INTRODUCTION
Hamstring strain injuries are among the most prevalent injuries sustained by basketball athletes.1 Previous epidemiological studies show the most common type of injury sustained by professional basketball athletes is a strain, with the hamstring muscle group being the most frequently strained muscle.1 An evaluation of injuries of the National Basketball Association showed strains comprised up to 57% of reported injuries.1 Of these strain injuries, 23% related to the hamstring muscle group. Universally, hamstring injuries are one of the most prevalent non-contact injuries in sports with approximately 96% of hamstring injuries occurring in non-contact situations.2,3 Although hamstring injuries are common, they can result in a substantial loss of playing time and an increased re-injury rate.2 The average number of days missed for basketball players who sustained a strain was 7.4 days, with nearly one-third of hamstring strains recurring within the first year of returning to play1,4 High rates of re-injury (12-14% within two years)5–7 cause more concern for athletes as re-injuries present with worsening severity and more lost play time upon re-injury.2 Previous authors have shown a near doubling of play time lost after hamstring re-injury.8
Many variables may play a role in an athlete’s susceptibility to initial hamstring injury and re-injury. Previous literature has postulated a relationship between greater hamstring stiffness and a higher risk of sustaining a hamstring injury.9 More recent literature has established a connection between increased hamstring stiffness and injury with male sex and past hamstring strain history.10,11 Male athletes routinely exhibit greater hamstring stiffness overall when compared to their female counterparts.10 Hamstring stiffness measurements (kPa) in male athletes are nearly double that of females on both the athlete’s dominant and non-dominant leg.10 Increased hamstring stiffness is a risk factor in male athletes as it associates with higher hamstring injury rates and a greater proportion of recurrent hamstring injuries.7 Compared to female athletes, male athletes participating in intercollegiate soccer are 64% more likely to sustain a hamstring injury and are nearly twice as susceptible to hamstring re-injury.4,12 In addition, initial hamstring injury can alter the length-tension relationship of the hamstring muscle group, which increases hamstring stiffness.9 On average, athletes with hamstring injury exhibit 11% higher hamstring stiffness than uninjured counterparts. This mechanical change places greater tension on the hamstring muscle group and may increase the re-injury rate after initial hamstring injury.9 Additionally, hamstring muscles in a lengthened state exhibit reduced strength and returning to sport without engaging eccentric strengthening in a lengthened muscle state predisposes secondary injury.13 In correlation with this increased stiffness, athletes with previous hamstring injury are also two to three times more likely to encounter a future hamstring strain than non-injured counterparts.8,14 However, increased hamstring stiffness is not universally observed after injury.15 Apart from associating with injury, muscle stiffness is also modifiable as dynamic stretching, which is known to decrease soft tissue injuries, has also been shown to decrease hamstring stiffness.16
Despite this data, findings that correlate injury prevention with hamstring stiffness based on sex are not unilateral. Female college basketball athletes suffer hamstring strains at higher rate than their male counterparts7 and, as noted, demonstrate decreased hamstring stiffness compared to their male counterparts. Decreases in passive stiffness are unfavorably associated with peak knee flexion torque generation,17 and knee flexion torque is subsequently associated with injury prevention.17 Indeed, greater hamstring stiffness has been associated with reduced knee ligament loading and reduced ligament injury risk18,19 Further, patients experiencing back pain exhibit reduced hamstring stiffness compared to matched controls.20 Accordingly, insufficient muscle stiffness can affect the stability of the surrounding joints. Thus, there is meritorious data to support injury prevention through both increased and decreased hamstring stiffness, but excessive hamstring stiffness is directly related to increased risk of injury to the muscle itself.
