_depending_on_test_category_(x-axis).tif)
Introduction
The risk of sustaining a serious acute knee injury, especially injury to the anterior cruciate ligament (ACL), is elevated in ball and racket sports that involve abrupt changes of direction (i.e. landing, turning, and sidecutting).1–4 The incidence rate may be as high as 2.0 per 10,000 exposures in female football5 and 3.1 per 10,000 player hours in female handball.6 However, when looking at incidence rate during game play incidence rate rises to 16 ACL injuries per 10,000 hours in female handball.6 The individual long term consequences may be substantial, as the knee injury may increase the risk of early osteoarthritis7 and reduce the quality of life.8
Many studies examining anatomical, physiological, biomechanical and neuromuscular risk factors have been carried out to investigate various mechanisms potentially influencing injury risk.9–13 It is shown in a case study that an ACL injury may occur after landing with little knee flexion and displaying rapid changes of knee abduction and knee rotation angles during the very early phase (<40 ms) after initial contact, thus emphasizing the importance of proper knee joint stability at landing.14 Also, anatomical studies show that quadriceps muscle contraction forces, as observed during the initial landing phase, may result in an anterior translation of tibia, thus increasing strain in the ACL.15–17 These tranaslational forces would best be counteracted by the hamstring muscles,18–20 and prospective studies have also shown that reduced medial hamstring activity at initial contact during a sidecutting maneuver significantly increased the risk of ACL injury.12,13 Exercises for increasing the medial hamstring activity may be especially important for females, as studies have shown less medial hamstring activity in female athletes during sidestep cutting.21
Although multi-exercise prophylactic training, including exercises on different balance devices, is estimated to be able to reduce the risk of ACL injury by 50% or more,22 few studies have examined the effect of such training regimes on the hamstring activation level during ACL injury risk movements. Zebis et al.23 found increased hamstring preactivation during sidestep cutting after a prevention training program24 which consisted of both standing and landing balance exercises on floor and unstable surfaces. To understand which exercises may be the most effective in increasing hamstring activation levels during risk movements like sidestep cutting, greater knowledge about the muscular activation, e.g. hamstring muscle activity, during the different specific exercises may be helpful. Further, such information may assist in planning the optimal progression and designing the most efficient prevention program or rehabilitation program.
Previously, studies investigating lower leg muscle activity during balance exercises showed gradually increased activation of the ankle joint stabilizing muscles when moving from standing balance on the floor to balancing on an Airex® mat and BOSU-ball®, respectively.25 Few studies have investigated if these increased activity patterns are also true for the knee joint muscles during such balance exercises. Thus, performing exercises that facilitate enhanced hamstring activity – and knowing how to progress them – may be a promising approach both in prevention and clinical rehabilitation, when aiming to enhance knee joint stability during vigorous movements seen in many ball and racket sports.
Therefore, the purpose of the present study was: Firstly, to investigate how knee muscle activation levels and knee and hip joint kinematics were influenced by exercises with increasing levels of postural control demands, progressed as either increasing the instability of the surface and/or increasing the demands of the balance task from standing exercises to landing exercises. Secondly, post-hoc analyses were made for analyzing possible effects of sex on muscle activation patterns and knee and hip joint kinematics within the different exercise modalities and balance devices.
Methods
Study design
The study used an exploratory, cross-sectional design in which a cohort of 20 healthy subjects (11 males) were examined for sagittal plane hip and knee kinematics and muscle activation while performing different exercises challenging postural stability with increasing difficulty in a 3-dimensional (3D) movement analysis laboratory. There was no pre-defined weighting of study outcomes or outcome hierarchy, but given the described potential importance of the hamstring muscles as knee joint stabilizers, particular the medial hamstrings,12,13,21 the primary focus was on identifying exercises with high medial hamstring activation. Data for ankle muscle activity and ankle kinematics during balance exercises in the same cohort have been reported previously.25
Subjects
A convenience sample of twenty healthy subjects, 11 male and nine females, volunteered to participate in the study. Mean age (± SD) was 28.8 ± 2.3 yrs, mean weight was 71.9 ± 11.5 mean height 177 ± 11 cm. All the participants were active in different sports, on average 5.2 ± 3.0 hours per week (range 1-13.5 hours per week). Subjects were excluded if they had any history of an injury in the lower extremity in the preceding six months. An injury was defined as an injury occurring during a scheduled game or practice, causing the player to miss the next game, practice session or to participate with considerable discomfort. Furthermore, subjects were excluded if they had performed any specific proprioceptive training during the same period or had performed any strength training sessions within a period of 48 hours before testing. None of the subjects reported any history of neurological or vestibular impairments. The local ethics committee did not need to perform a full ethics review, because the exercises were all commonly used in standard training programs and the non-invasive character of the experimental procedures, and furthermore only healthy participants were included. All participants gave their informed consent, according to the Helsinki Declaration, before entering the study.
