INTRODUCTION
Non-contact anterior cruciate ligament (ACL) injuries make up 70% of all ACL injuries,1 with rapid deceleration, single-leg landing and sidestep-cutting movements being the main contributors.1,2 Females who display poor neuromuscular control of the lower body when performing these high-risk movements resulting in high knee valgus and knee internal rotation moments that could strain the ACL are 4-6 times more susceptible to ACL injury than males.3 While several factors combined may incite an ACL injury,4 high knee valgus moments (KVM) during unplanned sidestep-cutting (USC) can rupture the ACL.3,5 KVM was reported to predict ACL injuries with 73% specificity, 78% sensitivity and an r2 of 0.88.3 Video-based studies have also reported that most ACL ruptures occur during initial foot contact during the weight-acceptance phase of USC when the knee goes into valgus.6–9 USC reportedly results in larger peak frontal knee moments in comparison to a single-leg landing.10
Netball, a team ball-sport with high female participation rates and over 20 million participants globally, involves multiple repetitions of single-leg landing and USC and accounts for many non-contact ACL injuries.11,12 Not only is recovery from ACL injury costly, full return to sport post-ACL reconstruction can take up to twelve months.13,14 Knee injuries were reported to be the most disabling injury in netball.15 The identification of non-contact ACL injury risk through periodic screening is therefore crucial.
The current gold standard for assessing knee moments during sporting maneuvers involves the use of three-dimensional (3D) motion analysis systems that are costly, time-consuming to operate and often inaccessible to the masses. Consequently, simple-to-administer screening tools are increasingly sought after to replace these sophisticated laboratory-based tests that can be used to infer sporting performance and injury risk. Examples of which include the Landing Error Scoring System and Tuck Jump Assessment that have been used to quickly recognize injurious postures such as knee flexion and valgus angles during double-legged landing that may injure the ACL.16,17 Relating to sport-specific maneuvers such as sidestep-cutting and single-leg landing, where unilateral balance, lateral hip and trunk control, and proper alignment of the lower extremity all contribute to ACL strain,5–7,18,19 a screening tool assessing these elements may be more relevant. An example of this includes the quick and simple-to-administer Y-Balance Test, which is performed unilaterally, replicating the stance after a single-leg landing. Correlations were found between the posteromedial and anterior reach distances with knee flexor and internal rotation moments, respectively, during single-legged jump-landing, and was suggested to be a useful screening tool for inferring knee moments contributing to non-contact ACL injury risk.20 No correlations between the Y-Balance Test and KVM during USC were found. Another screening tool, the Functional Movement Screen (FMS™),21,22 did however show potential to illuminate non-contact ACL injury risks.21,22
The FMS™ assesses seven fundamental movement patterns that require mobility and stability of the body and limbs.20,21 These seven movements include the 1) Deep squat (DS) 2) Hurdle step (HS) 3) In-line lunge (IL) 4) Active straight leg raise (ASLR) 5) Trunk push-up (TP) 6) Rotary stability (RS) and 7) Shoulder mobility. Each movement in the FMS™ is rated by an assessor from 0 to 3 based on their ability to perform the movements without compensatory actions.23,24 A composite score of 14 and below out of the maximum 21 has been associated with high injury risk,25–29 but has also been reported by some studies to be limited in predicting injury.29–32 Notably, when the shoulder mobility test is removed from the seven movements, a stronger correlation was shown to exist between the scores of the other six movements and lower extremity injury.26
While the majority of studies assessed lower extremity injury incidences post-testing, two were able to link the FMS™ scores to injury mechanism. In one study, it was reported that higher composite scorers displayed less spine and frontal plane knee movement during performance of the FMS™ than lower scorers22; both contributing factors to high KVM during the sidestep cut. In another study, clinical measures used to identify knee abduction(valgus) moment probability during a drop jump landing, albeit a proxy measure of actual KVM, found an increased risk for non-contact ACL and lower extremity injuries when FMS™ composite scores were lower than 14.21 Could the FMS™ scores also be used to identify participants who demonstrate high KVM during the sport-specific maneuver of USC and by means of inference indicate risk of non-contact ACL injury?
