INTRODUCTION
Low back pain (LBP) is a common complaint in the general population all over the world and often persists beyond the acute stage.1,2 It is commonly associated with sedentary occupations and lifestyles, obesity and smoking.1 Throughout the general population, research regarding epidemiology of LBP has been well established.3 Physical activity has been suggested to have a protective effect against LBP,4 and it is well documented that participation in sport has a positive effect on health in general.5 However, there is an inverse relationship between LBP risk in sedentary and in active people.6 There is an absence of information regarding the ideal dose-effect relationship of physical activity.3 Back pain is common among athletes and regularly influences sport performance and participation.3 A consensus statement published in 20217 examined the management and prevention of LBP in rowing. Their findings corroborated those in this study.
Intense physical activity may create a greater risk of LBP,6 particularly in demanding sports such as rowing.8 In New Zealand, the Accident Compensation Corporation (ACC) identifies the back/spine to be the most commonly injured area in rowing.9 The literature has covered a variety of different aspects of LBP, but its value is limited due to its heterogeneity. Epidemiological investigation has observed the widespread nature of the condition. Furthermore, various mechanical factors have been investigated to examine their impact on LBP in the rower and finally, a biopsychosocial approach to management has tentatively been explored.
A LBP definition has not been precisely determined, potentially due to a lack of definition within the literature.10 The heterogeneous data sets and wide variety of topics explored through the literature make a scoping review the best-suited study methodology to systematically map and appraise all the available literature and identify areas for further research. Therefore, the aim of this scoping review was to investigate and collate the available literature regarding LBP in rowing to inform athletes, coaches, and further research.
METHODS
The original methodological framework for scoping reviews published by Arksey and O’Malley11 and amended by Levac et al12 along with the reporting checklist developed by Tricco et al13 were utilized to synthesize relevant information available within the peer-reviewed literature. Updated guidance for scoping reviews was provided by Peters et al.14
Identification of the research question
The current scoping review was directed by using the following broad research question: What is the current peer-reviewed literature that has examined low back pain in rowing?
The objectives of the review were: (1) to complete a scoping review on the current literature available on low back pain (LBP) in rowing, (2) to investigate the breadth and depth of research regarding LBP within the rowing population, (3) to elucidate areas where research may be lacking to inform future research, and (4) to undertake a critical appraisal to assess the quality of research within a clinically or scientifically important section of the total literature reviewed.
Identification of the relevant studies
The search strategy was developed by the first author with input from a knowledge specialist, amended by the second author and applied to PubMed, ScienceDirect, and Ebsco health database (final search: 01.11.2020). Combinations of the following search terms were used on each database: “low back pain” OR “low back injury” OR “lumbar injury” AND “rowing” OR “rower”.
Study selection
Eligibility criteria were drafted prior to conducting the search, and in accordance with the process described by Arksey and O’Malley,11 any modifications required were applied throughout the progress of the review. The inclusion criteria were the following: (1) includes combinations of search terms within the title and/or abstract, (2) is on LBP in the context of the sport rowing, (3) full text available online, (4) no date restriction, (5) peer-reviewed published data. Exclusion criteria were as follows: (1) studies relating to similar water sports not specified to be rowing, (2) studies not relating to the region of the low back, and (3) grey literature.
The selection process comprised two screening levels: (1) a title/abstract/keyword review and (2) full-text review. During the initial screen, the first author reviewed titles and abstracts of the identified articles. Each citation from the electronic bibliographic database were entered into a Microsoft ® Excel (version 2002) spreadsheet, screened through the eligibility criteria and then concluded to be either included or excluded. Throughout this initial level of screening, it was clear that the search terms were not broad enough and were expanded from “low back pain” to include “low back injury” and “lumbar injury”.
