INTRODUCTION
The glenohumeral joint requires the coordinated neuromuscular interaction of several cooperative joints, balancing its contrasting roles of mobility and stability. The increased mobility can contribute to shoulder instability-related injuries1,2 such as traumatic anterior shoulder instability (TASI). TASI generally occurs when excessive forces during a traumatic event displace the humeral head anteriorly, out of the shoulder socket, resulting in the joint surfaces completely losing contact3 and may lead to recurrent anterior shoulder instability.
The shoulder is the most frequently dislocated joint; occurring in 8.2-23.9 per 100,000 people per year.3 Following TASI, there is a higher risk (39%) of experiencing recurrent anterior shoulder dislocation.4 Estimates of TASI in various countries reported incidences per 100,000 of 23.9 (USA), 23.1 (Canada), 27.5 (Sweden), 56.3 (Norway), and 12.3 (Denmark). TASI incidence is highest in the late teens and early twenties (15-20 years, proportion of recurrent instability: 51%), and is attenuated with increasing age (21-40 years, proportion of recurrent instability: 36%) with higher incidence in males (71.8%) and in athletes.5–7 Within the National Collegiate Athletic Association, glenohumeral instability occurs 12% per 1000 athlete exposures with the time lost to the sport on average greater than 10 days,8 with a return to normal activity ranging from five days to six months.9
Traditional rehabilitation for shoulder dislocation has a success rate of only 20%.10 Commonly, the treatment for TASI is surgical intervention followed by rehabilitation.11,12 However, 20% of surgeries after an initial TASI event, even amongst athletes, are unnecessary and an additional 14% of surgeries are unsuccessful,13 and there is an estimated pooled failure rate of 13.7% (7.7%-19.6%) for arthroscopic repair of shoulder dislocation.14 Hence, more effective non-invasive treatment modalities would be a benefit to this population.
The comprehensive conservative management approach to TASI requires several months to complete. Conservative management typically involves three to four weeks or up to six weeks of immobilization15 followed by a variation of rehabilitation timelines.9 During the management of athletes with TASI, the demands to return to play are much higher than non-athletes and an accelerated program would be more fitting for this population. Buss et al.16 examined 30 in-season athletes with TASI and found that they returned to play within 10.2 days. Consequently, ten athletes sustained a recurrent instability episode, and 16 eventually underwent surgical stabilization during the subsequent off-season. Furthermore, this expeditious return to play protocol appeared to center around allowing athletes to return to play faster instead of considering the long-term effects. Alternative tools that could be effective in accelerating recovery would be a valuable addition to the health professional’s tool box of rehabilitation implements.
An oscillation tool such as the Bodyblade™ has the potential to improve efficiency and efficacy in a rehabilitation program.17 Bodyblade™ has been shown to produce kinetic chain movement for the upper and lower body.18 Additionally, it has also been found in a number of studies to produce higher electromyography (EMG) activity than traditional rehabilitation tools,19–21 which may enhance the traditional conservative management approaches to TASI. The primary rationale for the high EMG activity could be due to the higher movement velocity required to oscillate the Bodyblade™. The increased velocity incurs enhanced concentric activity and decreased eccentric activity. The same concept occurs when slowing down the Bodyblade™, eccentric activity enhances, and concentric movement decreases.22,23 In comparison to dumbbell exercises, the Bodyblade™ reaches greater EMG activity exceeding 50% of maximum voluntary isometric contraction (MVIC)20 and can activate multiple muscle groups compared to other traditional rehabilitation tools. These factors lend further credibility to the exploration of effective and efficient oscillation devices to accelerate recovery.
