





INTRODUCTION
Landing on a single leg is a common movement in sports such as basketball, volleyball, and soccer. When this movement is not adequately controlled by the neuromuscular system, non-contact anterior cruciate ligament (ACL) injury may occur.1,2 It is well established that female athletes are more likely to suffer non-contact ACL injuries than male counterparts participating in the same sports.3 Female athletes have also been shown to have an increased propensity to experience ACL injury on their non-dominant limb which was defined as the stance limb when kicking a ball.4,5 However, minimal differences in mechanical variables have been reported between dominant and non-dominant limbs during a cutting task in female soccer athletes.6 Thus, it is unclear whether the reported increase in injury rate between dominant and non-dominant limbs are linked to bilateral mechanical differences.
Mechanisms for non-contact ACL injury consist of dynamic joint angles that result in excessive tensile forces on the ligament. For example, excessive knee abduction, and internal rotation have been shown to increase ACL strain during cadaveric modeling.7 Video analysis of ACL injury incidents has identified combined knee abduction and internal rotation as a mechanism of injury.8 Investigators have also demonstrated an increased lateral pelvic tilt is related to increased knee abduction moments, which may increase the risk of non-contact ACL injury.1,9,10 Alternatively, studies using 3D modeling and magnetic resonance imaging suggest that the ACL is under greatest strain during knee extension during dynamic and static loading.11,12 In addition to the various mechanisms of ACL injury, researchers have also hypothesized that lower extremity kinematic differences (asymmetry) can increase the risk for injury due to an increased loading and reliance on one limb, combined with an inability to maintain stability on the other.13
The single leg drop-landing (SLD) task is often used to assess lower limb kinematic symmetry.14–16 Other tasks that are more functionally related to sport movements, including cutting maneuvers, single leg hop for distance, and single leg jumps, have also been used to analyze lower limb symmetry.17–20 However, these tasks may require greater coordination and training to achieve or perform within the limits of a study design.16 Thus, the relatively limited complexity of the SLD may make it advantageous for the analysis of intrinsic bilateral asymmetries across individuals with varied training backgrounds.
Previous studies that have used a SLD task to examine potential bilateral lower extremity asymmetries have reported mixed results. Recently, Wang and Fu demonstrated an increased total hip and knee range of motion in the sagittal plane in the dominant limb of female soccer players.21 Other researchers16 did not find bilateral kinematic hip and knee differences in recreationally active females. The differences between populations may explain the conflicting findings. However, another possible reason for the discrepancies between these studies is the classification of lower extremities by either dominant limb or non-dominant limb when performing a group analysis.
When using a group analysis for the examination of bilateral differences, problems may arise from the difficulty of classifying a dominant lower limb. While several studies have defined the dominant lower limb as the leg used to kick a ball,5,6,14–16 limb dominance is likely task specific.22 If limb dominance is task-specific, grouping participants’ limbs based on what would be an arbitrary question, may generate misleading results. These factors have led researchers to contend that single subject design data should be reported in addition to group analysis when making bilateral comparisons.23 Thus, reducing the potential for applicable findings to be masked by interindividual variability between dominant or non-dominant limbs.
Another potential reason for discrepancies between the aforementioned studies is the interpretation of variables at discrete time points which may lead to analysis of less than 5% of the data.24 Discrete analysis of biomechanical variables may not always be comparable across participants or within participants due to temporal variations in movement traces.18,25 These potential inconsistencies may limit the interpretation of a temporal component, and how kinematics temporally relate to other biomechanical factors within the same movement. Thus, a more robust method may be required when examining a movement related to ACL injury risk that does not have a clear mechanism and timing. A proposed solution to this problem is statistical parametric mapping (SPM) which can be used to statistically analyze the kinematic waveform of the complete task cycle.25
Bilateral asymmetries during a SLD have not been analyzed with a SPM analysis at the group or single subject level. Thus, the purpose of the present study was to examine the SLD kinematic waveforms of female recreational athletes for the pelvis, hip, and knee using SPM. By including a group analysis and single subject design, the current study sought to identify the potential of inter-participant variability to influence group bilateral asymmetries. It was hypothesized that bilateral differences of the waveforms at the single subject design level would occur but not at the group level due to inter-participant variability.