The purpose of this study was to investigate whether externally applied peak KVM during weight-acceptance phase of USC were correlated with the composite and component scores of the FMS™. The presence of correlations may present a screening tool that can be used to infer KVM, a contributor to non-contact ACL injury, during USC in netball.
METHODS
Participants
Fifteen well-trained female netballers (age: 24.6 ± 2.5 y; height: 1.75 ± 0.1 m; mass: 63.2 ± 7.4 kg) from the Singapore National Open’s team participated in the study. A minimum of eleven participants were required for this study, according to G*power analysis (v3.1.9.2, Heinrich-Heine University, Düsseldorf, Germany), to detect a Pearson’s correlation coefficient of r = 0.75 (β = 0.80, α = 0.05, two-tailed). This effect size of r = 0.75 was set based on correlations found in a study by Chorba and colleagues (2010).26 All participants had no pre-existing lower limb injury and were proficient in performing USC on either leg. Participants were briefed that they would perform both the USC and FMS™ with the order randomized to eliminate sequencing effects. In addition, participants were asked to indicate if they were menstruating at the time of testing as it can affect ligament laxity.33 All procedures and forms were approved by the Singapore Sport Institute Institutional Review Board, and all participants provided their informed written consent before data was collected.
Instrumentation & Procedures
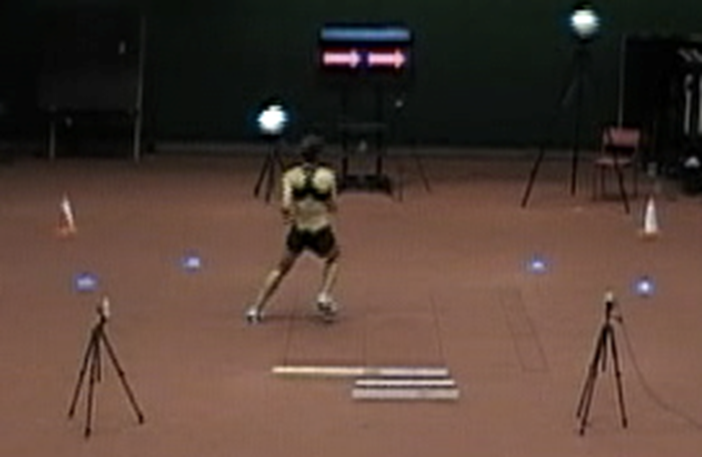
Participants performed bilateral USC (Figure 1) at a cut angle of 45o ± 10o toward the left or right by reacting to an arrow presented on a screen in front of them.34 The arrow direction sequence was randomized but counterbalanced in order to minimize anticipation, bias or sequencing effects. Participants were required to perform this task with an approach speed of 4.5 ± 0.5 m/s that was monitored by two pairs of customized timing gates, and react immediately with a sidestep cut in the direction of the arrow displayed on a screen upon passing through the second pair of gates. The 45º ± 10º cut angle was ensured by requiring participants to pivot on the force plate and then run through either pair of cones placed 45º to the left and right from the middle of the force plate. To avoid force plate targeting, participants were instructed to focus on the screen ahead of them during the approach run. Further, a cone was placed in a participant-specific position to demarcate the starting location of each participant, determined during familiarization, so that running with their natural cadence resulted in foot contact on the force plate. Eight familiarization trials were provided for USC.5 For the actual test, a trial was deemed successful when 1) the participant’s entire foot landed completely within the designated force plate and 2) the participant ran through the correct pair of cones after performing USC. Demonstration and familiarization were done prior to testing. Unfortunately, due to logistical reasons and the positioning of the force plate, only data from USC to the right side (i.e., left foot ground contact) could be obtained and analyzed. A total of three successful trials were required from each participant on their left leg. The prior decision was made to assess the left leg, between the two, as it was the non-dominant leg for majority (13 out of 15) of the participants. Females have been reported to suffer from non-contact ACL injuries more frequently on their non-dominant leg.35,36 Participants verbally indicated which leg they would perform a single-leg jump push-off with. This leg was determined as the participants’ dominant leg while the other leg was determined as their non-dominant leg. Consequently, data of only 13 out of 15 participants’, whose left legs were their non-dominant legs, were presented and discussed.