In addition to sex differences and hamstring injury history, increasing age and competition level correlate with increased hamstring injury incidence.9 Previous authors have found that in both football and soccer, surpassing 23 years of age was associated with a higher risk of hamstring injury in athletes compared to their younger counterparts.3,21 An estimated 1.78 increase in risk of hamstring injury is associated with every year increase in age after an athlete turns 23.22 The variation in hamstring injury rate by age is associated with an overall decrease in hamstring strength as individuals age resulting in a muscle imbalance between the quadriceps and hamstring muscle groups, ultimately leading to an increased risk of hamstring injury.6,23 Recently Alfuraih et al. showed decreasing hamstring shear-wave elastography (SWE) stiffness associated with aging in which elderly participants (77-94 years) had on average 16.5% lower hamstring stiffness compared to their young counterparts (20-35 years).24 Changes in SWE stiffness correlate with muscle weakness associated with aging.23,24 The epidemiology of collegiate injuries versus high school injuries shows a more drastic increase in injury rate than those associated with age.25 The rate of overuse injury in college athletes is 3.28 times higher than in high school athletes.25 In both high school and college athletes, muscle strain is the most common injury.25
The mechanisms of hamstring injury are essential starting points for developing injury prevention programs. Preventative biomechanical techniques are an increasingly popular means of decreasing the risk and incidence of musculoskeletal injuries.26 Targeted neuromuscular training (TNMT) is a preventative biomechanical technique that consists of exercises designed to activate deficient muscle groups and encourage muscle co-activation that may be related to injury through movements that mimic those experienced during sport.26,27 Monajati el al. demonstrated that hamstring-based neuromuscular training increases hamstring strength and flexibility over time.28 As a prevention technique, TNMT addresses muscle stiffness and hamstring to quadriceps strength ratio (H:Q) as plausible risk factors for hamstring injury.28 This biomechanical technique accomplishes neuromodulation using motor learning principles to focus on optimal control of 3D body positions and movement symmetry.27 Ultimately, re-establishing connections between nerves and muscles after injury leads to a reduced risk of re-injury.27 Accordingly, extrapolation of TNMT to non-contact hamstring injuries may prove efficacious in decreasing hamstring strain prevalence and severity by altering baseline biomechanics.
Commonly, hamstring injury is evaluated and diagnosed via dynamic ultrasonography. Classic clinical implementation of ultrasonography, relative to musculoskeletal injury, provides high-resolution imaging of fluid collection around an injured muscle or tendon.11 These images are highly accurate in the determination of the location and extent of a hamstring injury. Beyond diagnosis and localization, these images have limited use for risk prevention as they fail to provide feedback on mechanical properties or quality of individual muscle.10 Shear wave elastography (SWE) is a relatively new ultrasound technology that can provide a non-invasive evaluation of soft tissue elasticity.29 Accordingly, interest in musculoskeletal applications for SWE has grown in the past several years.10,11,29 Ultrasound SWE uses variation in wave propagation to create images that provide an objective measure of tissue elasticity with anatomic specificity.29 Past researchers have used SWE to evaluate and provide an initial characterization pathologic conditions and injuries of the musculoskeletal system, including, but not limited to, the hamstring muscle group, neck/back muscles, the Achilles’ tendon, and the anterior cruciate ligament.10,11,24,29,30 SWE can be used to assess hamstring stiffness at the time of injury, pre, and post-injury providing feedback on injury risk associated with increased stiffness and decreased hamstring stiffness post- injury prevention facilitation.27,28 Sex differences in SWE for adolescent basketball athletes have previously been explored,10 but further study into the relationship between hamstring stiffness and injury rate is necessary to determine whether hamstring stiffness is a primary causal factor for increased injury rate by age and competition level. It is known that increased stiffness at the muscle-tendon unit correlates with greater work absorption, muscle force, and power during countermovement jumps.31,32 As muscle stretch is necessary to induce injury and muscle failure occurs at forces greater than maximal isometric contractions,33 it remains that excessive passive muscle stiffness may predispose muscle tissue to injury. Subsequently, viscoelastic muscle stiffness can be reduced through passive and active stretching which increases both the force and energy absorption till failure.33 Additional investigation may also elucidate whether alteration of hamstring stiffness is a primary mechanism for injury prevention techniques such as TNMT. Finally, strong correlation between hamstring stiffness and injury may provide data that suggests that SWE is an optimal tool for determining injury risk and intervention efficacy.
This study’s objectives were to (1) To establish baseline hamstring stiffness measures for young competitive athletes and (2) determine effect of targeted neuromuscular training (TNMT) on shear wave stiffness of the hamstring. Regarding the first objective, it was hypothesized that hamstring stiffness would increase with age in high school basketball and college basketball athletes. Finally, it was hypothesized that TNMT intervention would decrease SWE stiffness in basketball athletes.