There is limited research available on the benefits of this tool in rehabilitation. A case study10 reported on treatment of an individual with a shoulder dislocation using a Bodyblade™ over 11 visits. Following the Bodyblade™ treatment, pain rating scales reduced from 4 to 0, range of motion measures returned within normal range with the exception of external rotation, strength returned and exceeded contralateral limb strength and the Western Ontario Shoulder Index (WOSI) decreased from 482 to 46. Oliver et al.21 had participants perform common shoulder rehabilitation exercises with the Bodyblade™ and reported moderate to moderately strong activation of upper and lower extremity muscles suggesting that these Bodyblade™ exercises may be utilized for a shoulder rehabilitation program. While current tools used for shoulder rehabilitation include elastic resistance bands, weighted balls, medicine balls, cuff weights, and dumbbells,19,22 Bodyblade™ has been found to achieve high EMG activity in the scapular stabilizers,22 shoulder,20 and core musculature.18,20 Hence, there is a dearth of research investigating the effectiveness of the Bodyblade™ as a major component of a sustained rehabilitation training program
Bodyblade™ recommends that an individual resist oscillation for up to 60 seconds to improve strength, pain relief, attain aerobic benefits, and improve proprioception.17 However, these claims have not been validated. The exploration of this multifaceted oscillation tool has the potential to improve traditional shoulder rehabilitation guidelines. Therefore, the purpose of this study was to compare three different protocols: Traditional, Bodyblade™, and Mixed (Traditional & Bodyblade™), for shoulder rehabilitation on athletes with TASI.
METHODS
Participants
Thirty-seven student-athletes were recruited from five community colleges (Table 1). Five of the 37 participants were left hand dominant and 14/37 had injured their left shoulder. The mean time since injury was 4.77±4.78 months with a range of one week to 12 months. Using controlled randomization, participants were randomly allocated regarding sport, training group, sex, type of athlete and time since injury. The sample size was justified by a priori power analysis (α= .05, β= .80 and meaningful effect size (ES) difference of 0.50: moderate magnitude), which indicated a minimum of 22 participants. Participants were considered to participate in the study if they had a history of TASI episode(s) and actively enrolled in an athletics class at their college. Researchers were blinded to the group allocation.
The inclusion criteria consisted of the participant indicating a TASI episode which was defined as a shoulder instability event in the prior 12 months based on the Shoulder History Questionnaire, cleared to participate in the demands of their respective sport by an orthopedic surgeon based on pre-participation physical examinations, or was cleared with recommended exercises supervised by a certified athletic trainer at selected colleges. The mechanisms of injury were shoulder abduction with external rotation with 18 participants, shoulder abduction and external rotation with external force with 15 participants, three participants fell onto an outstretched hand and one participant was injured swinging a baseball bat. Participants were excluded from the study if they had a surgical repair for shoulder instability, upper or lower extremity amputation, vestibular disorder, recent fractures (<6 months) to the involved upper extremity (clavicle, scapula, humerus, ulna, radius, metacarpals, or carpals), injury to the neck, elbow, hand; tendinitis, sprain or strain, undergone any treatment for the inner ear, sinus or upper respiratory tract infection, or concussion in the prior three months, undergone nonsurgical rehabilitation or under any care for their shoulder with an orthopedic surgeon, physical therapist, or athletic trainer. The participants were not undergoing any rehabilitation from a physical therapist or athletic trainer during the study.
The study design consisted of a randomized-controlled longitudinal training study (pre-test, mid-test [4 weeks], post-test [8 weeks], and a three-month follow-up). Participants were placed in one of three experimental groups. The Traditional (elastic resistance) protocol was designed to activate scapulothoracic musculature and promote optimal scapular positioning (n = 12).21 The Bodyblade™ protocol intended to activate scapulothoracic musculature at various movement planes (n = 13).18–20,22–26 The Mixed group was designed to include a combination of both Traditional and Bodyblade™ protocols (n = 12). Approval for the study was obtained from the Institutional Review Board (IRB) at Rocky Mountain University (IRBNet ID # 889924-10 – Protocol # 160443-03). The informed consent forms were obtained from all participants before the beginning of the study.