.png)
Three-dimensional body kinematics during the USC were captured using twelve 3D opto-reflective motion capture cameras (Vicon Industries Inc., Edgewood, NY, USA) at a sampling rate of 250 Hz. A single 0.6 m by 0.9 m Kistler force plate (Kistler 9287CA Piezoelectric, Winterthur, Switzerland) captured ground reaction forces synchronously at 1000 Hz. Thirty-two retro-reflective markers, following the University of Western Australia (UWA) Lower Limb Model and Marker Set, were affixed to selected anatomical landmarks on each participant to facilitate 3D motion analysis.37 Detailed description of data collection with this marker set set-up and calibration can be found from previous research by Besier and colleagues.37
Captured kinematic and kinetic data were analyzed in Vicon Nexus (version 2.3, Oxford Metric Group, Oxford, UK). Knee moments were calculated, through inverse dynamics, during the weight-acceptance phase of the USC where the peak of KVM occurred, and when the ACL load is high.9 Output moments calculated were externally applied and indicated as “+” for valgus and “-” for varus. Marker trajectories and force plate data were filtered with a low-pass (4th order, zero-lag) Butterworth digital filter at a cut-off frequency of 20 Hz after residual analysis and visual inspection of the data.38 Final KVM value for each participant was presented as the mean of peaks from three successful trials and normalized to their respective heights and masses.
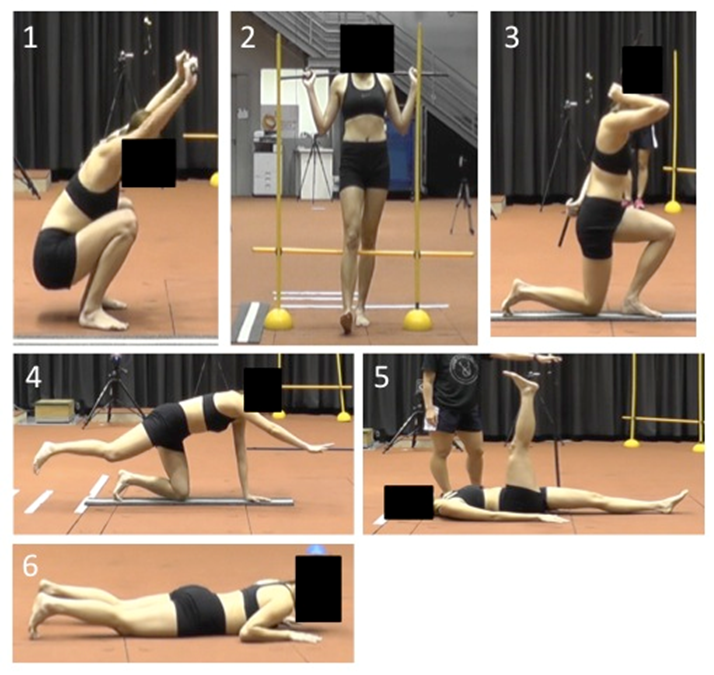
Participants performed the six movements (Figure 2), 1) Deep squat (DS) 2) Hurdle step (HS) 3) In-line lunge (IL) 4) Rotary stability (RS), 5) Active straight leg raise (ASLR), 6) Trunk push-up (TP), of the FMS™ in a randomized sequence, with the shoulder mobility test removed. Demonstration was provided prior to each movement test according to the standardized procedures and verbal instructions described by Cook and colleagues.23,24 Two familiarization trials; necessary in order to eliminate any possible learning effects39; and three test trials per side were required for each movement. An adapted half-point scoring from 0 to 3, in 0.5 increments, was adopted as the original whole-number scoring had been critiqued to be of low sensitivity where a score of 2 can be achieved in multiple ways.22 Zero point was awarded for participants who experienced any pain while performing any of the movements, and 3 points was awarded for participants who could perform the movements in accordance to the FMS™ guide.23,24 For movements that were performed bilaterally, the scores on the left side were used as only the left KVM, during sidestep cutting to the right, were recorded. Composite scores were obtained by summing the six movement scores, providing a maximum of 18 points. Both appraisers of the FMS™ were trained through a minimum of three weeks of pilot testing and were familiar with the half-point scoring criteria for each movement prior to data collection for the research.