METHODS
Population
Six hundred forty-two lower extremities from 321 high school and collegiate basketball athletes (177 F: 139 M; Table 1) were examined for hamstring stiffness across a range of passive hip and knee flexibility prior to the start of their competitive basketball season. Two subjects were excluded from this cohort due to a lack of demographic data. The subject population was a cohort of convenience, recruited from high school and college basketball teams that compete near Rochester, MN, USA. Teams were contacted via a clinical coordinator and offered the opportunity to participate in research with no remuneration. Teams who agreed to participate in the study were cluster assigned to either the Control or intervention (TNMT) group prior to arriving for their first data collection. In this manner, all individuals from the same team were assigned to the same group, intended to reduce potential for data cross-contamination. This design has previously been employed for other training intervention studies.34–36 Group assignments occurred in a predetermined order and were assigned to a team based on when they accrued into the investigation. Subject recruitment spanned a three-year period. The current investigation was unblinded to both investigator and participant. Subjects knew they would either receive a targeted training intervention during regular practice warmups or that they would proceed through their season activities unchanged. Pre-season data collection was completed after the start of team activities, but prior to the first competitive game. Post-season testing was completed after the last competitive game. All activities in this study were approved by the institution’s Institutional Review Board (IRB 17-003905). Informed consent was obtained for all subjects over 18 years old. Informed consent and parent/guardian assent were obtained for all subjects under 18 years old.
Procedure
For the control group, no intervention was enacted. These subjects underwent regular season activities as directed by their teams and coaches, with no influence from the research team. For the TNMT group, the research team introduced a hamstring targeted dynamic warm-up program as an intervention focused on activating the hamstring musculature. This intervention was substituted in place of each team’s regular warm-up activities for 15 minutes twice weekly. Intervention dynamic warm-ups were initiated at the start of the season immediately following the preseason evaluation session and continued until the team was eliminated from playoff contention. As multiple teams were training at the same time, warm-up sessions were overseen either by the lead athletic trainer on the research team (TN) or by additional athletic training staff assigned to the participating schools. These additional staff received instruction from the lead athletic trainer prior to enacting the interventional dynamic warm-up protocol. For the TNMT group, the intervention period lasted approximately 10 weeks in duration for each team. Selection of dynamic warm-up activities were orchestrated by the lead athletic trainer and the program was designed to incorporate elements known to positively affect the hamstring musculature.37–40 Specifically, the dynamic warm-up was designed around the incorporation of elements of stretching, skipping/hopping, lunging, jumping/landing, concentric/eccentric hamstring loading, balance, and dynamic range of motion at the core, hip, and knee (APPENDIX 1). Static stretching remains controversial relative to its efficacy for injury prevention; however, multiple studies have indicated that static stretching aides in the reduction of hamstring injuries.41–45 Warm-up drills are known to improve neuromuscular control during running.40 While the value of flexibility and dynamic range of motion remain controversial to hamstring injury prevention, incorporation of eccentric hamstring loading has shown efficacy due to its’ ability to affect hamstring to quadricep (H:Q) muscle deficits.38,39,41 Lumbopelvic exercises were incorporated as they have demonstrated importance to lower extremity neuromuscular control and injury recovery.39
Data Collection
