INTRODUCTION
Anterior cruciate ligament (ACL) tears are common among high school age athletes who participate in sports that involve frequent single-leg landing, cutting, and pivoting.1,2 Athletes who have sustained an ACL tear typically undergo ACL reconstruction and then complete extensive post-operative rehabilitation.3 Approximately one in five of these athletes will go on to sustain a second ACL injury shortly after returning to sport.4 This alarmingly high injury rate highlights the urgent need to examine factors that may influence an athlete’s ability to safely return to sport following ACL reconstruction.
Athletes who have undergone ACL reconstruction often demonstrate deficits in postural stability and dynamic balance for their involved limb (vs. their uninvolved limb), even after completing post-operative rehabilitation.5–7 This is concerning since deficits in postural stability and dynamic balance are associated with an increased risk for ACL injury/re-injury.8,9 Athletes who have undergone ACL reconstruction also tend to exhibit persistent (12+ months post-surgery) deficits in single leg hop performance for their involved limb,10–12 which is likely due, at least in part, to limitations in lower extremity strength and power generation.11 These types of persistent neuromuscular deficits may contribute to re-injury and/or limit an athlete’s ability to return to their prior level of sport performance.
Factors such as quadriceps weakness13,14 and kinesiophobia15,16 have been studied extensively and appear to contribute to the persistent deficits in dynamic balance and hop performance commonly exhibited by athletes following ACL reconstruction. However, one potential factor that has not been thoroughly examined is an athlete’s meniscal injury history. At this time, only one previously published study has compared dynamic balance for athletes with and without a history of concomitant meniscal injury13 and no studies have examined how meniscal injury status affects inter-limb symmetry in hop performance. It is important to further examine the influence of meniscal injury history since more than half of all ACL tears are accompanied by a meniscus tear,17–19 with 56% of tears involving the lateral meniscus and 44% of tears involving the medial meniscus.17 It is also important to examine whether neuromuscular performance is affected by how an athlete’s meniscal tear was managed. While surgeons typically attempt to repair the meniscus if possible, in some cases they must debride the injured part of the meniscus (partial meniscectomy). This could potentially negatively impact knee control, since the menisci serve as a source of mechanical stability for the knee.20–22
Therefore, the purpose of this study was to compare inter-limb asymmetry in dynamic balance and hop performance for athletes with and without a history of concomitant meniscal injury. It was hypothesized that the degree of interlimb asymmetry in dynamic balance and hop performance would be similar for athletes with isolated ACL tears, compared to athletes with concomitant meniscal injuries, regardless of whether they had undergone meniscal repair or partial meniscectomy.
MATERIALS AND METHODS
Participants
Clinical outcomes for 34 adolescent athletes were analyzed as part of this cross-sectional study; 19 (9 males, 10 females) of these athletes had sustained an isolated ACL tear, while 15 (8 males, 7 females) had sustained an ACL tear along with a partial meniscus tear. All athletes were competing at the high school level at the time of injury and were between 14-19 years of age at the time of testing. This age range aligns with the World Health Organization’s definition of adolescence.23 To be included in this study, athletes needed to have undergone successful primary unilateral ACL reconstruction (either bone-patellar tendon-bone autograft or hamstring tendon autograft), completed conventional post-operative rehabilitation, participated in facility-standard return to sport testing (which included testing of dynamic balance and hop performance), and expressed an intention to return to competitive sports. Data were excluded for athletes with a history of major injury or surgery for their uninvolved limb, a history of major injury or surgery for their involved limb (aside from their ACL injury/reconstruction), or a concomitant ligament injury (e.g. medial collateral ligament tear). ACL reconstruction surgeries were performed by one of a group of five orthopedic surgeons. All athletes had completed post-operative rehabilitation (see Rehabilitation Protocol sub-section for details) with the same physical therapist who is a board-certified sports clinical specialist through the American Board of Physical Therapy Specialists. The athletes had resumed high-level dynamic activities, such as landing and jumping, but had not been cleared to return to sport at the time of testing. At the time of testing, none of the athletes had notable limitations in knee range of motion (beyond what could be attributed to measurement error) or visible signs of effusion for their involved knee. The athletes who had sustained a meniscus injury had either undergone a meniscal repair (n = 9) or a partial meniscectomy (n = 6). Study data were obtained through retrospective chart review. This study protocol was approved by the Institutional Review Board at Lutheran Hospital (Fort Wayne, IN, USA).