.png)
All statistical analyses were done using SPSS (IBM Corp., SPSS Version 22.0, Armonk, NY, USA) with significance level set at p ≤ 0.05. Intra-class correlation coefficients (ICC) (model 2,1) were used to establish interrater and intrarater reliability for the FMS™ composite. Both raters appraised the three participants performing the six movements of the FMS, that was recorded on video, and repeated this appraisal of the same videos on another separate occasion. Each rater’s score on both occasions were used to assess the intrarater reliability, while both their scores for the second round of appraisal were compared to assess interrater reliability. Cohen’s Kappa (κ) was used to determine the interrater reliability of the component (individual movements) scores.25 Kendall’s tau-b (τb) was used to assess the associations between normalized peak KVM with FMS™ composite score and its six component scores; this statistical analysis was chosen due to the small sample size and its ability to compare between continuous and ordinal data (i.e. KVM and FMS™ component scores).40 Means ± standard deviations (SD) are also presented for each variable. All variables were tested for outliers.
RESULTS
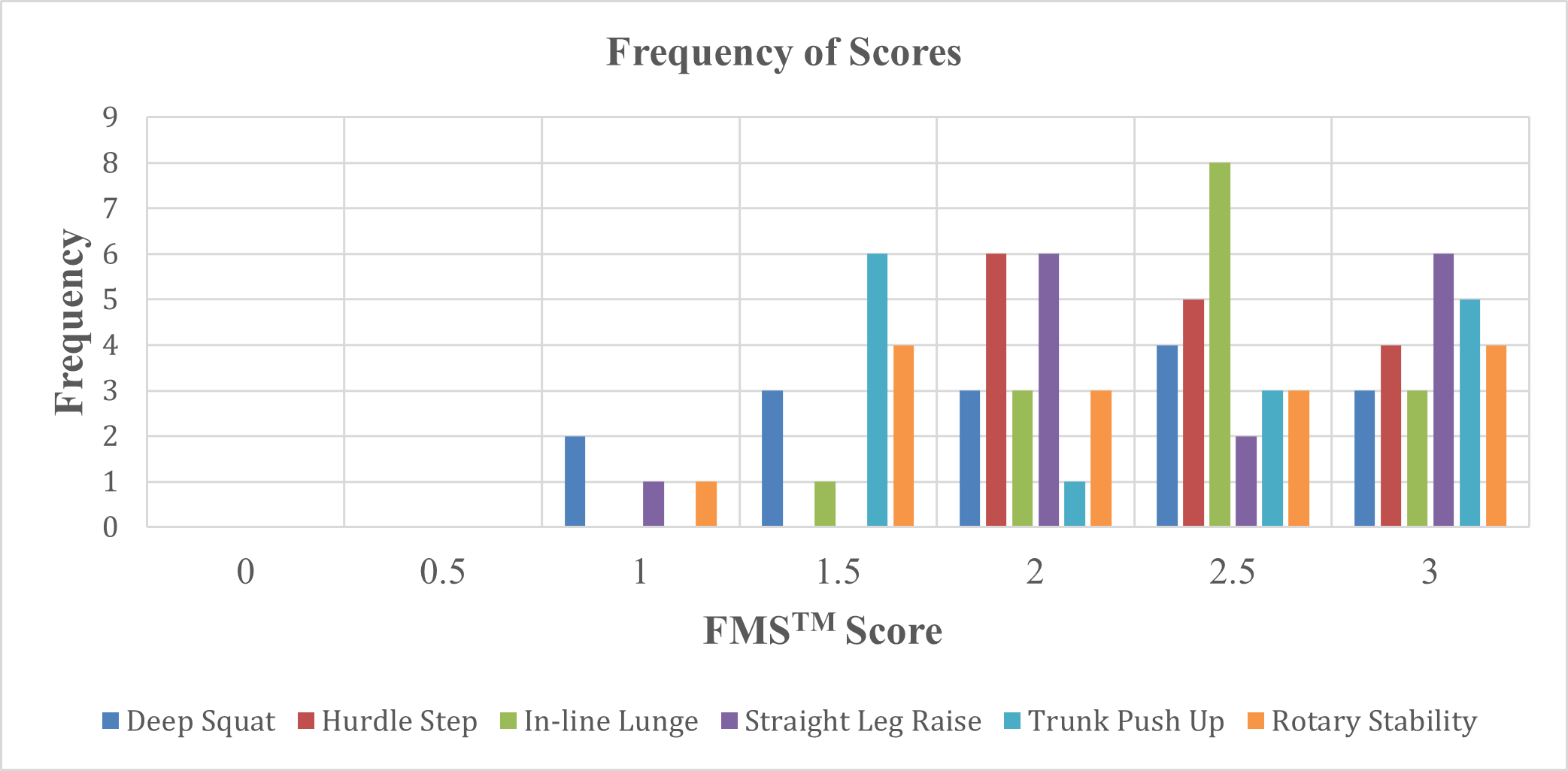
ICC displayed good to excellent intra- and inter-rater reliability with single measures ranging from 0.62 to 0.84 at 95% confidence interval, for the FMS™.41 Cohen’s κ displayed a moderate agreement between both raters, κ = 0.50 (95% CI, 0.31 to 0.68), p < 0.01.42 Table 1 details the mean ± SD of KVM and FMS™ composite score, τb and significance level for the various FMS™ scores and peak KVM during USC. Figure 3 displays the frequency of scores for each movement. No significant correlations were found between peak KVM and any of the seven scores (0.09 < p < 0.95) (Table 1).
.png)
DISCUSSION
The present study examined the correlation between FMS™ scores and peak KVM during USC in well-trained female netballers. The USC tasks were performed on the left leg, corresponding to the non-dominant legs of all participants. While past studies have reported on the FMS™’ ability to predict generic musculoskeletal injury predisposition retrospectively,26–28,43 the current study attempted to identify the relationship between FMS™ scores and peak KVM, a contributor to non-contact ACL injury, during USC, to assess the FMS™ diagnostic utility.30 Neither the composite nor component scores of the FMS™ showed any significant correlations with peak KVM.