METHODS
Participants
Nine female participants who were free from lower limb surgery, disease, or current injury volunteered for this study. Participants had a mean [SD] age of 22.4 [3.5] years, height of 1.68 [0.57] m, mass of 61.0 [6.7] kg. All participants were defined as physically active and performed plyometric activities at least once per week. Physically active was defined as performing at least 30 minutes of low-intensity exercise five times per week, 20 minutes of high-intensity exercise three times per week, or participants who ran at least five miles per week. For descriptive purposes, all participants were asked which limb they preferred to kick a ball with. All reported that their right limb was their preferred kicking limb. Prior to participation, all participants signed an informed consent form approved by the University’s internal review board.
Instrumentation
Three-dimensional marker trajectories were collected with an eight-camera motion capture system (250 Hz; VICON, Oxford Metric Ltd., Oxford, UK). Participants were equipped with 73 retro-reflective markers (14mm) used to create a custom cluster-based model for the upper extremities, torso, pelvis, and lower extremities (Figure 1).

A force-platform (1000 Hz; ORG-6, AMTI Inc., Watertown, MA, USA) time synchronized with the motion capture system was used to collect ground reaction forces (GRFs).
Drop Landing Procedure
Prior to performing the SLD, participants performed a five-minute warm-up on a stationary bicycle. Participants were then asked to perform the SLD task from a 60 cm platform after completing two practice trials on each leg. The platform was positioned behind the force platform with a minimum distance that allowed participants to vertically land on the center of the force platform to minimize GRF in the anteroposterior direction. Participants were asked to place the limb they would land on off the step and then drop down onto the force plate with minimal assistance from their stance limb to drop off the box. No restrictions were placed on the positioning of the arms. Participants performed 10 successful trials on each leg with a maximum of 15 attempts. Participants were given as much time as they needed between trials and the starting limbs were counterbalanced to reduce the potential effect of fatigue. Trials were considered successful if the participant was able to drop off the box without lowering themselves with the stance leg and maintain balance upon landing as determined by the researcher. All participants wore their own activity shoes, which was done to remove any perturbation caused by novel footwear.
Data Analysis
Angular kinematics and center of mass were computed using a Cardan (X-Y-Z) rotation sequence with Visual 3D software (v6, C-Motion Inc., Germantown, MD, USA). Pelvis segment angles were calculated using a Z-Y-X sequence of rotations to be consistent with the conventional clinical understanding of pelvic tilt and pelvic drop. The pelvis was modeled as a using the anterior and posterior superior iliac spines and pelvis segment angles were calculated relative to the global coordinate system. Pelvic drop was defined as the angle in the frontal plane and pelvic tilt was defined as the segment’s rotation in the sagittal plane. Negative values in the frontal plane were represented as a contralateral pelvic drop and anterior pelvic tilt was represented by positive values. Marker trajectories were filtered using a fourth-order Butterworth filter at 8 Hz and kinetic data were filtered at 20 Hz respectively. Vertical GRF data was used to define initial contact (IC) at the beginning of the deceleration phase. The IC was defined as the moment when the vertical GRF threshold of 20 N was surpassed. To define the end of the deceleration phase, we used the minimum vertical height of the center of mass (minCOM).26 Joint (hip and knee) and segment (pelvis) temporal data were analyzed between IC and minCOM using MATLAB (MathWorks, Natick, MA, USA). Temporal data were interpolated to 101 data points (100% of cycle) for the SPM analysis.