Test protocol
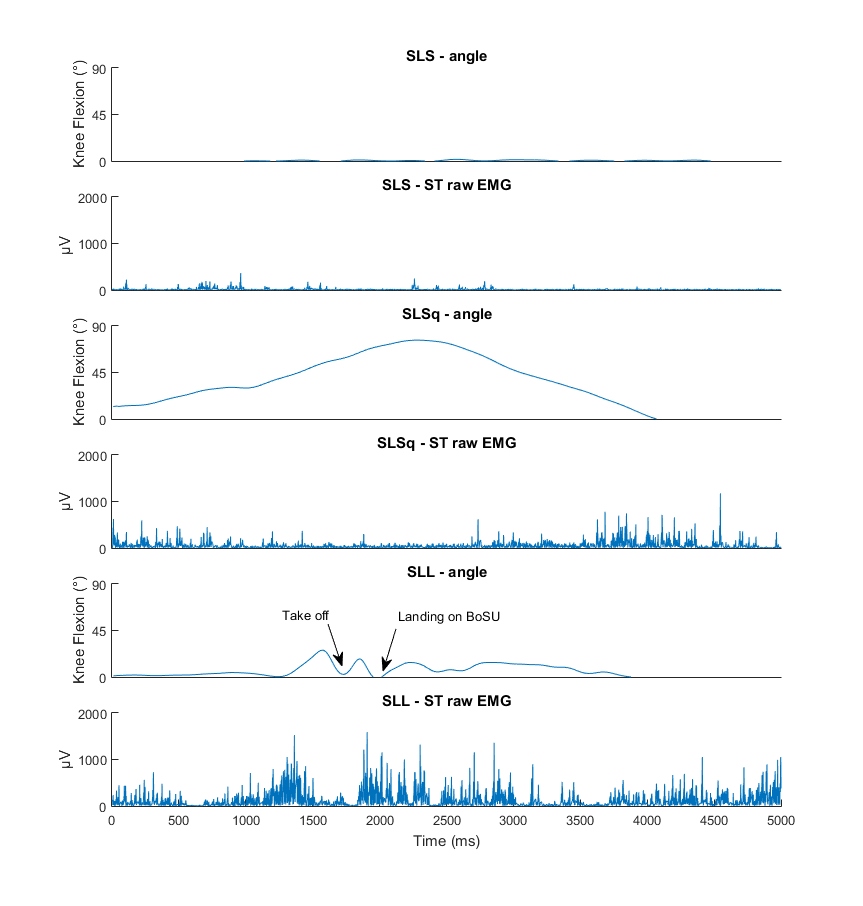
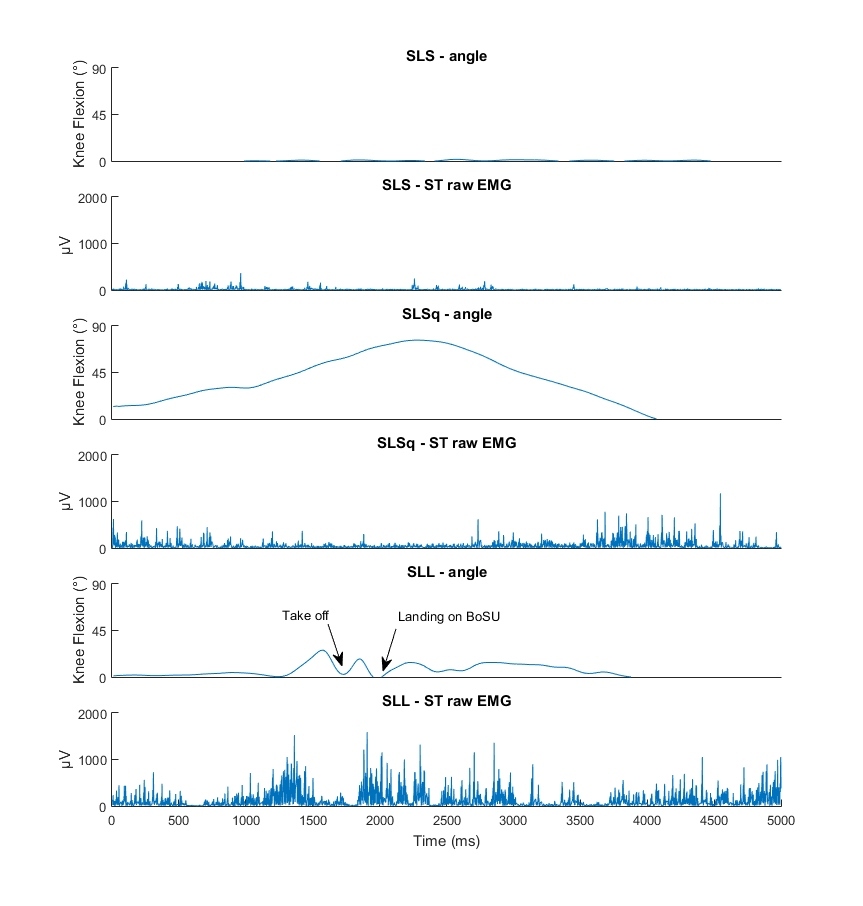
The test session comprised three types of exercises commonly used in prevention programs or rehabilitation regimes: 1) single-legged standing balance, 2) single-legged squatting, and 3) single-legged landings. The single-leg stance exercise demanded 15 seconds of quiet standing balance, while the single-leg squat test was a starting from straight leg position performing a single knee flexion to approximately 90 degrees followed by full extension, in a 2-second up and 2-second down steady rhythm. The single-leg landing tests were performed as one-legged hop from a distance of 80 % of the subject’s leg length, and the subject was required to maintain balance after landing for five seconds.
Each exercise was performed on three different surfaces of varying degrees of instability, one stable and two unstable, in this way a total of nine different tests were performed. The stable reference surface was solid floor, and the two unstable balance devices were a foam pad (Airex-mat®, Sins, CH) and the convex side of a BOSU-ball® (OH, USA), henceforth called Airex and BOSU, respectively. Both balance devices are commonly used in rehabilitation or injury prevention training programs.24,26,27
The BOSU exercises were considered to challenge the postural balance more than the Airex. Subjects were instructed to maintain balance as steady as possible with no restrictions or instructions on leg and arm positioning. Subjects were permitted three familiarization trials before single-leg landing and one to two familiarization trials before single-leg squat and single-leg stance tests. Three trials were collected for each test and used for analysis. The test protocol ensured that all exercises were performed in a randomized order with a 30 second rest between trials and two minutes