Ultrasound SWE was used to measure shear wave velocity (kPa) of the biceps femoris muscle at three leg positions (40%, 60%, and 80%) of the maximum passive 90-90 straight-leg raise position for each leg as previously described.10 Briefly, hamstring flexibility was assessed by a clinician who used a passive knee extension test and a digital inclinometer. Neutral position was considered to be ipsilateral hip and knee flexion both positioned at 90°.46 The three leg positions (40%, 60%, and 80%) were subject-specific and calculated from the maximum flexibility observed by the clinician. The greater trochanter and femoral condyle were then marked, and the midpoint was identified by the clinician for repeatable placement of the ultrasound transducer both within and between subjects. While lying supine, an assistant moved and held the athlete’s leg at each position for the clinician to measure the biceps femoris stiffness using ultrasound SWE at each position (GE Logiq E9, 9L-D transducer, GE Healthcare, Wauwatosa, WI). Ultrasound SWE captures the Young’s Modulus of soft tissues in kPa based on displacements of the shear wave beam the propagation across the tissue. The Young’s Modulus equation is as follows:
E=3ρ(αD/tmax)
where is the density of the medium, is the Gaussian profile of the beam, is a dimensionless diffraction parameter, and is the rising time.47 Three SWE images were acquired at each position for average values. Prior to lower limb manipulation, each subject was instructed to fully relax their muscles and allow the assistant to fully support the leg. To ensure that passive muscle stiffness was being obtained, random subjects were selected to be monitored by surface electrodes placed on the medial hamstring muscle. These electrodes would provide real-time audio feedback to ensure the subject did not actively engage the hamstring muscles and that the ultrasound SWE measurements were of passive muscle stiffness. Electrode subject selection was randomized based on the availability of the sensors as several subjects could be undergoing evaluation simultaneously. Throughout pilot testing and the first year of randomly selected subjects, electrodes confirmed that the hamstrings musculature was maintained in a passive state. Beyond this, electrode monitoring was determined to be redundant and ceased. Copious ultrasound gel and minimal pressure was applied to the ultrasound transducer probe to minimize tissue compression and artifact error in tissue stiffness induced from externally applied pressure. Muscle stiffness (kPa) was measured using shear wave velocities from the SWE elastogram calculated via custom designed MATLAB software.10 Following completion of preseason testing, 103 athletes (206 lower extremities) returned for post-season evaluations that repeated the identical process. Post-season evaluations were conducted within two weeks following each team’s playoff elimination. Whether or not an athlete returned for post-season testing, the Mayo Clinic athletic training staff embedded at each school tracked participants for occurrence of hamstring strain during the basketball season.
Statistical Analysis
For statistical analysis, data were separated by sex and a one-way ANOVA was used to assess hamstring stiffness differences between ages (14-18 years) with a Tukey’s post-hoc test to assess individual differences within each age year. A Student’s t-test was used to assess differences in hamstring stiffness relative to competitive level (high school vs. collegiate). Pearson correlations were used to assess association between age and stiffness at each orientation. A 2x2 ANOVA of Intervention (TNMT, Control) vs. Time (Pre-, Post-Season) was used to assess for statistical differences among these groups. Individual differences within groups were assessed via Tukey’s post-hoc test. All statistical analyses were performed in JMP Pro (version 14, SAS Institute, Cary, NC, USA). Significance was set a priori at < 0.05.
RESULTS
Of the 321 total athletes recruited into this investigation, 103 athletes returned for post-season testing. Of these 103 athletes who completed both preseason and post-season evaluations, 22 athletes were assigned to the Control group and 81 athletes were assigned to the TNMT group (Table 1).
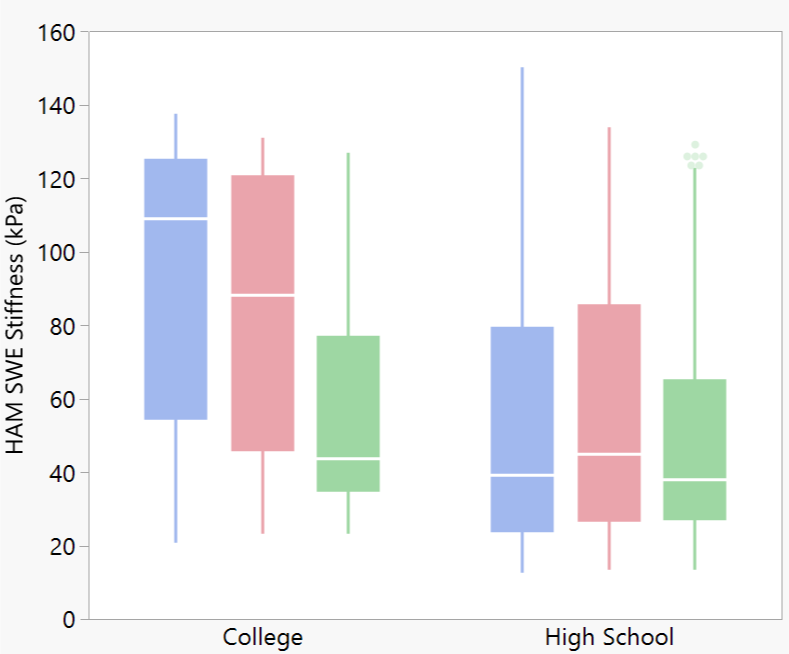
Age was a significant factor for hamstring stiffness in females at all three orientations (p ≤ 0.03) and in males at the 60% extended orientation (p < 0.01). However, there was no significant linear correlation between age and hamstring stiffness for either sex at any orientation (r2 ≤ 0.08). In females, hamstring stiffness peaked at ages 15 and 16 for the 80% orientation and age 15 for the 60% and 40% orientations (Table 2). In males, hamstring stiffness decreased by age 17 relative to age 14 and 15 in the 80% and 60% orientations (Table 2). Collegiate status was significant to hamstring stiffness for females at all orientations and for males at the 80% and 60% orientations. In each of these orientations, the collegiate athletes had significantly greater hamstring stiffness than their high school counterparts (Figure 1).