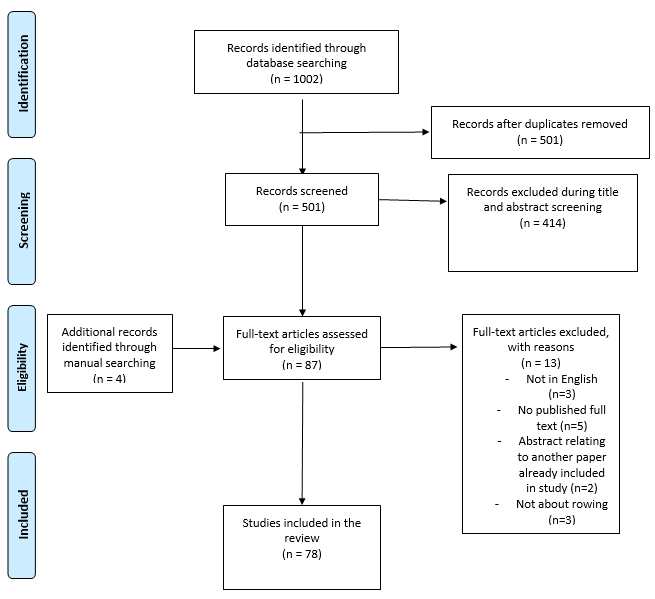
During the second level of review, the full texts of studies were reviewed by the first author to establish their eligibility. Additionally, reference lists of included studies were searched manually to identify further pertinent studies (Figure 1). Each study picked up during the full-text review to meet the inclusion criteria were collated in Mendeley Desktop (version 1.19.4).

Three papers identified in the search were not published in English. Submitting these texts to Google Translate, resulted in significant translation errors and they were excluded.
Screening and Agreement
Throughout the initial screening level, studies reviewed by the primary author were reviewed by the second and third authors and a consensus as to eligibility was obtained. The inclusion and exclusion criteria were checked against a sample of the papers found through the first search (28 papers) by the second author and ‘substantial’ agreement, Fleiss Kappa = 0.625,15 was found between the authors’ decisions on inclusion of the subset of papers. Any discrepancies were resolved with the help of the third author until a consensus was reached.
Data charting process
Data were extracted from the pertinent studies with the use of a standardized data charting form (where relevant) on the ensuing features: (1) Citation details, (2) sample size, (3) study aim, (4) results, and (5) definition given (Appendix 1).
Collating and Summarizing the Findings of included studies
Analyzing the data
The remaining 78 studies were examined for similarities and differences once the primary author had established familiarity with the data. The papers were then categorized into four main themes as follows: (1) epidemiology, (2) biomechanics, (3) biopsychosocial, and (4) miscellaneous. Each theme was subsequently divided into further sub-categories (Table 1).
Data validation
Agreement on study selection of the papers into the themes created by the primary author was attained and finalized through verification of 5% of the total number of articles (four of the total 78 papers) by the second and third authors. One paper from each of the four themes was picked out at random for verification. Any discrepancies found throughout the verification process were talked through by the authors until a final decision was reached.
Reporting
Data were analyzed by sorting the extracted data concerning the research question and objective of the review. The results were displayed in accordance with the four themes and their individual categories, using an illustrative outline of the key findings, summarized, and displayed in table format (Appendix 1).
Critical Appraisal
A total of 12 papers with primary data within the epidemiology category were appraised using The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) tool.16 This tool was created to assist authors when producing analytical observational studies and “…to facilitate critical appraisal and interpretation of results”.16,17(p1)
RESULTS
Overall, the search yielded 1,002 studies, of which 501 were screened after the elimination of duplicates (Figure 1). First level (title and abstract) screening eliminated 414 studies. Thirteen further studies were eliminated during the second level (full text) review (Figure 1). Four additional studies were found to be relevant during manual searching of reference lists, resulting in a total of 78 studies included in this study. Included studies were allocated into one or several of four main themes, epidemiology, biomechanics, biopsychosocial, and miscellaneous, and studies were classified to a specific category within the theme (Table 1). In five instances, papers were identified into two categories.18–22
Only 21% (27) of the total papers mentioned a definition of either low back pain (LBP), back pain or injury (Appendix 1). Definitions were most commonly given within the epidemiology category (18 of 27).
Epidemiology
Low back pain (LBP) in rowers was explored through peer-reviewed literature and included the incidence and prevalence of LBP, aggravating factors, sex differences, previous injury, and time off training or competition.