rest between different tests to avoid muscle-fatigue and maintain a high level of focus. A trial was discarded if the subject could not stand for 15 seconds during the single-leg stance test, lost balance during the squatting movement, or could not maintain balance during the first five seconds after landing in single-leg landing. Lost balance was defined as the subject requiring any correction such as re-positioning their foot or touching the floor/balance device with the opposite foot during the test.
Kinematic data
Kinematic differences in knee and hip joint angles between exercises and balance devices were determined using 3D motion analysis (Vicon 612 Vcam motion capture system, Vicon Motion Systems., Oxford, UK). Before testing, sixteen reflective markers were placed over anatomical landmarks according to a modified Helen Hayes marker setup,28 except for the thigh markers, which were substituted by markers attached over the patella, to reduce soft tissue artefacts.29 Knee and hip joint angles were calculated using inherent Vicon plug-in-gait software, including Woltring cubic spline filtering of marker trajectories. The tests were performed with the balance devices placed on a force platform (AMTI OR6-7, MA, USA). The single-leg stance test was a static standing exercise, therefore mean hip and knee flexion angles during the duration of the test were obtained for comparison with the two dynamic exercises. Hip and knee flexion angles were obtained for both the initiation of the movement and the maximal hip and knee flexion angles displayed during the single-leg squat and single-leg landing, respectively. The initiation of the movement was defined as the start of the downwards movement during the single-leg squat and the time of initial contact during the single-leg landing, recorded as the instant the vertical ground reaction force exceeded 20 N.