__60__(red)__and_40__(.png)
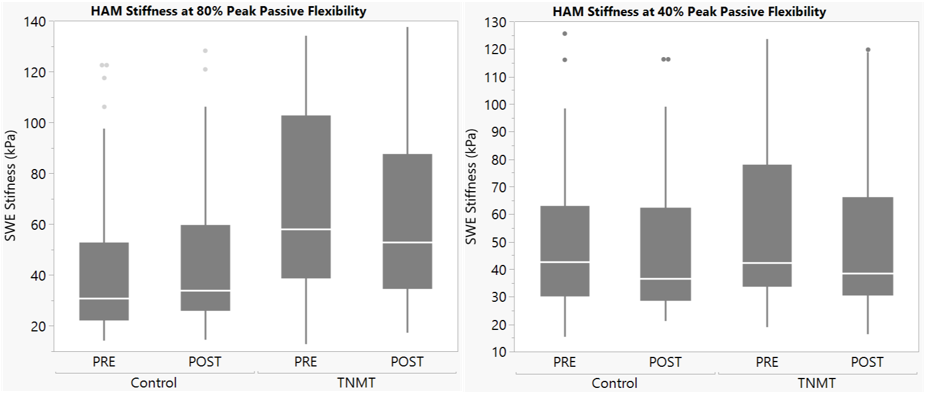
TNMT intervention was a significant factor at the 80% and 60% flexibility orientation (p ≤ 0.01), but not at the 40% orientation (p = 0.12). Time was not a significant factor when sampled across the whole cohort (p ≥ 0.28). However, within the TNMT group, Time was significant for the 80% and 60% orientation (p ≤ 0.05). In all cases where Time was significant, the TNMT group exhibited a decrease in hamstring stiffness from pre-season to post-season testing (Table 3, Figure 2). Despite being measured with the same SWE machine with the same collection settings, pre-season SWE stiffness was higher in the TNMT group than the control group (p < 0.01).
_and_40__of_peak_passive_flexion_(.png)
For female athletes, intervention was a significant factor as hamstring stiffness at the 60% flexibility orientation decreased after TNMT (p = 0.04). TNMT intervention with female athletes approached significance at the 80% flexibility orientation (p = 0.07). TNMT intervention in male athletes did not show a significant change in hamstring stiffness at any orientation (p ≥ 0.13; Table 4).
Across the whole population cohort, the embedded Mayo Clinic athletic training staff were able to track hamstring injury status on 286 athletes (89%). Due to COVID interruption, injury tracking on all collegiate athletes was lost to follow-up. Of the injury-tracked cohort, 193 athletes assigned to the Control group suffered three hamstring injuries, while 93 athletes assigned to the TNMT group suffered zero hamstring injuries. All three injured athletes were female (age = 16.7 ± 1.5 years; height = 173.0 ± 2.2 cm; mass = 79.4 ± 13.3 kg). The mean pre-season SWE hamstring stiffness among the three injured athletes was 27.1 ± 15.7 kPa at the 40% flexibility orientation, 26.9 ± 16.1 kPa at the 60% flexibility orientation, and 18.8 ± 5.1 kPa at the 80% flexibility orientation.
DISCUSSION
Within the baseline stiffness measures, there were significant sex differences in hamstring stiffness.10 Males showed significantly greater hamstring stiffness than females for all three flexibility orientations across all ages, 14-18. Neither males nor females showed linear correlation between age and hamstring stiffness. This data rejects the hypothesis that hamstring stiffness would increase with age in high school basketball athletes. Based on this data, hamstring stiffness does not appear to be directly associated with maturational or athletic development.