Incidence of LBP was reported as 1.5-3.7 per 1000 hours of rowing training and competition,21,23,24 and LBP prevalence was observed to be between 6% and 66% over 12 months.8,21 Seventeen papers reported incidence,8,20,21,24–37 the number of people developing LBP during one time, while nine papers reported prevalence,3,22,23,27,38–42 the number of people who have LBP at one time. Three papers employed a prospective design with both incidence and prevalence reported.8,21,29
Throughout the primary data sources, many papers utilized retrospective questionnaires.eg, 32,33,38 Of the 19 papers employing questionnaires, four adapted the standardized Nordic Musculoskeletal Questionnaire43 with additional rowing-specific questions.8,27,40,41 Four papers used custom-made rowing-specific questionnaires.21,33,34,37 One study adapted the Rugby Injury and Performance Project questionnaire44 along with interviews.24 Ten did not specify the questionnaire utilized.20,22,23,25,26,28,32,35,38,39
The low back was reported as the most commonly injured site for rowers in sixteen of the included studies.3,10,21,28,30,33,34,37,38,42,45–50 The low back injury rate was reported to be 53% of total injuries for rowers.41 Thus, many studies investigated risk factors for LBP in rowers.
The rowing stroke requires repetitive actions that place an increasing load on the lumbar spine.10 Wilson et al10 identified the most significant risk factors for LBP onset to be a history of lumbar spine injury and volume of ergometer training (Appendix 1). Stationary ergometers were suggested to increase the risk of LBP onset or exacerbation10,21,23,24,28,32 with many papers identifying use for more than 30 minutes to increase risk. Trease et al29 reported dynamic ergometers to be positively associated with a lower incidence and burden of low back injury compared to stationary ergometers. It must be noted here that the majority of studies observing prolonged ergometer use do not specify the type of ergometer. It may be inferred that for most articles, stationary ergometers are discussed as these are the more widely used models since their invention in 1981.51 In contrast, dynamic ergometers are a more recent innovation being created in 2010.51 Moreover, none of the studies included in the present review have commented specifically on the effects of prolonged dynamic ergometer use.
Training in winter was associated with higher rates of LBP development potentially due to increased volumes of land-based training,10,24,35 including the use of free weights and weight machines.28,29,32,39 Additional factors suggested to contribute to LBP in rowers included on-water rowing28,29 and long rowing sessions.23 Results regarding frequency of injuries by sex were inconsistent and inconclusive.21,27–29,33,35,37,38
Arend et al39 identified higher LBP intensity when training between seven to 16 hours per week compared with lower training volumes. Additionally, Newlands et al21 found a positive correlation between LBP and total training hours (on- and off-water) as well as with kilometers rowed per month (Appendix 1).
Previous history of LBP was positively associated with further LBP episodes.8,10,21,25,26,32 O’Kane et al25 observed that rowers with previous back pain had a higher risk of further episodes than rowers without. However, rowers with preexisting back pain had less time off training while individuals without were more likely to end their rowing career due to back pain.25
Finlay et al38 observed 39.2% of their cohort reported more than 21 days off training or competition while Teitz et al32 found 72% lost one month or less due to pain. One paper suggested that time lost due to pain was a poor indicator of injury severity as injured rowers in their study were able to complete a larger mean training volume than non-injured athletes.24 High injury rates have prompted investigation of the utility of pre-participation evaluation tools in individuals without pre-existing back pain without success.21,22
Epidemiological investigation is important in mapping the influence of LBP on the rowing population. Examining incidence and prevalence found that LBP was seen as the most common injury in the rowing population. Some consensus has been reached regarding training volume, the use of the ergometer, and a history of LBP constituting risk factors. Exploration of sex differences and risk assessment tools have not yet yielded any statistically significant results.