EMG Data
Electromyographic (EMG) recordings were used to measure the activity of the muscles controlling the knee joint during all tests. EMG signals were recorded using rectangular (20 mm x 30 mm) bipolar surface electrodes (DE-2.1, Delsys, Boston, MA, USA). The electrodes were attached to the quadriceps muscle over two vastii, the vastus medialis (VM) and the vastus lateralis (VL), the hamstrings, the semitendinosus (ST) and the biceps femoris (BF) according to standard guidelines.30 All electrodes were placed on the dominant leg determined as the preferred kicking leg. Skin surfaces were shaved, abraded, and cleansed with alcohol to improve the conductivity of the EMG signal.21 All EMG signals were pre-amplified and sampled with a frequency of 1000Hz by a device (Myomonitor IV, Delsys, Boston, MA, USA) carried on the back of the subject. Data was wirelessly transmitted to a computer with a fixed delay of 200 ms and recorded synchronously with the kinematic recordings by inherent software in the Motion Analysis system (Vicon 612 Workstation, Vicon Motion Systems, Oxford, England). Prior to dynamic exercises, three trials with five seconds of maximum voluntary contractions (MVC) were performed to obtain maximal EMG-levels for each muscle. The maximal activation of the quadriceps muscle was obtained in a sitting position with 60° of knee flexion, and the hamstring maximal activation levels were obtained during prone lying with neutral hip and 20 degrees of knee flexion.
The fixed transmission delay was adjusted to have the EMG data synchronized with the kinematic data. The raw EMG-signals were filtered first using a fourth-order high-pass filter with a cutoff at 10 Hz, and subsequently filtered using a root-mean square (RMS) sliding windows of 30 ms with 29 ms overlap. Similar filtering procedures were applied to the MVC-trials over the five second period. Peak values from each muscle during the MVC-trials were used for normalization of EMG data during the exercise trials.
To compare the level of muscle activity between three dynamically different exercises the peak amplitude obtained during the trial was chosen as primary output parameter. During the single-leg stance test, only the mid-10 seconds of the 15 second trial were used to exclude postural adjustments at the beginning and to avoid muscle-fatigue at the end of the balance trial.31 For the single-leg squat the peak amplitude in the period from the beginning of the descending motion to the end of the ascending motion was obtained. During single-leg landing, the peak amplitude recorded from 100 ms before landing to one second after landing was obtained.
Statistical methods
Because this study used an exploratory design, no a priori sample size estimation was performed.
Peak normalized EMG amplitudes for the four muscles and joint angles of the hip and knee joints were averaged across the three trials for each of the test conditions. A mixed-design ANOVA was applied for the data defining test modalities (single-leg stance, single-leg squat and single-leg landing tests) and balance devices (floor, Airex and BOSU) as within-subjects random effects factors, and sex was defined as between-subjects fixed effects factor. The level of significance was set at p < 0.05, and partial Eta squared (η2) was used as effect size estimate. If significant differences were found in muscle activation levels across exercises and/or levels of balance stability, a Bonferroni adjusted post-hoc analysis of differences between each condition was performed. The statistical analyses were performed in SPSS version 22.0.0.
Results
Kinematic data
Knee flexion and hip flexion at initiation of the exercise varied significantly between the different exercises showing a larger degree of flexion with increased dynamic intensity of the task (knee: F(2,36)=12.39, p<0.001, η2=0.41; hip: F(2,36)=111.60, p<0.001, η2=0.86). Likewise, the maximal knee and hip flexion angle were affected by the specific exercise performed (knee: F(2,36)=577.71, p<0.001, η2=0.97; hip: F(2,36)=228.62, p<0.001, η2=0.93) showing a larger degree of flexion during the single-leg squat exercise compared to both single-leg standing (knee: p<0.001, η2=0.98; hip: p<0.001, η2=0.95) and single-leg landing (knee: hip: p<0.001, η2=0.96; hip: p<0.001, η2=0.72).
The choice of balance device also significantly affected kinematics. The knee and hip flexion at initiation of the task increased with the increased postural challenge induced by the balance device with the floor offering the least challenge and the BOSU inducing the most postural challenge (knee: F(2,36)=52.22, p<0.001, η2=0.74; hip: F(2,36)=37.40, p<0.001, η2=0.68). The maximal knee flexion was not affected by the choice of balance device, but the maximal hip flexion increased with increased postural challenge (knee: F(2,36)=4.48, p=0.018, η2=0.20; hip: F(2,36)=11.38, p<0.001, η2=0.39).
