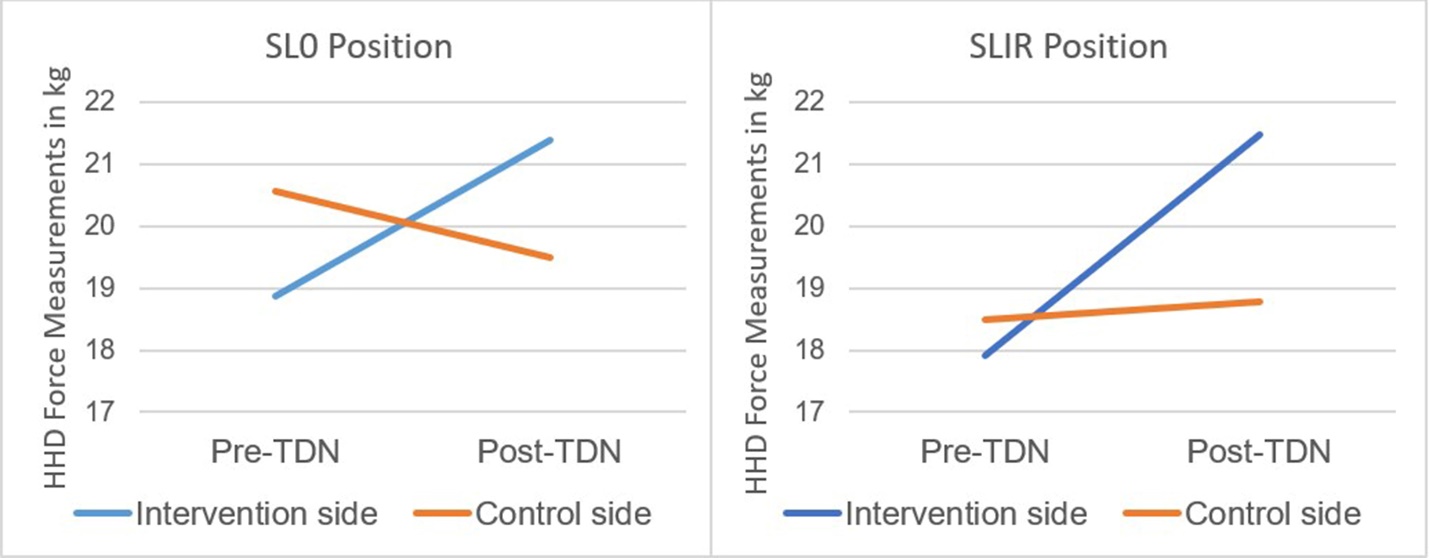
Hand held dynamometer measurements of force for the intervention and control sides for both the SL0 and SLIR positions are presented in Table 3 and Figure 5. There was a statistically significant interaction between the time (pre-TDN to post-TDN) and groups (intervention side and control side) for both positions, SL0 position, F(1,38) = 107.89, p < 0.001 and SLIR position, F(1,38) = 93.37, p < 0.001. The overall effect sizes were large for the interactions in the SL0 position (partial eta squared = 0.74) and the SLIR position (partial eta squared = 0.71).

Pairwise post hoc analyses were statistically significant (p < 0.001) for all comparisons in the SL0 position: pre-TDN to post-TDN within and between the intervention side and the control side for both time periods. For the SLIR position, there was a statistically significant difference (p < 0.001) for pre-TDN and post-TDN measurements within the intervention side and between the intervention and control side for the post-TDN measurements. There was no significant difference (p = 0.146) within the control side when comparing pre-TDN and post TDN measurements, or when comparing pre-TDN measurements between the intervention and control sides (p = 0.074).
Hand held dynamometer measurements for the control side in the SL0 position decreased by 1.31 kg following the application of TDN. Three separate paired t tests were used to assess differences between the three trials of HHD measurements taken on the control side following the application of TDN. Significant differences were found for the measurements recorded between trial 1 and trial 2 (mean difference = -0.71, t(38) = -2.42, p = 0.020) and trial 1 and trial 3 (mean difference = -0.97, t(38) = -3.60, p = 0.001). No significant difference was found between measurements recorded for trial 2 and trial 3 (mean difference = -0.26, t(38) = -1.08, p = 0.287).