Rehabilitation Protocol
The athletes’ rehabilitation generally progressed through four phases (a copy of the protocol is included as supplementary material). Phase 1 focused on controlling swelling/effusion, increasing knee motion, maintaining patellar mobility, facilitating quadriceps activation and strength, and initiating and progressing weight-bearing. Phase 2 focused on regaining full knee range of motion, improving quadriceps and hamstring strength, normalizing walking gait, promoting knee control during functional tasks, general lower body strengthening, and aerobic conditioning. Phase 3 focused on more advanced strengthening and conditioning, initiation and progression of running, jumping, and cutting, and sport-related training. Phase 4 focused on more advanced strengthening and training to promote sport-specific skills (e.g. sprinting, agility drills). Rehabilitation followed this general protocol for all athletes; however, athletes progressed through the stages at different rates, depending on a variety of factors (e.g. surgical factors, rate of recovery). Return-to-sport testing was conducted once athletes exhibited full knee motion (based on goniometric measurements), minimal pain/effusion, symmetrical strength for their involved limb (within 90% of the uninvolved limb, based on standardized testing with a handheld dynamometer), and no major movement faults (e.g. quadriceps avoidance, excessive knee valgus) during dynamic activities such as landing, jumping, and cutting (based on visual observation by the therapist). At the time of testing all athletes had successfully “completed” rehabilitation from the standpoint of they had met the criteria for formal return-to-sport testing.
Study procedures
The data analyzed as part of this study were recorded at the time of the athletes’ return-to-sport testing session (within a range of 5-11 months after surgery). To promote consistency, testing was standardized and administered by the same physical therapist who has extensive experience in administering the tests used in this study. Subjects wore their own athletic shoes during testing.13
Hop testing
All athletes completed the single hop test and triple hop test, which are both common performance-based outcome measures used to assess knee-related function and lower extremity strength/power following ACL reconstruction.24,25 For each hop test, the athlete was given a demonstration, performed a practice trial with each limb, and then completed two successful trials per limb, with the uninvolved limb tested first.24,25 Successful trials were defined as trials where the athlete was able to maintain single-limb stance for at least two seconds upon the final landing.25 Unsuccessful trials, such as when an athlete was unable to maintain single-limb stance for at least two seconds, were repeated (up to two repeat trials per limb). The average of the two successful trials was recorded as the outcome of interest. No restrictions were placed on arm movement during hop testing.25 Hop testing was performed in a fieldhouse with artificial field turf.
For the single hop test, the athletes initiated the test in single-limb stance (test limb) with their toes behind a marked line. They then hopped forward for maximal distance, landing on their test limb. Hop distances were measured in centimeters using a tape measure affixed to the turf. Measurements were taken at the point of the heel of the athlete’s shoe for the test limb. The triple hop test was completed in the same manner, except the athlete completed three consecutive maximal hops with their test limb.