Biomechanics
Studies in this theme assess the movement involved in the rowing stroke. Sub-categories include spinal mobility, muscular contribution, pre-participation evaluation tools, and force produced by the lower extremity. Spinal mobility assesses the amount of movement accessed through the rowing stroke. Wilson et al47 compared lumbar spine kinematics when rowing on-water with ergometer rowing (Appendix 1). Both the ergometer and on-water rowing resulted in larger ranges of sagittal lumbar flexion by the final round of the step test compared to a full standing flexion test.47 Moreover, ergometer rowing showed a greater range of lumbar flexion and maximum angle compared to rowing on-water.47 Ng et al52 observed rowers experiencing LBP spent more time in increased flexion in the upper lumbar spine during the drive phase compared with rowers without LBP. Lumbopelvic movement has shown varying results between studies. Due to limited study numbers, no agreement has been found.50,53,54
Prolonged rowing caused greater ranges of spinal motion to achieve the same start and finish positions.55 Wilson et al46 found that as stroke rate increased, so did lumbar spine frontal plane angular displacement. These studies suggest that deterioration of technique due to fatigue may contribute to LBP.55
Muscular contribution describes muscles involved in the rowing stroke and assesses factors such as activation, symmetry between either side of the body and trunk flexor/extensor ratios. Electromyography has been used to assess muscle activation in rowers and Martinez-Valdes et al56 observed inefficient recruitment of erector spinae muscles in rowers with a previous history of LBP. Caldwell et al57 found that increased activity of lumbar extensor muscles (multifidus, iliocostalis lumborum, longissimus thoracis) may suggest muscular fatigue contributes to increased levels of lumbar flexion.
Additional muscles are suggested to affect the low back. Shortened hamstrings are suggested to alter the hip and low back mechanics resulting in pain or injury, however, this has not been demonstrated as a significant relationship.58
The epidemiology theme did not find utility of pre-participation evaluation tools. Clay et al49 utilized a functional movement screen (FMSTM) and found rowers with a higher risk of injury were significantly more likely to experience LBP during the rowing season.49 In contrast, Gonzalez et al59 cautioned against the use of the FMSTM to identify an increased risk of back pain due to the small effect and large variability observed in their study. Overall, these tools have not yet shown utility in assessing risk of injury in the rowing population.
The impact of asymmetry in the stroke motion on the lower limb has been the focus of a small number of investigations.60,61 While there was a measurable lack of symmetry in sweep rowing,61 there has been no evidence of this being a causal factor for LBP.62
In the biomechanics grouping, investigation into movement of the lumbar spine has suggested increasing angles of flexion are achieved with increased rowing speed and time spent rowing. Fatigue has been suggested to contribute to the deterioration of technique seen with prolonged rowing. Tools used to assess potential risk of LBP and lower extremity force have proved inconclusive.
Biopsychosocial
Five of the 78 articles explored the biopsychosocial influence of LBP. Wilson et al63 investigated the lived experience and impact of LBP on rowers. A culture of injury concealment was documented, influenced by fear and isolation63 (Appendix 1). McNally et al64 further suggested a lower rate of symptom reporting by rowers. Wilson et al63 discussed the complex condition athletes face when experiencing LBP and suggested that factors outside of the physical domain need to be addressed.
Ng et al18 utilized an individualized cognitive functional approach with adolescent rowers compared to a control group. Participants undergoing the cognitive functional approach had larger reductions in pain during ergometer rowing and reduced disability.18 Similarly, Thorpe et al65 demonstrated a 24% (pre-post-season) decrease in LBP following a back pain education session.
These papers observed some positive influence when considering a biopsychosocial approach to LBP in rowers. Although limited in number, these papers provided information on the use of back pain education and additional support required for athletes experiencing LBP.
Miscellaneous
A final small set of six studies were found to satisfy the inclusion criteria but did not fit the above categories and these were grouped under the miscellaneous heading. For example, Smoljanovic et al,66 described adaptive rowing at the Paralympic level advocating for an increase in racing distance. Injuries to adaptive rowers including the low back region are briefly mentioned, however, this is not the focus and there is no elaboration on LBP.66
Further although peer-reviewed, four of the six papers were identified as promotional pieces or using relatively older dataeg 67–69 and do not add to the present review.
Critical Appraisal
The ‘aggravating factors’ grouping within the epidemiology category was chosen for appraisal as this category may provide the greatest value to rowers and coaches when assessing preventative measures for LBP that may be considered. Using The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) tool, it was found that the abstracts and introductions of the papers provided relevant information (Table 2). Details of study characteristics and boundaries (such as participants, variables, measurement, and study size) were described including diagnostic criteria in the methods sections of the appraised studies. Results were commonly missing some of the STROBE recommended items although provided accurate information regarding participants, descriptive data, and outcomes of the study. Finally, the majority of information required by the STROBE process in the discussions was present, however, some did not discuss generalizability of the results (Table 2).
Eight STROBE items were missing in two-thirds of papers. These included representation of missing data and aspects of statistical analyses such as relative risk estimate and sensitivity analyses. None of the papers met all 22+ criteria.