Statistical parametric mapping
All SPM analyses were conducted in MATLAB using an open-source software package spm1D 0.4.27 Multiple paired t-tests (p < 0.05) were performed with Bonferroni corrections to compare the grouped kinematic data of lower extremity limbs for all participants at each percentage of the cycle. For group analysis the mean trajectories of each participant’s twenty trials (10 on each leg) were used. Additionally, paired t-tests were performed comparing the limbs for each individual participant that was calculated using 10 trials from each limb. The significance level for all statistical tests after the alpha corrections was (p = 0.006). The null hypothesis was rejected if the computed t-value exceeded the critical threshold. In SPM the t-value is calculated across the temporal region of interest (i.e., IC to minCOM). Whereas, the critical threshold is a product of random field theory that can be used to determine a threshold where equivalently smooth Gaussian random fields would cross at the specified alpha level when the null hypothesis is true.28
RESULTS
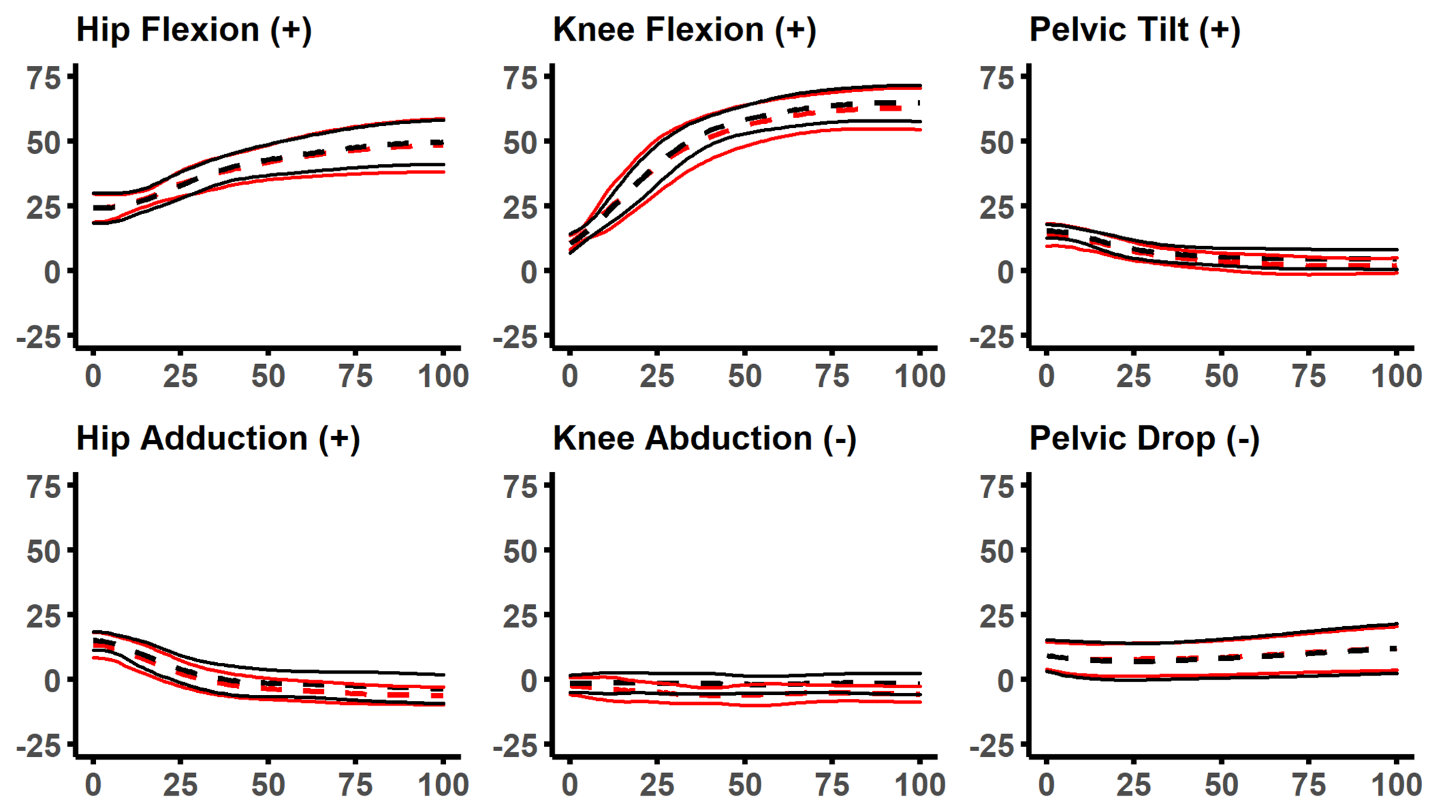
The group SPM analysis with paired t-tests did not reveal any significant differences between the dominant and non-dominant limbs for all kinematic variables (Figure 2).