Overall, female subjects displayed across all tests less maximal joint angle flexion compared with male subjects (Table 1) and a tendency to have less flexion at the initiation of the exercise. However, no significant difference between sexes was found in the change in kinematics with between balance devices or between exercises (p>0.05 for all kinematic parameters).
Muscle activity - Between exercises
In general, the hamstring activity increased significantly with each level of test modality, from very low peak activity during single-leg stance to medium activity during single-leg squat (ST: F(1,18)=14.106, p<0.001, η2=0.44; BF: F(1,18)=34.108, p<0.001, η2=0.66), and from medium activity during single-leg squat to highest activity during single-leg landing activities (ST: F(1,18)=64.040, p<0.001, η2=0.78; BF: F(1,18)=42.744, p<0.001, η2=0.70) (Figures 1 and 2, and Tables 2-3).
The quadriceps activity was very low during the single-leg stance exercises, but increased four-fold during the single-leg squat (VM: F(1,18)=83.103, p<0.001, η2=0.82; VL: F(1,18)=151.515, p<0.001, η2=0.89). No difference in activity levels of either VM or VL was seen when performing single-leg landing exercises compared to single-leg squat (F(1,18)< 2.8) (Tables 4 and 5).
Muscle activity - Between balance devices
When comparing the different balance devices across exercise modalities, the BOSU induced significantly higher hamstring activity levels than the Airex (ST: F(1,18)=24.216 , p<0.001, η2=0.57; BF: F(1,18)=25.245, p<0.001, η2=0.58). No difference in hamstring activity was found between exercises on the floor and on an Airex (F(1,18)<0.5) (see tables 2-3). Also for the two quadriceps vastii, there was no difference between exercises on the floor and on the Airex (F(1,18)<1.9), but the VL-activity increased significantly when exercising on the BOSU (F(1,18)=6.993,p=0.016, η2=0.28). The increase in activity of VM from Airex to BOSU was minor and non-significant (F(1,18)=3.828, p=0.066, η2=0.18) (Tables 4 and 5).
Muscle activity - Between sexes
No overall differences in muscle activity across all test modalities and devices were found between sexes, however when including sex as a between-subjects effect, small but significant differences in activity level changes from single-leg squat to single-leg landing were observed for the medial hamstring. The increase in ST activity across all devices when changing from single-leg squat to single-leg landing was larger for the female participants than for the males reaching a higher level of activity (F(1,18)=4.335, p=0.038, η2=0.19) (Figure 2). This sex-specific increase in activity was most apparent for exercises on the BOSU (Figure 2). No changes were observed for the other muscles as an effect of sex.
_depending_on_test_category_(x-axis).tif)
Discussion
The main results of the present study were that the more challenging, i.e. unstable, the balance devices were, the higher the hamstring muscle activity levels, with a clear progression from standing balance exercises to standing dynamic exercises to dynamic landing exercises. Thus, dynamic exercises on an unstable surface are superior to static exercises in terms of increased hamstring activation. Interestingly, the data furthermore indicate that this increase in hamstring activation is especially pronounced in female athletes when progressing from single-leg squat to single-leg landing exercises (Figure 2).
As mentioned earlier, a high level of muscle activity around the knee joint, including high activity of especially the medial hamstrings, seems important for prevention of ACL injuries.12,13,18–21 Therefore, specific attention was given to how different exercises with three levels of progression would affect hamstring activation levels.
The present data show little activity in any of the examined muscles during the single-leg stance exercise. This corresponds to other studies also showing low levels of activity in the thigh muscles during standing balance exercises.32,33 Considering the lack of loaded movement around the hip and knee joint this may not be surprising, however increasing the demand on postural control may also induce an increase in the degrees of hip and knee flexion significantly for the most challenging device, i.e. the BOSU as a compensation for the reduced ability of the ankle to control postural stability. These changes in the need for stabilisation and slight increase in hip and knee joint flexion increase the external moment, and as such place more demand on force production in the knee and hip extensors, thereby explaining the small, yet significantly increased levels of muscle activation in the hamstrings and quadriceps during single-leg stance on the BOSU. Furthermore, no difference in thigh muscle activation was observed during standing balance, between the firm floor surface and the less stable Airex. It should be noted that the present study was conducted with healthy subjects and that standing on an Airex may possibly be more challenging and induce greater muscle activation with subjects in the early phase of rehabilitation after an ACL injury.