DISCUSSION
The purpose of this study was to systematically map and investigate the currently available literature relating to low back pain (LBP) in rowing to inform athletes and coaches, and to identify gaps for future research.
In the general population, LBP has been associated with poor health, heavy physical work, obesity, smoking and low socioeconomic status.70 Athletes may, at first sight, be unlikely to be affected by these factors. However, athletes may be impacted by stress, anxiety, fatigue and reduced sleep and mood,71,72 factors that have been associated with increased risk of LBP. Furthermore, exercise and LBP have been expressed as a U-shaped curve where exercise reduces risk while simultaneously, high levels of physical activity can predispose to LBP.73 Elite athletes in one study were shown to have a higher prevalence of back pain in comparison with a physically active control group.27 Elite athletes may undergo a higher level of stress on the musculoskeletal system which may account for a higher back pain prevalence.27 Elite rowers were well represented as participants in the research reviewed in this study (23 of the 78 papers).
Many risk factors for LBP were identified, most notably, prolonged ergometer use and previous back pain history. Prevention may be a significant factor in avoiding the first back pain episode to decrease the chance of future LBP.74,75 Prevention has been investigated through the use of pre-participation evaluation tools, however, these have not yet shown utility in rowers. Prolonged ergometer use (particularly for more than 30 minutes) has been identified throughout the literature as a risk factor for LBP in rowers.7,10,21,23,24,28,32 The statement “prolonged ergometer use” has not been clarified further in the literature as to whether this pertains to stationary ergometer rowing or dynamic ergometer rowing, it may be useful in future to clarify this. This risk may be interpreted through biomechanical analysis of rowing technique on- and off-water, where it has been observed that technique seems to deteriorate with prolonged ergometer use and rowing at higher-intensities.46,50,53,55 During on-water rowing, the rower is required to maintain balance, through activation of hip and trunk flexors, particularly during the recovery phase to create a smooth stroke.76 Balance is not required in the same way while using the stationary ergometer as it would be when rowing on water which means the sensory feedback is also altered. This has been observed through the literature where some studies have shown that increasing angles of lumbar spine flexion may be the result of fatigue. Prolonged ergometer use and back pain history were the only significant risk factors agreed upon within the literature. Furthermore, many of the studies assessing rowing technique observed the rower while on the ergometer10 and results may not generalize to on-water rowing.
The present study found that a LBP definition was not well established, in line with previous studies.10 The terms low back injury and low back pain were used interchangeably by many authors.35,38,39,41 The authors of the Global Burden of LBP define LBP as “pain in the area on the posterior aspect of the body from the lower margin of the twelfth ribs to the lower gluteal folds with or without pain referred into one or both lower limbs that lasts for at least one day”.77(p968) In total, only 21% (27) of the papers included in the present review mentioned a definition of either LBP, back pain or injury (Appendix 1). Definitions were most commonly given in the epidemiology category (18 of 27). This has been reflected in the critical appraisal as 11 of the 12 papers appraised reported a definition (Table 2). Without effective defining of terms within the study or in using incompatible definitions, a comparison between studies is difficult to make. It has also been observed that a lack of common definition may affect prevalence data.3 Furthermore, this decreases the ability to build a literature base that adds evidence to create clarity and consistency of findings. Future research should include definitions of significant terms such as LBP to provide understanding for the readers as well as for quality reporting.
The literature within the present study contained many limitations concerning methods employed. These issues include low injury reporting, minimal prospective studies, low participant numbers and a lack of randomized controlled trials (RCTs).
With regard to low injury reporting, prevalence has been well mapped to highlight the widespread nature of LBP, however, the figures produced may vary considering the lack of reliable injury reporting mentioned in some papers.63,64 Decreased injury reporting was referenced in a 2020 systematic review of athletes stating that some may be reluctant to highlight their condition due to fear of repercussions.75 Some papers are calling for a more comprehensive view of pain management.71 This has been explored within the studies included in the biopsychosocial category of the present study. Specifically, these studies bring to light the importance of understanding and supporting the athlete by people around them. However, family and other people in an athlete’s circle may directly or indirectly pressure the athlete to ignore, not report pain or treat an injury with short-term remedies that may create long term negative consequences so that they can continue their sport.71,78 There seems to be a broad sporting culture that promotes playing through pain and injury and lessen its significance.79 This may create future episodes of back pain for the athlete. This culture of concealment seems to be common throughout many sporting disciplines75 and breaking this down may help to allow athletes to disclose pain earlier resulting in prompt rehabilitation and potentially less time taken off training and competition.63 Wilson et al63 recommended education for athletes, coaches and medical staff around appreciating the complexity of LBP, the significance of early disclosure, and the negative effect of concealment. Removing the stigma would allow athletes to disclose LBP which would additionally produce more accurate research data. Moreover, generating further prospective studies may produce more useful results.