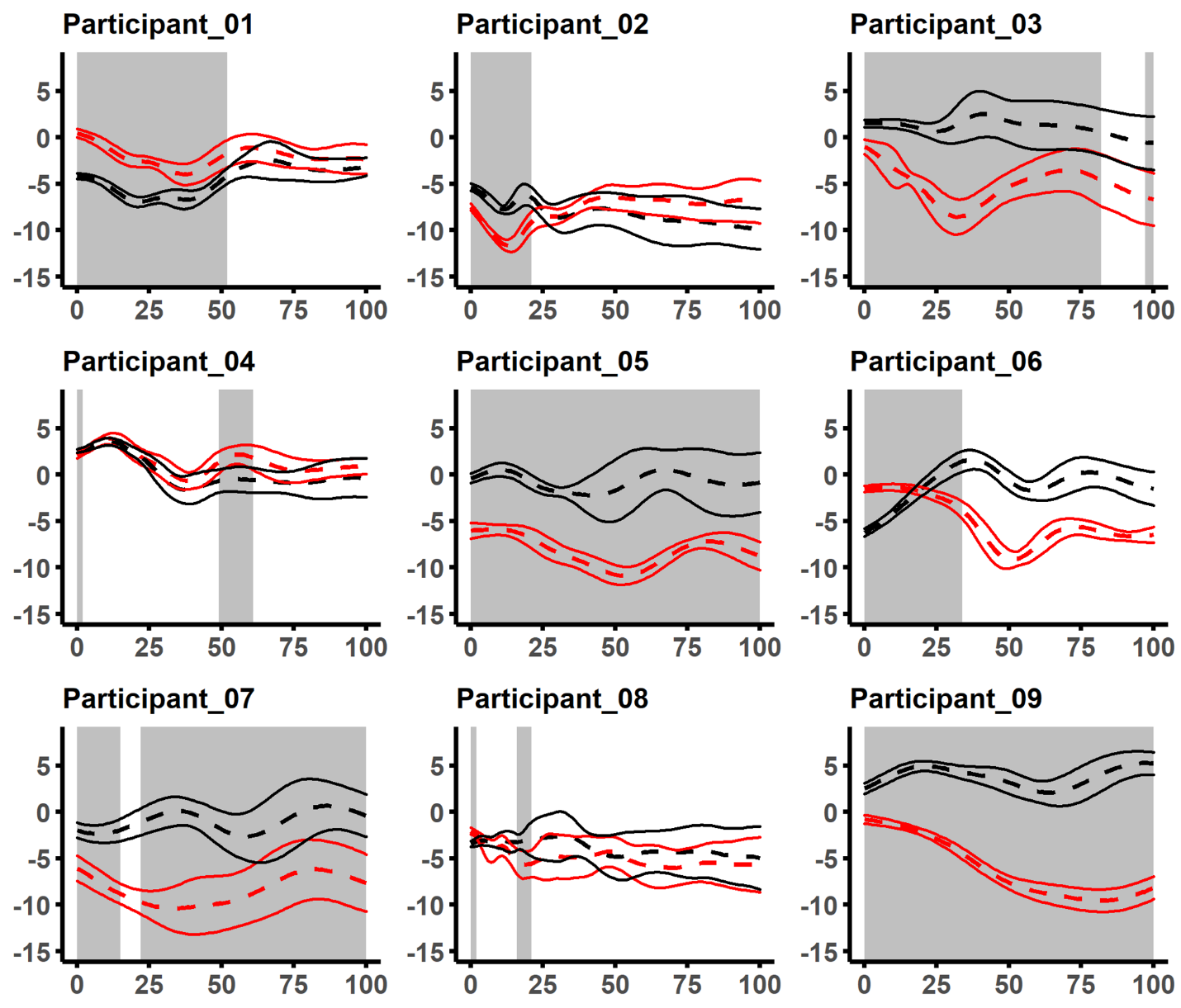
Individual SPM analysis with paired t-tests revealed significant kinematic differences between the right and left limbs for all participants. At the hip in the sagittal plane, seven participants had a significant difference between their two limbs. During the phase when the difference between lower limbs exceeded the critical threshold, four of those seven participants had a relative increase in hip flexion on the right limb (Figure 3).