Exercise Protocols
The study was an eight-week intervention performed three times a week with a three-month follow-up under the guidance of supervising athletic trainers. An eight-week duration was chosen as both neural and morphological changes, which contribute to the objective of increased strength are reported to occur in an eight-week training program,27,28 and the duration would be reasonable to ensure participant retention. Each group progressed weekly by either progressively adding resistance, repetitions, or increasing time and intensity. Participants needed to attend at least two sessions per week and were instructed that they would be removed from the study if they missed more than four sessions overall.
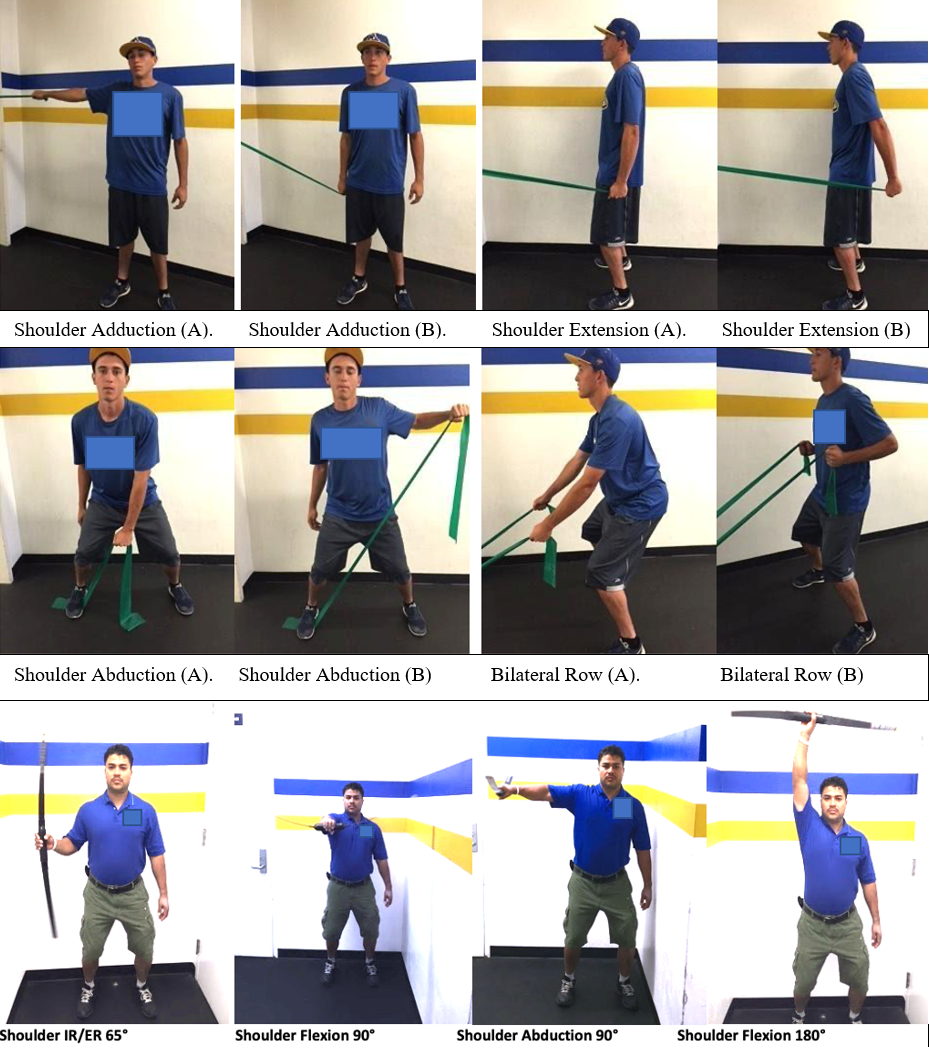
The Traditional protocol included four elastic resistance band exercises: 1) shoulder adduction, 2) shoulder extension, 3) shoulder abduction and 4) bilateral row (Figure 1). Based on prior research by Kibler et al.,24 expectations were that the serratus anterior (SA) and lower trapezius (LT) would be activated between 15% and 30% in all four exercises and the upper trapezius (UT) activation between 21% and 36% in the dynamic exercises (Shoulder Abduction and Bilateral Row). The anterior deltoid (AD), and posterior deltoid (PD), which act as both mobilizers and stabilizers would also be expected to be moderately active.20 The moderate activation levels found in these exercises are consistent with physiologic activation sequences and restoration of shoulder function and are effective for asymptomatic and symptomatic populations.19–21,24 This protocol followed strengthening exercise guidelines that limit atrophy and allow for pain-free movement.29
_and_bodyblade_trade__exercises_(.png)
The Traditional group trained three sessions per week (Table 2). The guidelines followed were based on the Essentials of Strength and Conditioning textbook.30 Supervising athletic trainers documented progression using the Traditional Elastic Resistance Checklist.