Researchers have determined that SWE muscle stiffness decreases with ageing from 20 to 94 years along with changes in muscle composition and dysfunction in extracellular fibers24,48; however, hamstring stiffness in adolescent athletes has not previously been disseminated. While neuromuscular efficiency muscle size and contractile force has been shown to increase as adolescents age, data regarding changes in elastic properties remains scarce.49–51 Past findings measuring musculotendinous stiffness, joint stiffness, and series elastic component (SEC) stiffness show differences in development and changes to muscle stiffness between the lower and upper extremities in adolescence.49,52,53 Previous data showed knee extensor stiffness decreasing as children age and identical measures for elbow flexor stiffness between children and adults.49,52,53 Similar studies have yet to be conducted using SWE stiffness as the primary measure of muscle stiffness in adolescence during development. The lack of association between hamstring stiffness and age during adolescence likely indicates a limited influence of pubertal status on muscle stiffness; however, pubertal status was not assessed in the present investigation and further validation is warranted.49,54 Likewise, strength was not directly assessed in this study, so it was not possible to determine if SWE stiffness was directly correlated with athlete strength.
Unlike age, level of competition was a significant indicator for increased hamstring stiffness in both sexes. The present data supports the hypothesis that collegiate athletes would have greater hamstring stiffness than high school athletes. In conjunction with increased hamstring stiffness, musculoskeletal injury incidence and sport-specific performance attributes also associate with higher levels of competition.25,55 Accordingly, muscle stiffness may be relevant to both injury prevention and sports performance as data from the current study demonstrated that hamstring stiffness is modifiable in female athletes through a minimal regimen of TNMT. Despite these fiindings, further investigation is warranted to determine whether muscle stiffness has a causal influence on injury prevention within sports as musculoskeletal injuries increase dramatically between high school and collegiate levels.27,55
The present data indicates that a TNMT hamstring warm-up program is likely to decrease hamstring stiffness. The results of the study show lower postseason hamstring stiffness compared to the control group. This supports the hypothesis that TNMT intervention would decrease shear wave stiffness in basketball athletes. Throughout this study three hamstring injuries occurred. Each reported injury occurred in a female high school athlete who was not assigned to the TNMT group. Further investigation is necessary to determine whether dynamic warm-ups targeted to specific muscle groups can offer prevention against soft-tissue injuries in females during athletic participation.
Further, regarding the three injured subjects, the SWE hamstring stiffness in this sub-cohort was different than the whole study cohort, as the three injured athletes individual SWE values were below the cohort mean. This fact remained true regardless of what age bracket the injured subjects were compared against. Relative to the position and limb where SWE was measured, the first injured subject was between 0.12-1.09 standard deviations below the cohort mean, the second injured subject was 0.44-1.02 deviations below the mean, and the third injured subject was 1.12-1.40 deviations below the mean. While this granular data demonstrates that injuries only occurred in athletes with hamstring stiffness deficiencies, the current results are unable to conclusively prove that hamstring stiffness is a primary cause of predisposing athletes to injury during a competitive season.
Optimal hamstring stiffness for basketball athletes is likely to lie along a Bell curve where extremes of extremes of high and low stiffness increase injury risk. It is also interesting to note that overall subject population increased hamstring stiffness with increased extension in the passively manipulated straight leg extension (Table 3), but the injured cohort did not exhibit this trend. Additional investigation is necessary to determine whether these functional mechanics have clinical implications. Further study is also warranted due to preseason differences in the Control and TNMT groups. Measurements were recorded with identical methodology between groups, so it remains unknown as to why the control group was initially less stiff than the TNMT group. It is possible that the TNMT group would have been more susceptible to influence due to their higher initial stiffness.
The current intervention program, TNMT, included eccentric resistance exercise such as Nordic hamstring (NH) eccentric strength training which is associated with reduced injury.56–58 However, studies show while NH strength training lowered future hamstring strain injury post-intervention, data showed no significant changes to muscle fascicle length, stiffness, or eccentric hamstring strength occur.56 The results of this study compliment these previous data and demonstrate that mechanical variables outside increased strength or muscle length56–58 may contribute to muscle strain prevention. Thus, further studies are warranted to determine if the decrease in injury rate related to TNMT is directly associated with changes in muscle stiffness or occurs through other biomechanical modifications.9
Data from this study support past literature that indicates TNMT effectively reduces injury rate and muscle stiffness.27,28 Furthermore, the present data demonstrates that the magnitude of response to TNMT varies by sex. Compared to female athletes, hamstring stiffness in males responded less significantly to TNMT at all flexibility orientations. Reduced stiffness response seen in male athletes is exacerbated by a substantially higher risk of hamstring injury and re-injury.4,12 Thus, additional study into the utility of injury prevention programs for male athletes may be warranted. More research is needed to determine the cause for sex differences associated with TNMT effectiveness. Future studies may look at TNMT intervention in male and female college athletes who show higher overall hamstring stiffness than their high school counterparts, to elucidate whether the magnitude of hamstring stiffness plays a role in TNMT effectiveness while isolating sex differences.