Performance of single-legged squats are extensively investigated as an exercise for knee injury prevention or rehabilitation exercise.32,34–39 The present data corroborate previous studies in showing highly increased levels of quadriceps activity for all balance devices, compared to single-leg stance, but a more moderate increase in mean peak hamstring activity. Although the increase in hamstring activity relative to single-leg stance was significant for the Airex and the floor, single-leg squat on BOSU still required larger levels of hamstring activation compared to the less demanding devices. None of the tested devices, however, produced hamstring activation above 40% during single-leg squat. This emphasises, as also shown by other studies, that the single-leg squat may not be optimal if the purpose is to induce high levels of hamstring activation in co-contraction with quadriceps activation.32,35,39 This may be an important consideration when designing prevention programs or rehabilitation programs after ACL-reconstruction. In contrast, during the dynamic landing exercises much higher levels of activity in both hamstring and knee extensor muscles were present around the time of initial contact, regardless of the type of landing surface. No studies have compared the activity levels of dynamic landings to standing balance exercises, but studies on landing show peak values of knee muscle activity very similar to the present study.40–42 Although muscular activity levels above 40-60% are considered necessary for inducing strength gain,43 the high activation levels of the hamstrings during dynamic single-leg landing exercises may not be in increasing hamstring strength, due to the short duration of the activity bursts. However, optimizing the neuromuscular coordination in terms of increasing medial hamstring activation during injury risk situations, like side-cutting, has also been shown to be important.12,13 Studies on motor learning have shown that a consistent perturbation of the muscle synergies involved in an existing motor program, e.g. the motor program used during landing, may be the fastest way to make consistent changes in a motor program.44 It is therefore likely that the increased hamstring activity observed in the single-leg landing exercises may indicate that single-leg landing is more efficient in altering the motor programs during landing or cutting movements and as such suggest that dynamic landing exercises may be more suitable for injury prevention programs and probably also late phase rehabilitation after ACL-reconstruction. The importance of dynamic exercises for improving joint control is also highlighted in a review of effectiveness of ankle stability exercises, which concluded that dynamic landing exercises were particular beneficial for increasing the anticipatory adjustments stabilising the ankle joint.45 And also, addressing knee joint stability, a recent meta-analysis showing that prevention programs consisting of balance exercises alone were less successful in ACL injury prevention compared to programs consisting of a variety of dynamic exercises, and this effect may be partly due to a more effective alteration of hamstring activation after dynamic exercises.46 The results of the present study also showed that the dynamic landing exercises investigated increased the medial hamstring activation more in female subjects than male subjects, indicating that such exercises might be even more beneficial for female athletes (Figure 2). The results further suggest that exercises on the BOSU device may potentially be most effective.
When designing injury prevention or rehabilitation programs, different training devices designed to challenge a subject’s balance may be selected. Information about the effect of the different devices may be very useful to guide an optimal training progression, and the results of the present study may offer such guidance. Some care should be taken in the interpretation of the results, as the number of subjects was low. Furthermore, subjects in this study were healthy persons without previous injuries affecting their performance, and some of the tests may be too challenging early in ACL rehabilitation. Also, when designing injury prevention programs, these results may help in selecting exercises, however the subjects were a randomly selected group of physically active young, adult subjects, and the neuromuscular response to the selected exercises may be different in other populations e.g. highly trained athletes or adolescent subjects. In addition, the implementation of these results may be a challenge in some sports, as the instable surfaces may be less accessible in outdoor settings. Given these limitations, the results of the present study indicate how increasing the instability with balance devices and increasing the dynamics of the exercise may influence the neuromuscular control of the knee joint in young, physically active men and women.
Conclusion
In this explorative trial in healthy, physically active male and female subjects, the neuromuscular activity of the quadriceps and hamstrings increased when the motor task became more dynamic. Specifically jump landings were effective in increasing the hamstring muscle activity. Also increasing the instability introduced by the balance device increased muscle activity, however only when progressing from the Airex to the BOSU. The data also indicated that female subjects increase hamstring muscle activation more than males when using the most unstable balance device. This information may be useful when selecting exercises for knee injury prevention or rehabilitation.
Conflict of interest statement
The authors report no conflicts of interest.