The Bodyblade™ exercise protocol consisted of shoulder internal and external rotation (IR/ER) at 65° (transverse plane: longitudinal axis), shoulder flexion at 90° (sagittal plane: mediolateral axis), shoulder abduction at 90° (frontal plane: anteroposterior axis), and shoulder flexion at 180° (sagittal plane: mediolateral axis) (Figure 1). The exercises and the modified progression were based on prior studies.18–26 Supervising athletic trainers provided participants with a demonstration of Bodyblade™ exercise protocols using verbal and tactile cues to maintain a neutral pelvis, athletic position, and shoulder retraction throughout the selected exercises. Participants practiced with the selected tool until the principal investigator felt confident that the participant was proficient. Supervising athletic trainers continued to provide feedback to participants as instructed at the start of the study. The Bodyblade™ exercises were proposed to challenge scapulothoracic musculature at various planes of movement and promote joint stability.19–22,24–26 Prior research indicated moderate muscle activation (≥20%MVIC) of the UT, LT, and GM for all four exercises.21 The Bodyblade™ (polycarbonate flexible oscillating blade with a handgrip in the center) intervention started with participants using the Classic model (0.68 kg and 122 cm) for the first four weeks. Three sessions per week were performed to maintain consistency throughout each group. On week 1, sessions started at 30-seconds and progressed weekly in 10-second increments to 60 seconds. At weeks 5–8, participants transitioned to the Pro model (1.13 kg and 152.4 cm). The rest between each set equaled the time spent performing the exercise (30-60-seconds, 1:1 work to rest ratio) to minimize the effects of fatigue27 (Table 3). The supervising athletic trainers documented progression using the Bodyblade™ Checklist.
The Mixed exercise protocol group utilized both Traditional and Bodyblade™ exercise protocols (Table 4). The protocol alternated weekly starting with the Traditional on odd-numbered weeks and continuing with the Bodyblade™ on even-numbered weeks. The Mixed group’s progression allowed the participants to only advance to the halfway point from each protocol (Table 4). The supervising athletic trainers documented progression using the Mixed Checklist.
Supervising Athletic Trainer Participation
There were six supervising athletic trainers from five colleges that participated in the study (31-51 yrs., all master’s degrees with 8-27 yrs. of experience). Supervising athletic trainers-initiated participation in the study by submitting a letter of support and completing research training. Research efforts began by identifying potential participants in the respective athletic programs. The principal investigator provided supervising athletic trainers and participants with a brief demonstration of exercise protocols using verbal and tactile cues to maintain pelvic neutral, athletic position, and shoulder retraction throughout the selected exercises. Participants practiced with the selected tool until the principal investigator felt confident that the participant was proficient. Throughout the intervention, supervising athletic trainers continued to provide feedback to participants as instructed at the start of the study. There was a 30-60 second rest between sets and exercise tools to minimize the effects of fatigue.27 Exercise log checklists were submitted to the principal investigator via electronic mail or fax no later than Friday of each week. Any questions, concerns, or data collection issues that arose supervising athletic trainers immediately contacted the principal investigator.