To understand why the FMS™ composite score may be able to predict lower extremity injuries in general but has thus far not been able to predict specific injuries, the nature and type of movements tested in the FMS™ need to be examined. The FMS™ requires individuals to perform a series of movements that are meant to illuminate issues with stability, mobility and motor control dysfunction.23 However, the FMS™ is limited in its utility to predict specific sporting injury risks as many athletic movements encompass elements such as power, endurance, and change of direction; elements that differ considerably in nature from the movements tested in the FMS™.23,24,44 Several authors have, however, reported correlations between the composite scores and lower extremity injury risks.25–29 Afterall, the FMS™ component movements test elements of strength, posture and movement capacities that are related to performance of the lower limb. For example, core strength affects lumbo-pelvic stability, which in turn has a cascading effect on alignment, structural loading, and injury implications of more distal lower limb segments and joints. This is assessed through the TP and RS movements.23,45 Postural stability, an indication of neuromuscular control and contributor to intersegmental joint forces that can strain the lower extremity soft tissue structures, is assessed through the HS and IL.23,46 The lack of hip, knee and ankle range of motion and strength, associated with dysfunctional lower limb biomechanics during sporting movements and increased injury risk, are assessed by the DS, ASLR, HS and IL.23,24,46–48 As a result, when assessing an individual’s ability to perform these various tasks using a composite score, it represents the cumulative propensity for which this individual may be subjected to any or all of the abovementioned risks linked to lower extremity injuries.