Performance on both the single hop test and triple hop test have been shown to demonstrate excellent test-retest reliability, are sensitive to changes for the involved limb over the course of rehabilitation, and correlate with perceived lower extremity function in athletes with a history of ACL reconstruction.25,26
Dynamic balance testing
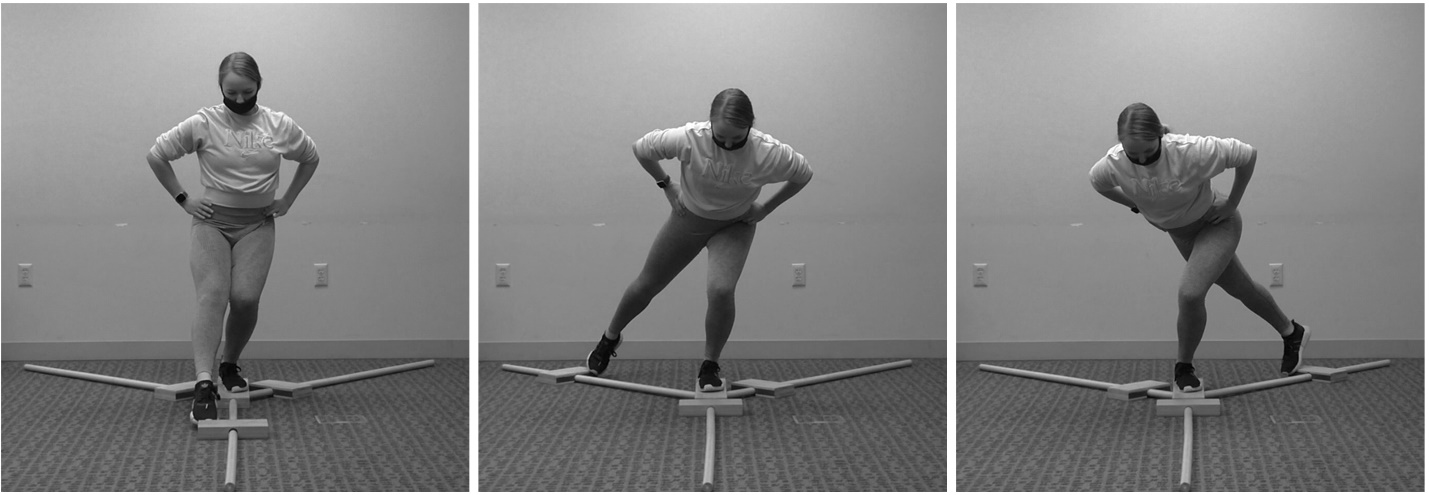
Similar to the hop tests, the athletes completed the Lower Quarter Y Balance Test (also referred to as the modified Star Excursion Balance Test) with both their involved and uninvolved limbs. A Y-Balance Test kit was used to record test performance (Functional Movement System; Danville, VA, USA). The Y-Balance Test is a commonly used clinical test to assess single leg dynamic balance. As part of the test, athletes must maintain their balance on a single limb (test limb) while reaching as far as possible in the anterior, posteromedial, and posterolateral directions with their contralateral limb, while a sliding indicator is used to mark their reach distance (Figure 1). Athletes completed three trials per limb in each direction. An examiner recorded the single farthest distance reached (centimeters) for each direction. As recommended, the athletes were given a demonstration of the test and completed practice trials in each direction prior to formal testing.27 Athletes completed three trials with their right limb and then three trials with their left limb in the anterior direction.27 The same testing procedures were then completed in the posteromedial and posterolateral directions. As recommended,28 athletes where required to maintain their hands on their hips when completing the Y-Balance Test in order to limit their ability to use their upper extremities to assist in maintaining stability.29,30 This allows for a more direct assessment of lower body neuromuscular control, since it limits an athlete’s ability to stabilize themselves with their upper extremities.28 Trials were considered invalid if the athlete failed to maintain single-leg stance throughout the trial, failed to maintain foot contact with the indicator when reaching, used the indicator for support, or removed their hands from their hips during a trial.13,27
__poste.jpeg)
The Y-Balance Test has been shown to demonstrate excellent intrarater and interrater reliability.31 In addition, relatively poor Y-Balance Test performance has been found to be associated with an increased risk of sport-related non-contact lower extremity injury, including ACL tears.9,31
Statistical analysis
The dependent variables of interest were the reach distances for the Y-Balance Test (anterior, posteromedial, and posterolateral directions) and the hop distances for the single hop test and triple hop test. For each variable, a two-way, mixed-model analysis of variance with a between-subjects factor of group (isolated ACL tear, meniscal repair, partial meniscectomy) and a within-subjects factor of limb (involved, uninvolved) was conducted. An alpha level of 0.05 was used for each test of statistical significance. In addition, 95% confidence intervals (CI95%) were generated to supplement the results of the null hypothesis significance tests.