Surface Electromyography
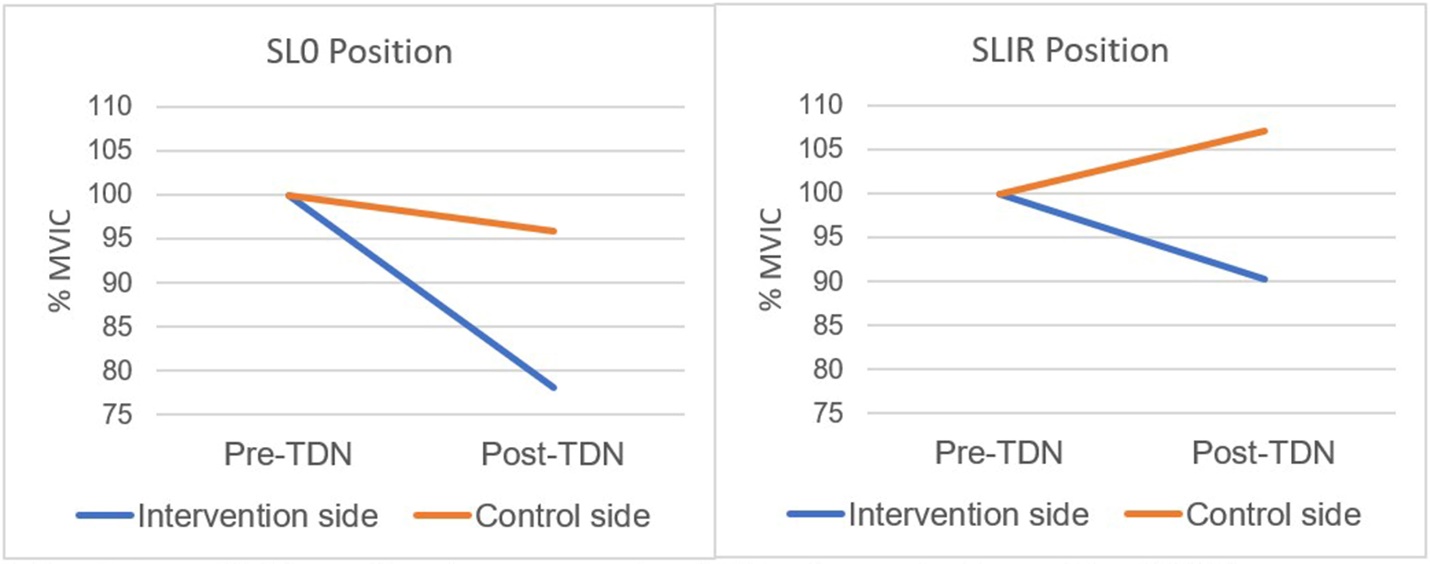
Surface EMG measurements of amplitude for the intervention and control sides for both positions are presented in Table 4 and Figure 6. Within group analysis revealed a statistically significant difference between pre-TDN and post-TDN sEMG amplitude measurements on the intervention side in the SL0 position Z(39) = - 2.60, p = 0.009 with a medium effect size (Cohen’s d = 0.62). There were no statistically significant differences between pre-TDN and post-TDN sEMG amplitude measurements in the SL0 position on the control side, Z(39) = -1.46, p = 0.145. For the SLIR position, there was no statistically significant difference within either the intervention side, Z(39) = -2.09, p = 0.037 or the control side, Z(39) = -1.00, p = 0.317.

Between TDN group comparisons for the SL0 position revealed there was not a statistically significant difference in pre-TDN sEMG amplitude measurements between the intervention side and control side, Z(39) = -1.17, p = 0.241. However, there was a statistically significant difference in post-TDN sEMG amplitude measurements between the intervention side and control side in the SL0 position, Z(39) = -3.08, p = 0.002 with a medium effect size (Cohen’s d = 0.74). In the SLIR position, the difference between the intervention side and control side at pre-TDN and post-TDN was not statistically significant, Z(39) = -0.27, p = 0.786 and Z(39) = -0.20, p = 0.042, respectively.