As with all investigations, the current study had several limitations. The stiffnesses measured by SWE are orders of magnitude lower than the elastic modulus and yield stress for hamstring tissue.59 Therefore, we are using hamstring stiffness measurements as a surrogate, as opposed to an absolute measure of hamstring tissue properties. The use of surrogate measures instead of yield stress or elastic modulus may distort the significance of TNMT influence and its relative association with risk of hamstring injury.60 Given that multiple schools underwent TNMT training simultaneously, a single universal athletic trainer could not be used for this study. This introduces potential variation in facilitation of TNMT intervention, but improved generalizability. To combat any variations in administration of intervention across trainers, all schools implemented the same program, each school trainer was taught by the same interventionalist, and a written protocol was provided. While the population cohort for this study encompassed athletes between ages 13-22 years, data was captured on an insufficient number of athletes aged 13 (n = 3), 19 (n = 9), 20 (n = 3), 21 (n = 8), and 22 (n = 3) to include them as separate groups within the age-based statistical analysis.
In addition, this investigation experienced limitations in the collection of post-season data that accounts for the large number of athletes unable to be tested at follow-up. Post-season data collection was deterred by two events: 1) teams that were assigned to the control group felt a lack of investment in the investigation and subjects were reluctant to return for post-season testing, 2) government mandated shutdowns due to the COVID pandemic prevented the capture of post-season data in Spring 2020. These unfortunate events contributed to substantial attrition in participants in postseason data collection, limiting the internal validity of the study. Unfortunately, this limitation was unavoidable, but the captured cohort was deemed acceptable for statistical analysis as each group had a minimum of 21 athletes that completed full analysis. This outbreak also impeded the planned implementation of collegiate TNMT groups for the 2020-2021 basketball season, which resulted in zero collegiate TNMT subjects (Table 1). Lastly, the GE Logiq E9 had a ceiling of SWE of 120 kPa. As hamstring elastic modulus exceeds 2500 kPa,59 even in a passively flexed state, many SWE stiffness values for the hamstring stiffness were saturated during imaging, which likely increased variability and standard deviations observed in this study. Future studies should incorporate SWE technology with a larger range of measurement for improved precision. Finally, the clinical significance of SWE stiffness measurements remain undescribed. SWE measurements on muscle tissue are reliable within a session but lack precision and offer substantial variability within a whole population,61 as is herein observed with the standard deviations. Intra-session standard error of the mean for SWE stiffness on lower extremity muscles are between 8-12 kPa,61 which should be considered when accounting for clinical applicability of statistical findings.
CONCLUSION
Higher SWE measurements have been correlated with increased risk of injury and groups at higher risk of hamstring injury (i.e., males and collegiate athletes). As such, potential exists to utilize SWE stiffness as a surrogate for injury risk; however, further study is necessary to substantiate these claims. Age did not factor into hamstring stiffness or injury. The current findings contradicted previous research citing correlation between increased hamstring injury and decreased stiffness with increased age and may be indicative of a separate trend in adolescent cohorts. Data from this study reiterated that TNMT intervention can lessen muscle stiffness and incidence of re-injury. However, the current data uniquely exhibited that females showed greater response to TNMT, and that intervention effectiveness can be sex specific.
Disclosures
The authors have no financial disclosures or conflicts of interest.
ACKNOWLEDGEMENTS
This investigation was funded by and NBA / GE Collaborative Grant, as well as National Institute of Health grants from National Institute of Arthritis and Musculoskeletal and Skin Diseases R01-AR055563 and L30-AR070273 and the National Institute of Children and Human Development K12-HD065987. We also acknowledge the contributions of Rena F. Hale, PhD, to the early stages of data collection for this project.