Measurements
Researchers performing the testing were blinded to the group allocation. Demographic information was obtained before taking baseline measures (age, sex, sport, and arm dominance) followed by anthropometric measures (height, weight, and upper limb length). Arm dominance was determined as the arm used to throw a ball. The measurement of upper limb length was taken by instructing the participant to stand with their back against a wall, feet together, shoulders and arms in 90° abduction, and back of hand flat against the wall: this position limited trunk movement and scapular tilting. A cloth tape measure was used to determine arm length by placing the stationary end of the tape on the spinous process of the 7th cervical vertebrae and the loose end at the tip of the hand’s middle finger.
The WOSI (web-based) 21 item questionnaire evaluates outcomes occurring after interventions for patients with shoulder instability.31 WOSI consists of four domains; a) physical symptoms (10 items), b) sport/recreation/work function (4 items), c) lifestyle function (4 items), and d) emotional function (3 items). Participants used a visual analog scale that ranged from no complaints (0) to severe complaints (100). The WOSI was conducted before the start of the intervention, during the 4th week, after the intervention (8th week), and at the three-month follow-up. The total score from the four domains and each domain individually were used to perform statistical analyses.
Following WOSI, the UQYBT, (Move2Perform, Evansville, IN) was conducted. The UQYBT was developed to identify upper extremity and trunk mobility in the reaching limb’s open kinetic chain as well as midrange limitations, asymmetries, core stability in the closed kinetic chain on the stabilizing limb.32 To complete the analysis, each direction’s maximum score was extracted to represent the end range of the athlete’s performance. The average maximum reach from the three directions was calculated to record a composite score for each participant. The assessment progresses in the following order: a) medial, b) inferolateral and c) superolateral directions. Before official testing, participants watched an instructional video entitled “Y Balance Test Upper Quarter – Client Instruction”. Once participants watched the video, they removed their shoes and began warming up by reaching in all three directions two times on each arm. After warming up, participants began three official trials. The trials were acceptable if they maintained the following criteria: 1) three points of contact to the floor with involved arm and feet, 2) participant did not use momentum to move the reach box (i.e., push the box), 3) participant did not let the reaching hand touch the ground during the trial, 4) participant did not use the top of the reach box or testing equipment to help stabilize their body. Participants did not experience any pain or discomfort during trials that would inhibit any further testing.
The three reach directions were named based on the arm placed on base during the trial. For example, the right-handed stance was labeled; (right) medial, (right) inferolateral, and (right) superolateral and the left-handed stance followed the same procedure (left) medial, (left) inferolateral, and (left) superolateral. Each trial was performed without stopping between the three reach directions. Subsequently, participants returned to their starting position after each reach direction in a controlled manner. The principal investigator recorded the greatest distance from each direction and averaged those numbers to attain a composite score.29 Measures were taken before the intervention (pre-test), at the 4th week (mid-test), at the conclusion of the 8th week (post-test), and at the three-month follow-up.
Statistical Analysis
Descriptive statistics included means and standard deviations for all tests and measures. Kolmogorov–Smirnov tests of normality were conducted for all dependent variables. Significance was defined as p<0.05. If the assumption of sphericity was violated, the Greenhouse−Geiser correction was employed. A mixed model, repeated measures 4x3 ANOVA design was used to evaluate UQYBT and WOSI score differences within tests (pre-test, mid-test, post-test, and three-month follow-up), and between groups (Traditional, Bodyblade™, and Mixed) interactions (SPSS Version 20.0). The modified Bonferroni post-hoc analysis controlled for Type 1 error rate across multiple comparisons and was used to find significant differences between and within groups. Eta-squared (eta2) was utilized as a measure of effect size with ratios interpreted as 0.01: small, 0.06: medium, and >0.14: large magnitude. Cronbach alpha intraclass correlation coefficients (ICCs) were measured for the pre-test trials of each condition to assess consistency of these data. Based on Koo and Li,33 ICC between 0.75 – 0.9 were classified as good, and over 0.9 was considered excellent.