A limb symmetry index (LSI) was also generated for each variable by dividing the distance for the involved limb by the distance for the uninvolved limb and then multiplying by 100 to express as a percentage.6,24,25 An LSI equal to 100% reflects perfect inter-limb symmetry, an LSI less than 100% reflects poorer performance for the involved limb, and an LSI greater than 100% reflects poorer performance for the uninvolved limb. SPSS software was used for statistical analysis (Version 28; IBM Corp., Armonk, New York, USA).
RESULTS
Table 1 describes the characteristics of the athletes whose data were analyzed as part of this study.
There was not a group-by-limb interaction effect for the anterior [F (2, 31) = 0.26; p = 0.77], posteromedial [F (2, 31) = 0.86; p = 0.43], or posterolateral [F (2, 31) = 0.41; p = 0.67] Y-Balance Test reach distances, or the single hop test [F (2, 31) = 0.04; p = 0.96] or triple hop test distances [F (2, 31) = 0.03; p = 0.97], which indicates that the groups exhibited similar degrees of inter-limb asymmetry in dynamic balance and hop test performance.
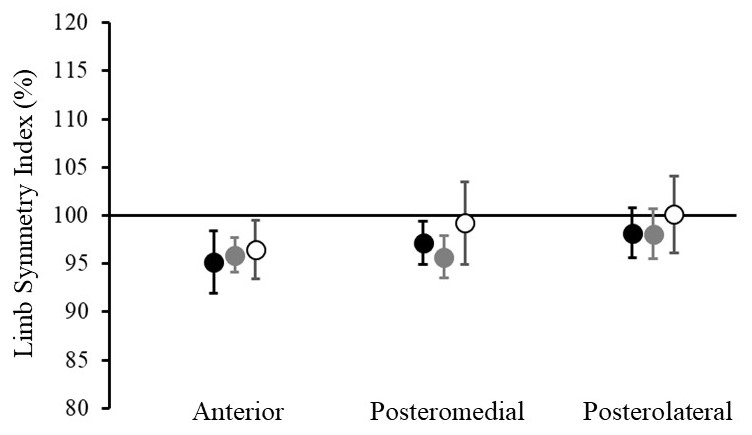
There was a main effect of limb for the anterior [F (1, 31) = 16.52; p < 0.001] and posteromedial [F (1, 31) = 9.76; p = 0.004] Y-Balance Test reach distances; however, there was not a main effect of limb for the posterolateral direction [F (1, 31) = 1.56; p = 0.22] (Figure 2). On average, Y-Balance Test reach distances were 2.7 cm less in the anterior direction [CI95% = (-3.8 cm, -1.6 cm)] and 3.3 cm less in the posteromedial direction [CI95% = (-5.1 cm, -1.5 cm)] for the involved limb, compared to the uninvolved limb.