Considering the abovementioned, the past authors that found correlations between FMS™ composite scores and lower extremity injury rates assessed injury incidences retrospectively, over a period after the FMS™ was performed.26–28,43 One reason for the correlations found could be that overuse injuries arise from poor movement patterns that are repeatedly performed.23 In which case, it is possible that the poor scores on the FMS™ may associate with eventual injury incidences when these compensatory movement patterns are repeated over time. Another reason could simply be due to an increased exposure to confounding effects in the period between the conducting of FMS™ test and time of injury occurrence.30
In the current study, the FMS™ was investigated specifically for its correlations with peak KVM during USC. With the above explanation regarding the composite score and its higher sensitivity but lower specificity, component scores were also assessed in order to investigate if specific FMS™ movements showed correlations with peak KVM. Amongst the six movements tested, the HS was the most replicable in its posture to that of USC; unsurprisingly, it was also the only component test that showed correlation that approached statistical significance (τb = - 0.39, p = 0.09). Both are performed with an upright single-leg stance where emphasis is on trunk and pelvic stability to maintain dynamic stability, with proper lower extremity alignment while lifting the opposite leg.23 Despite the similarities in posture, neither the HS, nor any other movements displayed significant correlations.
What may be lacking in the FMS™ movements compared with movements in a sport-specific context are the conditions in which these postures are executed. In unplanned scenarios such as USC, the knee can be loaded up to twice that of planned scenarios.49 This raises the utility of the planned FMS™ movements in assessing injury risk during unplanned scenarios. Boey and Lee echoed this supposition when they found correlations between reach distances in the planned Y-Balance Test with knee moments during a planned forward single-leg jump-landing task but not with an USC.20 Additionally, other instances when high KVM were recorded during single-leg stance, participants had either landed from a lateral or diagonal jump50 and/or in the presence of perturbations,51 and/or landed with high velocities such as a running take-off landing.52 It is therefore important that the movement tasks within the selected screening tests encompass some of these aforementioned conditions in order to make it more specific for assessing non-contact ACL injuries. Tran et al. suggested the Landing Error Scoring System to be a better predictor of ACL injury than the FMS™ due to its faster and higher-impact movements; elements present during ACL injury occurrences; assessed compared to the slower controlled movements of the FMS™.53 Alternatively, advanced methods utilizing two-dimensional video to reliably predict 3D knee moments during unplanned sidestepping could be considered most specific in identifying injury risk as the movement assessed is that performed during the sport and can comprise the sport-specific conditions such as an unplanned scenario.54 It is postulated that in order for a screening test to be specific to non-contact ACL injury risk during USC, one or more of the following conditions in the movement task assessed needs to be included: 1) performed in single-leg stance, 2) replicate a similar motor pattern, 3) executed in an unplanned scenario, 4) include a weight-absorption phase, 5) approached from high velocity, and 6) movement in a lateral or diagonal direction.
Unlike a typical exploratory study assessing correlation between a screening test and subsequent injury occurrence, this study investigated if there was a correlation between the FMS™ scores and peak KVM during USC in the lab with the aim of preventing the onset of injury in the first place. Unfortunately, the six-movement version of the FMS™ protocol did not show any such relationships. To identify non-contact ACL injury risk during specific sporting maneuvers, the FMS™ movements may need to be modified or supplemented to account for the maneuver-specific mechanisms and conditions under which they are performed.
Limitations
Firstly, the sample size of 15 in this study is small despite our power analysis reporting that 11 was enough to yield a power of 0.8. Secondly, due to logistical reasons, only the left leg; the non-dominant leg for majority of the participants; reflected as USC towards the right, could be assessed. The relationship between FMS™ scores and peak KVM on the dominant leg during USC should also be explored to expand the current findings.
Future Research
Future research utilizing the FMS™ should consider supplementing it with additional tests to accurately assess dynamic movements. In addition, exploration of the knee flexor and internal rotation moments, that can also contribute to strain of the ACL, during the USC with FMS™ scores may provide new insights on its utility. Finally, a larger sample size comprising athletes from more variety of team sports would better confirm any results and allow generalizability to participants of team sports.
CONCLUSIONS
The results of this study indicate that there are no significant correlations between six-movement FMS™ scores and peak KVM during USC. The FMS™ as used in past studies may be able to identify generic risk of lower extremity injury due to compensated mechanics which should be corrected promptly before an injury eventually occurs. However, in order to screen for non-contact ACL injury risk during USC, movement tasks within the screening assessment may need to be more similar in mechanism and conditions to that of the maneuver that puts an individual at risk of that injury.
Declaration of interest
The authors declare no funding resources and no conflict of interest in the authorship and publication of this contribution.