RESULTS
There was nearly full (97.3%) participation and adherence throughout the study, except for one participant in the Mixed group who could not complete the three-month follow-up on the UQYBT due to surgery on the involved shoulder. Demographic, anthropometric characteristics and the average time since the last injury were not significantly different between groups with no initial differences during baseline measures.
Western Ontario Shoulder Index (WOSI)
Reliability (ICC) for the WOSI was classified as good (ICC: 0.85). There were no significant differences between participants and multiple comparisons composite score findings (Table 5). There were main effects for time demonstrating improvements for WOSI physical symptoms (F(3,102)=32.4, p<0.0001, eta2: 0.488), WOSI Sports, Recreation, Work (F(3,102) =16.53, p<0.0001, eta2: 0.327), WOSI Lifestyle Output (F(3,102) =10.21, p<0.0001, eta2: 0.231) and WOSI Emotion (F(3,102) =16.16, p<0.0001, eta2: 0.322). Hence, with the WOSI composite score, there was a significant, large magnitude (F(3,102) =21.61, p=0.001, eta2: 0.61) main effect for time with mid-test (4 weeks), post-test (8 weeks), and three month follow-up exceeding the baseline scores by 35.2% (p=0.01), 53.2% (p=0.004), and 43.7% (p=0.005), respectively. There were significant (p=0.001, eta2: 0.496), large magnitude, composite WOSI scores for within-participants interaction effect for the time and group. All groups (Traditional, Bodyblade™, and Mixed) improved over the three measurement points (mid-test (4 weeks), post-test (8 weeks), and three-month follow-up) exceeding baseline scores by; Traditional: 45.6% (p=0.002), 59.4% (p=0.01), and 59.7% (p=0.07), Bodyblade™: 26.6% (p<0.05), 56.5% (p=0.01), and 58.4% (p=0.01), Mixed: 35.9% (p=0.03), 43.3% (p=0.01) and 50.4% (p=0.008) respectively (Table 5). There were minimally clinically important differences between the pre-test and mid-test (4 weeks) with all three groups, as well as between the mid-test and post-test (8 weeks) for the Traditional and Bodyblade™ groups
Upper Quarter Y-Balance Test (UQYBT)
Reliability for the UQYBT was also classified as good (ICC: 0.81). The composite scores for between-participants and within-participants effects showed no significant findings (Table 5). There was a significant, large magnitude (F(3,102) =16.84, p=0.03, eta2: 0.24) main effect for time with mid-test (4 weeks), post-test (8 weeks), and three-month follow-up exceeding the baseline scores by 4.3% (p<0.05), 6.3% (p=0.03), and 5.3% (p<0.05), respectively. The inferolateral reach was the only direction with a significant, large magnitude, between-participants effect (F(3,102) =14.64, p=0.042; eta2: 0.17). Additionally, the Bodyblade™ group exceeded (p=0.038) the Mixed group at post-test (8 weeks) and three-month follow-up by 10.7% and 24.5% (Table 5). There were minimally clinically important differences with the composite scores between the pre-test and mid-test (4 weeks) with the mixed group, as well as between the post-test (8 weeks) and three-month follow up for the Bodyblade™ and mixed groups. With the inferolateral scores, minimally clinically important differences were detected between the pre-test and mid-test (4 weeks) with the Bodyblade™ group and between the post-test (8 weeks) and three-month follow up for the Bodyblade™ and mixed groups.
DISCUSSION
A major finding in this study was that all three training groups demonstrated significant improvements over time in the WOSI composite scores. However, there was no significant difference between any of the groups. The UQYBT demonstrated improvement only during the inferolateral reach at post-test (8 weeks) and three-month follow-up. The Bodyblade™ and Traditional groups outperformed the Mixed group, with the Mixed group demonstrating decreased UQYBT performance towards the latter duration of the study.