_limb_symmetry_index_values_based_on_the_y-balance_test_di.jpeg)
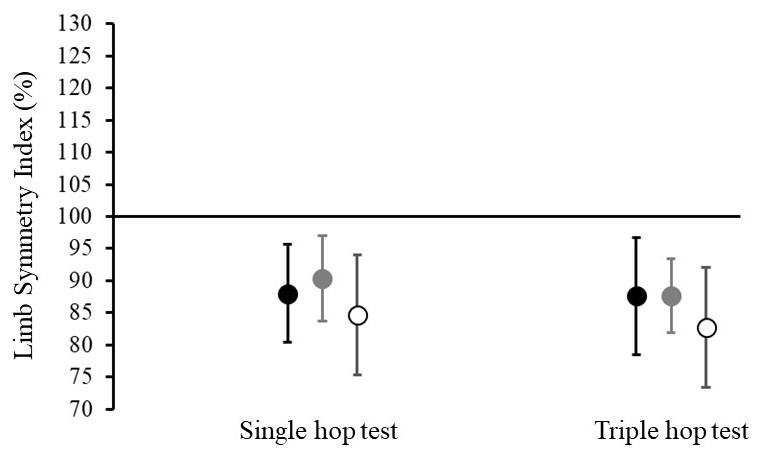
There was also a main effect of limb for the single hop test [F (1, 31) = 15.55; p < 0.001] and triple hop test [F (1, 31) = 20.92; p < 0.001] distances (Figure 3). Single hop test distances were 19.2 cm less for the involved limb [CI95% = (-27.5 cm, -10.8 cm)] and triple hop test distances were 57.5 cm less for the involved limb [CI95% = (-80.1 cm, -34.9 cm)], compared to the uninvolved limb.
_limb_symmetry_index_values_based_on_the_hop_test_distance.jpeg)
There was not a main effect of group for any of the variables of interest (p ≥ 0.12).
DISCUSSION
The purpose of this study was to compare inter-limb asymmetry in dynamic balance and hop performance for athletes with and without a history of concomitant meniscal injury. As hypothesized, the degree of interlimb asymmetry in dynamic balance and hop performance was similar among athletes with isolated ACL tears and athletes with concomitant meniscal injuries who had undergone meniscal repair or partial meniscectomy. Each group of athletes (isolated ACL tear, meniscal repair, partial meniscectomy) exhibited deficits in dynamic balance and hop performance for their involved limb, vs. their uninvolved limb (main effect of limb). In general, it appears that deficits in dynamic balance and hop performance following ACL reconstruction are not dependent on meniscal injury history.
A previous study by Clagg et al.13 also compared Y-Balance Test performance at the time of return to sport (average of 6.7 months after ACL reconstruction) for athletes with isolated ACL tears vs. those with concomitant meniscal injuries. Although the investigators did not examine inter-limb symmetry, their results were generally consistent with those of the current study, as they found no significant differences in involved-limb anterior, posteromedial, or posterolateral Y-Balance Test reach distances for athletes with isolated ACL tears vs. those with concomitant meniscal injuries. Considering the results reported by Clagg et al.,13 as well as those of the current study, it does not appear that deficits in dynamic balance differ for athletes with and without a history of concomitant meniscal injury. While Clagg et al.13 reported the average single hop test and triple hop test distances for their entire cohort of athletes, they did not compare hop performance based on meniscal injury history. They also did not differentiate between athletes who had undergone meniscal repairs vs. those who had undergone partial meniscectomies, as they grouped these athletes together in their analysis.