Conversely, the remaining three with significant differences were shown to have increased hip flexion on their left limb. At the knee in the sagittal plane, seven participants had a significant relative difference between their two limbs (Figure 4).

Four of those participants increased knee flexion on the left limb and three increased knee flexion on the right limb. Anterior pelvic tilt was greater when landing on the left limb in five participants, and in three participants when landing on their right limb (Figure 5).

For frontal plane hip motion, six participants had increased hip adduction on the right limb and three participants had relatively increased adduction on the left limb (Figure 6).

At the knee, two participants had increased knee abduction on the right limb, 4 had relative increases on the left limb, and participants six and eight had relative differences between limbs in both directions (Figure 7).

Significant differences for pelvic drop occurred in eight of the nine participants (Figure 8).

Six of those participants had a relative decrease in pelvic drop when landing on their right limb.
DISCUSSION
The aim of this study was to examine physically active females for potential bilateral differences in pelvis, hip, and knee kinematics during a SLD task. A group analysis (comparison of mean data between right and left limbs) and a single subject design was used to ascertain the findings of potential bilateral differences among the population studied. The findings indicated that there were no significant differences for kinematic variables between the right and left limbs when analyzed at a group level. However, this was not indicative that bilateral differences were not prevalent among the study’s population. For instance, each of the participants demonstrated at least two asymmetries out of the six variables in question and six out of the nine participants had bilateral differences for all kinematic time-series. Thus, the hypothesis that bilateral differences would be observed at the single subject design level, but not at the group level was accepted. The consequence of group analysis concealing individual differences is not novel to the current study.29–31
The data were grouped by right and left limbs because there is currently not a clear metric for determining limb dominance during a SLD task. However, the selection of comparing right and left limbs was not an adequate method for homogenizing participant data to describe the observed differences between limbs. Therefore, the approach of including a single subject design allowed us to look at bilateral differences without defining the criteria of which leg was dominant during the task. It should be noted that all participants reported that they preferred kicking a ball with their right limb. Thus, grouping limbs by this metric would not have affected the outcome of the data.
The absence of significant group findings may be explained by not all participants displaying similar movement patterns with their right or left limb. For example, participants (4, 5, 9) had a significant relative increase for hip flexion angles on their right limbs when compared to their left (Figure 3). Conversely, participants (1, 2, 6, 8) demonstrated greater hip flexion on their left limb (Figure 3). Similar participant variability was also observed in the other variables of interest. Thus, it appears that in this sample population of uninjured participants, the heterogeneous movement patterns influenced the findings at a group level and provided support for the use of single subject analysis.
The current study’s group findings in recreational female athletes are similar with those of Wang and Fu21 who found no bilateral differences in female soccer players at IC. However, the researchers15 did not include a single subject design which may have limited their interpretation of their results. For instance, when considering this study, four of the participants (1, 4, 6, 9) had a significant difference for hip and knee flexion at IC (Figure 3, 4). Interestingly, for hip frontal plane motion all but one of the participants (8) demonstrated a significant difference at IC (Figure 6). At the knee in the frontal plane, all but two of the participants (4, 8) had statistically similar waveforms at IC (Figure 7). Another difference between the two studies methods is the fact that the female soccer players dropped from a box 20cm shorter than what was used for the current study’s participants (60cm).