The WOSI (scores range from no complaints: 0, to severe complaints:100) demonstrated significant improvements in the composite scores (physical symptoms (10 items), sport/recreation/work functions (4 items), lifestyle functions (4 items), and emotional functions (3 items)) during all the three testing periods for all groups (Table 5). The current study reported reliability as excellent (ICC: 0.85), which is consistent with previous reports of ICC 0.88-0.92.31 The eight-week intervention performed three times a week provided consistent supervision, design, and compliance amongst participants for all three treatment groups and these factors may have contributed to the significant findings in the WOSI. The present findings are contrary to Eshoj et al.34 who reported no significant differences when comparing 12-week treatment protocols for shoulder instability utilizing a self-managed at-home exercise protocol versus a physical therapist-led semi-supervised exercise protocol. Although both at-home and semi-supervised exercise attempted to provide their participants with sound training progression throughout the protocols, there were major differences in the design of protocols which varied in sets, repetitions, and types of exercises. At-home exercise used general strengthening exercises compared to semi-supervised exercise that used more shoulder instability-specific exercises. Supervision for at-home exercise was limited to only the initial physical therapy session and the remaining sessions were self-reported. Alternatively, the semi-supervised group received supervised sessions twice a week for the first two weeks and then once a week for the remaining 10 weeks. Compliance for both at-home and semi-supervised exercise was set at 66%.
Kirkley et al.12 compared participants that received shoulder surgery for instability to those that chose conservative management and found that at the 32-month follow-up period, the surgical group had 16% (p=0.03) greater improvement than the conservative group. At the 72-month follow-up, the surgical group did not change in score. However, the conservative group reduced the difference to 11% (p=0.17). These delayed improvements at the 32- and 72-month periods may have influenced this tool’s utility. Earlier and more frequent testing may have better illustrated potential differences.
The Bodyblade™ group demonstrated significant improvements in the UQYBT during the inferolateral reach, outperforming the Mixed group at post-test (8 weeks) and three-month follow-up. This finding could have been due to the Mixed group only performing 50% of the Traditional and Bodyblade™ protocols. The Mixed group did not progress beyond the green resistance band or get to advance to the Bodyblade™ pro model. Hence, the progressive training stimulus did not reach the intensity of the Bodyblade™ or the Traditional training protocols and thus may have been insufficient. Previous UQYBT studies only used healthy participants to help establish reliability and sex differences in performance.32 No participants in previous studies exhibited pre-existing shoulder instability conditions. Nonetheless, the UQYBT foundational studies provide insight into how normal values can be utilized to determine performance without an intervention.32,35,36 Furthermore, previous UQYBT studies to date suggests the need to develop rehabilitation protocols for those with shoulder instability and continue to expand the knowledge into different types of athletes to increase normative data and allow to screen for those at risk of injury.32,35,36
The utilization of the Bodyblade - Classic and Pro models used in this study are in accord with UQYBT authors’ recommendations in developing rehabilitation protocols for TASI. All four Bodyblade™ exercises used in this study have been shown to elicit moderate to moderately strong muscle activation levels between 20% - 46% MVIC of the infraspinatus, upper trapezius, lower trapezius, and gluteus maximus.21,37 These levels are considered to be effective for moderate muscle strengthening.21 Furthermore, Escamilla et al.37 utilized the Bodyblade™ Classic (0.68 kg, 119.38 cm) and Pro (1.13 kg, 152.4 cm) in two of the four exercises used in this study. However, Oliver et al.21 utilized the Bodyblade™ CxT model (0.68 kg, 102 cm), which weighs less than the Pro and is shorter in length compared to the Classic and Pro models. These factors may have to be further explored to determine their effect on muscle activation levels. Nevertheless, the whole-body kinetic-chain patterns found by Oliver et al.21 are favorable for rehabilitation and could explain why the Bodyblade™ group was the only group to obtain significant findings during the inferolateral reach direction.