The results of this study suggest that athletes who have undergone ACL reconstruction exhibit deficits in dynamic balance at the time of return-to-sport testing, regardless of their meniscal injury history. In addition to their role in distributing axial joint loads, the menisci provide passive mechanical stability to the knee, contributing secondary restraint to tibial translations both anteriorly and posteriorly.20–22 The lack of an association between meniscal injury history and dynamic balance impairments in this study suggests these deficits may be related more to general neuromuscular factors than residual mechanical insufficiency of the involved limb. It has long been known that detriments to neuromuscular performance and limb asymmetries persist for years after ACL reconstruction and contribute to risk of future injury.11,32 However, the addition of rehabilitation techniques targeting these neuromuscular factors, such as perturbation training, has not resulted in consistent/significant improvements in functional outcomes or return to sport success rates.33 While a longer course of rehabilitation may be effective in mitigating injury risk and improving achievement of evidence-based return to sport criteria,34 an extended return-to-sport timeline may not be a satisfactory solution to many athletes. Thus, further research into emerging/novel surgical and rehabilitation techniques that specifically preserve or enhance neuromuscular function is needed. For example, transcranial direct current stimulation has the potential to impact corticospinal activity and may provide a means to maintain or improve neuromuscular function over the course of recovery after injury or surgical intervention.35 Additionally, surgical repair techniques that seek to preserve native ACL tissue, and potentially the neural elements of the ligament, may allow for greater natural restoration of neuromuscular function. Early studies of techniques such as the bridge-enhanced ACL reconstruction36 or other similar approaches have shown promise in the short term.37
While these techniques continue to develop, it is important to recognize there are long-standing treatment approaches with strong evidence that could be examined within a broader neuromuscular context. For instance, electrical stimulation is strongly recommended to enhance quadriceps strength in the latest clinical practice guidelines from the Orthopedic Section of the American Physical Therapy Association.38 However, studies of patients with neurologic disorders have demonstrated the value of functional electrical stimulation to enhance the neural representation of a limb within the central nervous system.39 Given that similar neurophysiologic and neurocognitive deficits have been demonstrated in individuals with ACL injury,40 use of electrical stimulation, in combination with more conventional rehabilitation components (e.g. targeted strengthening, active isometric muscle contraction), should be considered as a standard of care for more than restoration of simple muscular strength. In addition to augmented sensorimotor stimulation, the environmental context and cognitive-attentional demands of functional and sport-specific tasks should be considered in the rehabilitation plan. A graded exposure approach to the neurophysiologic and neurocognitive demands of patients’ activities may prove to be the most salient, cost-effective means to restoration of multi-system neuromuscular function.41
As with any study, it is important to consider the limitations of this work. First, it should be noted that the current study did not consider the extent or location of meniscal injury. This was also a limitation noted by Clagg et al.13 Future studies should examine how the nature/extent of meniscal injury affects neuromuscular performance. In addition, the effect of graft type was not examined as part of this study. Previous studies have compared neuromuscular performance among athletes who received different types of grafts6,13; however, the findings from these studies have been somewhat inconsistent. Also, it is important to note that clinical measures of dynamic balance and hop distance may not be sensitive to subtle differences in postural stability and movement performance. Future studies should consider applying more advanced instrumentation to identify more subtle differences in postural stability and movement control/performance. The relatively low number of athletes (n = 6) who underwent partial meniscectomy should also be considered as a limitation. Although not necessarily surprising, since surgeons typically aim to repair the meniscus when possible, the low number of athletes in this group may have limited our ability to detect subtle between-group differences in dynamic balance and/or hop performance.
Finally, it is worth noting the variability in when athletes were tested (ranging from 5-11 months post-surgery). Dynamic balance and hop test data were recorded at the point of return-to-sport testing, which is typical for studies of this nature.13 Since athlete’s progress through rehabilitation at different rates, this resulted in significant variability in the time from surgery to return-to-sport testing. The reason for comparing performance at the point of return-to-sport testing was to ensure that athletes were at a similar stage of recovery, even though they were not necessarily at the same time post-surgery. An alternative would have been to compare performance at a consistent time point (e.g. five months post-surgery); however, this would be problematic since athletes would be at different phases in their rehabilitation (e.g. some would be preparing to return-to-sport, while others would be just beginning to initiate landing/jumping tasks). Regardless, it is interesting to note the variability among athletes with respect to their return-to-sport timeline.
CONCLUSION
The results of this study indicate that adolescent athletes who have undergone ACL reconstruction exhibit deficits in dynamic balance and hop performance for their involved limb, even after completing post-operative rehabilitation. The results of this study also suggest that the magnitude of the inter-limb asymmetries in dynamic balance and hop performance are not dependent on meniscal injury history.
Disclosures
The authors have no conflicts of interest to report.
ACKNOWLEDGEMENTS
The authors would like to thank their partners at Lutheran Hospital and Optimum Performance Therapy for supporting this work.