DISCUSSION
The purpose of this study was to investigate whether the application of TDN to latent trigger points within the gluteus medius musculature affected strength measurements and muscle activation levels immediately following intervention. Participants within this study had to be asymptomatic to ensure that the latent trigger points themselves were the sole reason for muscle weakness, not pain or articular dysfunction. Furthermore, to specifically assess the effect that TDN had on strength measurements, it had to be completed in isolation of any other therapeutic intervention. As such, this is the first study to investigate the effects of TDN in isolation on strength measurements of the gluteus medius in asymptomatic individuals.
Results reported from previous research assessing the effect of TDN to latent trigger points in the gastrocnemius found no significant difference in strength measurements as measured by a HHD immediately following intervention.25,26 In contrast, participants within this study demonstrated a statistically significant increase in HHD measurements of gluteus medius force production immediately following the application of TDN in both testing positions. While the minimal clinically important difference for HHD measurements of the gluteus medius muscle has not been established,52,53 a large treatment effect size was found for interactions in the SL0 position (partial eta squared = 0.74) and the SLIR position (partial eta squared = 0.71) following the application of TDN suggesting a strong relationship between intervention and the difference in HHD measurements over time as well as between groups. These results are consistent with previous studies that investigated immediate changes in force production of hip musculature measured by a HHD following the application of dry needling to MTrPs in the lower extremities for both symptomatic29,30 and asymptomatic individuals when combined with other interventions.31
Strength as measured by HHD force measurements was not the only outcome measure utilized in this study. Participants demonstrated a statistically significant decrease (78.17% of pre-TDN readings) in sEMG amplitude readings on the intervention side following the application of TDN even though HHD force measurements increased by 2.52 kg in the SL0 position. While not statistically significant, sEMG amplitude readings in the SLIR position also decreased (90.32% of pre-TDN readings) on the intervention side, while HHD force measurements increased by 3.38 kg. Recorded sEMG amplitude readings can be used as a direct measure of the activation level of a muscle during a contraction.43–45 Both Dwyer et al54 and Penney et al41 found an increase in sEMG amplitude readings recorded during functional activities for individuals who demonstrated weakness of the gluteus medius muscle during baseline testing. These results suggest individuals who present with weakness of a muscle will require an increased level of muscle activation during a contraction, which may be a compensatory mechanism used to increase the amount of motor unit recruitment in order to achieve a given force output.55 As such, the inverse relationship of HHD force measurements and sEMG amplitude readings found in this study suggests a more efficient gluteus medius muscle contraction following the application of TDN, as participants required less motor unit recruitment to achieve greater levels of force production.
Based on the results of this study, latent trigger points can be identified as a potential source for impaired muscle function of the gluteus medius muscle resulting in a weak and inefficient muscle contraction. Authors of previous research have stressed the importance of eliciting a LTR during TDN to ensure that the myofilament needle has come in contact with a myofascial trigger point.56,57 While it is still unclear if the elicitation of one or multiple LTRs during the application of dry needling is essential for reductions in pain and disability in various patient populations,58,59 the purpose of this study was to investigate the effects of TDN specifically to latent trigger points within the gluteus medius muscle. As such, it was critical that a LTR was elicited during the application of TDN to ensure that the needle had in fact come in contact with a latent trigger point.25,26,32 All of the study participants demonstrated a palpable LTR and subjectively reported feeling a LTR during the application of TDN.
The exact mechanism of how TDN can reverse the effects of MTrPs is still unknown.5 Following the application of dry needling as well as the elicitation of a LTR, an increase in blood flow and subsequent tissue oxygenation have been found, along with a reduction of the biochemicals associated with pain and a localized muscle contraction within the milieu of a myofascial trigger point.8,18 Increases in localized blood flow and biochemical changes within the tissue itself may explain the increase in force production following the application of TDN observed during this study. Specifically, a reduction of calcitonin gene related peptide may allow for improved overlap of actin and myosin proteins through elimination of the localized muscle contracture22 which has the potential to improve cross bridge formation within the sarcomere unit, thereby improving muscle force production. Furthermore, Lucas1 argued that a reduction of group III and IV afferent input to second order neurons could potentially reverse alpha motor neuron inhibition, thereby improving neuromuscular control which may further explain the inverse relationship between HHD force measurements and sEMG amplitude readings found in this study following the application of TDN. Similarly, changes in neuromuscular function including a reduction in resting muscle tone25,26 as well as a decrease in muscle contraction time25 have been found following the elicitation of a LTR during the application of TDN to latent trigger points within the gastrocnemius.