It has been shown that increasing the height of the SLD task may result in greater bilateral kinematic differences.16 In a study where participants landed from the same height for the SLD task as the current study, the researchers16 also reported that no bilateral differences were observed for hip and knee flexion between the limbs of recreationally active females. However, the researchers16 analyzed the kinematic data at the moment of peak vertical GRF because it was thought to be related to the timing of injury. As discrete time points were not considered in the current analysis (other than to determine the beginning and end of the movement) it is difficult to draw comparisons with their kinematic data. The discrepancies between cadaveric7,32 and model simulated ACL strain11,12 is conflicting for researchers looking to identify the optimal time or joint angle for assessing risky lower extremity movement patterns. Research from cadaveric modeling has been used to suggest that peak ACL strain occurs simultaneously with peak knee abduction angles.33,34 Thus, there is a potential advantage of using a wave form analysis technique as it limits the bias of researchers when selecting discrete time points for analysis.
To the best of the authors’ knowledge, this is the first study to include pelvic kinematics with bilateral comparison during a SLD task in females. Bilateral pelvic imbalances may be relevant to injury prevention as increased pelvic kinematics have been shown to result in amplified torque at the knee in the frontal plane during a SLD jump.35 Only three of the participants (Figure 8) displayed mean pelvic drop angles below 0° (neutral). However, these findings may be more indicative of the SLD methods than the ability of the participants to stabilize their pelvis in the frontal plane. For example, each of the participants landed with a negative pelvic drop (i.e., their hip on their landing limb was lower). This is likely due to asking them to step off the box with the same limb that they landed on. If the participants had landed in a more neutral position, greater pelvic drop angles may have been observed. Nonetheless, all but one of the participants (8) demonstrated a bilateral difference. Interestingly, six of the participants (1, 2, 3, 5, 7, 9) who landed in a more neutral pelvic position (closer to 0°) had increased knee abduction angles on the same limb (Figure 7, 8). This suggests that pelvic and knee kinematics may be linked during a SLD task. However, a causative relationship cannot be established with the current evidence.
When examining anterior pelvic tilt, most of the participants (3-9) demonstrated a significant bilateral difference. Although the purpose of the current study was not to describe the ideal anterior pelvic tilt during the movement task, it may be that not all participants with bilateral differences possess inadequate pelvic control. For instance, participants 7, 8, and 9 either maintained a relatively neutral pelvis, or decreased the amount of pelvic tilt throughout the motion (Figure 5). In contrast, participants 1 and 2 did not present with bilateral differences but increased their degree of anterior pelvic tilt from initial contact to the end of the movement.
Although the results of this single subject analysis indicated that each of the participants had kinematic imbalances during the SLD task, it is still unclear whether these asymmetries were suggestive of poor movement patterns (on one or both limbs) that may facilitate an increased risk of injury. It may be that the observed bilateral differences were simply a result of performance variability between the two limbs. In short, performance variability is a natural biologic phenomenon that adapts for desired outcomes based on force distribution mechanisms, development or skill level, and environmental factors.23 Inter-individual variability has been shown to occur in professional athletes during basketball shooting and elite javelin throwers,30 as well as in recreational athletes while running and performing a SLD.23,30 The participants’ bilateral kinematic differences in the current study may have been compensations that occurred due to muscular strength imbalances, prior training, or possibly structural/anatomical asymmetries. Thus, the observed imbalances may have been necessary to complete the task. Further research is needed to examine the circumstances in which movement compensations and bilateral differences are beneficial or detrimental.
This study has several limitations. First, the current study only collected data on a small sample of physically active female participants. Group findings may have been apparent if participants had more homogeneous training backgrounds. A larger sample size may also have provided a greater probability of observing differences at the group level. Second, participants were only stratified based on their right or left limb. Future research might examine the potential for task specific methods to dichotomize limbs. For example, participants may self-identify their preferred landing limb. Lastly, due to the method participants dropped off the box (i.e., stepping), there may have been differences in the distance they fell onto the force plate, either between legs, or participants.
CONCLUSION
At the single subject analysis level, participants were asymmetrical regarding their kinematic time-series. However, these differences were not observed in any of the waveforms for the group analysis. The authors recommend that until an accepted method for dichotomizing right and left limbs for bilateral comparisons is accepted, single subject design should be included with any group analysis where bilateral differences are examined.
Disclosures
This study was approved by the University of Idaho Institutional Review Board, irb@uidaho.edu
The authors did not have any financial or personal relationships with people or organizations that may have inappropriately influenced or biased their work.