The inferolateral reach demands its participants to maintain a prone three-point stance position while supporting themselves on the involved arm. The arm must maintain a stationary position of approximately 90° of shoulder flexion. Basset et al.38 reported that the pectoralis major, the short head of the biceps brachii, coracobrachialis, anterior deltoid, and subscapularis were the primary restraints in anterior shoulder instability when the shoulder is in a flexed position. Furthermore, Kronberg et al.39 identified decreased muscle activity of the anterior deltoid, subscapularis, pectoralis major, latissimus dorsi, and serratus anterior in participants with shoulder instability. Thus, Parry et al.19 in examining the utilization of the Bodyblade™ Pro in shoulder flexion reported the anterior deltoid, serratus anterior, and pectoralis major and infraspinatus all elicited 50% MVIC, which may have been the reason for the greater improvement in the UQYBT inferolateral reach direction.
It can only be speculated that the improved Bodyblade™ group performance during the UQYBT inferolateral direction resulted from greater muscle activation based on previous studies. The interventions performed in this study required participants to perform the exercises while in an athletic stance position. However, the UQYBT is performed in a prone three-point stance. The transferability of the interventions onto the UQYBT reach directions may have affected the potential for significant outcomes. There could have been different outcomes if the interventions were also performed prone similarly to the demands of the UQYBT. Behm & Sale28 suggested that task-specific resistance training will exhibit optimal gains with a similar testing training method. In accordance with the SAID (Specific Adaptation to Imposed Demands) principle, when training methods deviate from testing measures, there will be decreased improvements.
However, it is unknown whether the benefits of the Bodyblade and Traditional groups were from strength gains or motor control, or possibly a combination of both. The timing of muscle activation (motor control) is an important component of neuromuscular efficiency, which can be affected by shoulder conditions compared to healthy patients.40 The late improvements during the eight-week intervention allow clinicians to understand the delayed benefits of using the Bodyblade™ and help educate patients on its utility. These findings are further supported by the Sugimoto & Blanpied25 study that found participants reported the Bodyblade™ more challenging at the start of the 5th week of intervention. Additionally, these findings could lend further credibility to the role of the Bodyblade as an early to intermediate phase rehabilitation tool.
Limitations
The study participants were cleared by an orthopedic surgeon during pre-participation physical examinations and satisfied the inclusion criteria based on the shoulder history questionnaire. However, the severity of shoulder instability was unknown amongst each participant. Participants may have had pre-existing conditions that could have contributed to decreased performance. Only through diagnostic imaging would the participant’s level of shoulder instability be fully determined. Nonetheless, if this component would have been added to the study, it may have presented several challenges with the imaging findings and their clinical relevance. This challenge could have potentially reduced the number of participants included in the study if the structural abnormalities exceeded the orthopedic recommendations for conservative management. These potential factors were carefully considered during the development of the inclusion, exclusion criteria, and assessment strategies. Based on the limited resources available for this study, a practical training and testing approach was taken. Future research on the Bodyblade™ to manage TASI may perform manual orthopedic assessments, instead of imaging to confirm anterior shoulder instability.
CONCLUSIONS
The main significant findings were demonstrated in the Bodyblade™ group during the UQYBT inferolateral reach at the post-test (8 weeks) and at the three-month follow-up. Conversely, the Mixed group had deleterious effects during the post-test and three-month follow-up. This could have been due to the Mixed group performing only 50% of the Traditional and Bodyblade™ protocols, preventing participants from obtaining high enough stimulus for positive benefits.
The stepwise progressions discovered in each of the three groups during the WOSI measurement points allow clinicians to provide their patients with the option of choosing the Traditional or the Bodyblade™ protocols. However, choosing the Mixed protocol has no additional benefit and may decrease performance based on the UQYBT post-test and three-month follow-up findings. Finally, it is not recommended to use the WOSI as a standalone outcome measure for shoulder instability rehabilitation. The WOSI should be accompanied by a functional outcome measure such as the UQYBT to make a sound clinical decision.
Conflict of Interest
The authors declare no conflicts of interest with the contents of this manuscript.