An unexpected outcome of the study was that there was also a statistically significant difference in HHD measurements for the control side in the SL0 position as force measurements decreased by 1.31 kg. A possible explanation for this result could be found in the order in which the strength measurements were recorded and the level of soreness experienced following the application of TDN. Post-TDN strength assessments were completed first on the control side and then the intervention side. Participants reported an increased level of soreness in the gluteus medius muscle on the intervention side during the first MVIC break test trial on their control side while in the SL0 position. Even though strength was being assessed on the control side, participants reported an increased level of soreness on the side that they were lying on potentially due to the need for stabilization during testing. Post needling soreness is commonly reported following the application of TDN58 and may have affected the participants’ ability to generate force during their first MVIC break test trial on the control side in the SL0 position.
To support this explanation, post-TDN HHD force measurements of all three trials in the SL0 position on the control side were analyzed for differences. Significant differences for the measurements recorded between trial 1 and trial 2 and trial 1 and trial 3, while no significant difference was found between measurements recorded for trial 2 and trial 3. It is plausible that the level of soreness experienced in the gluteus medius musculature following the application of TDN reduced with each subsequent MVIC break test trial. This phenomenon may explain why there was no significant difference found between measurements recoded for trial 2 and trial 3 in the SL0 position as well as no significant difference between any of the measurements recorded in the SLIR position on the control side, which were collected following the measurements in the SL0 position. Clinically, TDN is rarely performed in isolation and as such, clinicians should be aware of the possibility for post needling soreness and its potential effect on force production. Results of this analysis suggest that it may be beneficial to perform isolated gluteus medius contractions in an open chain position prior to any functional strengthening activities. This may reduce the effects that post-needling soreness may have on force production, thereby potentially reducing the risk for compensatory movement patterns during strengthening activities.
Study Limitations
The PI, who collected all of the data and applied the intervention to each of the study’s participants, was not blinded to which side received TDN and which side was the control. Even with standardized protocols, the risk of inadvertent bias during MVIC testing cannot be eliminated.
During the informed consent process, participants were instructed that the purpose of the study was to assess the effects of TDN on strength measurements of the gluteus medius, whether that be an increase or decrease in strength in an attempt to reduce the risk of performance bias. However, since participants were not blinded to which side received TDN and which side was the control side, performance bias cannot be completely ruled out.
Sham needles have been utilized in studies that have investigated the effects of dry needling to account for a potential placebo effect.27 When it comes to TDN studies, participants are able to feel the difference in needle depth penetration between the sham and TDN needles, as well as the elicitation of a LTR. Furthermore, if study participants have previously received TDN they may be able to realize the difference between the placebo and actual intervention. Future research on this topic could include other types of dry needling including superficial dry needling techniques, which may make it easier to include sham needles as a true placebo, while also reducing the potential for post needling soreness.58
While the side of dominance was recorded for each of this study’s participants, it was not considered during statistical analysis outside of descriptive statistics for demographic information of the sample. Future studies may consider if side of dominance has an effect on the number of MTrPs found in the muscle tissue as well as study outcomes.
This study only assessed the outcome measures immediately following the application of TDN. Future studies should assess the effects of TDN on muscle strength at different post-treatment time intervals. Furthermore, TDN’s effect on muscle force production or activity during functional movements should also be investigated as this may have a more direct clinical application to improving performance during activities of daily living.
CONCLUSION
Application of TDN to latent trigger points within the gluteus medius musculature was able to significantly increase gluteus muscle force production immediately following intervention while reducing the level of electromyographic muscle activation required during force production testing. These results suggest that latent trigger points may have a negative impact on gluteus medius muscle strength as well as the efficiency of contraction. Clinically, latent trigger may be considered as a potential source of impaired muscle function.
Clinical Trials Registration Number
ClinicalTrials.gov, ID NCT035802000
Conflicts of Interest
The authors report no conflicts of interest