A retrospective design was common in the epidemiological category (18 papers)20,22,23,25–28,30,32–41 with only four papers adopting a prospective design.8,21,24,29 Recall bias may have been an impact for study participants in remembering previous episodes of back pain and the factors associated with it.80 One study discusses their retrospective cross-sectional design as “a survey of the survivors” whereby only the athletes who continued their sport have been surveyed and others who may have left were not accessible, therefore, introducing bias.41(p452) This is a consideration for the remaining retrospective papers as to whether they have included rowers who left the sport. Prospectively designed papers with adequate sample sizes are needed to accurately survey risk factors for LBP.10,40
The epidemiological category has provided some conclusions when considering risk factors for LBP on the rower. However, conclusions are difficult to make from the biomechanical category due to a lack of cohesiveness and smaller study sizes. Increasing study sizes and using repeat methods will help to allow a more confident conclusion as to the effect of factors such as stroke rate, optimal lumbopelvic position and muscular activation. Additionally, for the results set of the present study, only one RCT was included.18 Conducting more RCTs would increase the understanding of and confidence in this literature. Further, critical appraisal of (a subset of) the literature can work to increase confidence in the findings to date.
For the present study, the subset of articles investigating aggravating factors was assessed against the STROBE tool to advance critical analysis of current knowledge of LBP in rowing. This subsection of data was chosen as it contained the most cohesive information and, therefore, conclusions have been easier to draw. The critical appraisal revealed significant strengths in reporting quality with some gaps around thorough reporting within the results. When read critically, the appraised literature is informative in providing epidemiological data. Researchers can view this subsection of data to highlight gaps in the literature such as a lack of definition. Additionally, this section of data highlights risk factors such as prolonged ergometer use and history of LBP that may be useful to coaches and athletes in thinking about LBP prevention.
Injury prevention is an important aspect of LBP in rowing. A six-staged process developed by Finch81,82 called The Translating Research into Injury Prevention Practice (TRIPP) has been developed whereby injury surveillance leads to implementation of preventative measures. Due to the methodological issues described earlier, this study may not inform injury surveillance in the first step of the TRIPP model.81,82 However, this scoping review may work to inform subsequent studies in highlighting areas for further investigation.
A 2021 consensus statement corroborated the findings of this study. That is risk factors such as a history of LBP and ergometer use (longer than 30 minutes) were highlighted similar to the present findings.7 Furthermore, the contributors to the consensus statement recognized the need for increased research in this area.7 Although methodologically less rigorous than the present scoping review, the consensus statement provided pertinent information regarding management of LBP in rowers that is in line with the present review and the quality appraisal contained herein and may be useful for rowers, coaches and health practitioners.7
Strengths
This study highlights the importance of prevention of the first LBP episode for athletes and coaches. Prolonged ergometer use should be approached with caution as it was the most commonly agreed upon risk factor. The rigorous methods used in this study including the use of a critical appraisal create increased confidence in the conclusions found.
Weaknesses
Underreporting by rowers and retrospectively designed studies may result in imprecise epidemiological findings and affect the validity of the study outcomes. Use of a strong definition such as that by the Global Burden of Disease77 would strengthen the data. There is a need to consider ways to decrease emotional and physical stress on athletes and break down the culture of concealment with regard to injury reporting.
Study limitations
Undertaking a larger critical appraisal to assess the reporting quality of all of the included papers would have given greater weight to the findings of the study.
CONCLUSION
This scoping review identified a body of literature that showed good quality epidemiological information to document the widespread effect of LBP on rowers. Many risk factors were highlighted, most significantly, back pain history and prolonged ergometer use. Issues of method within the literature were present including, a lack of LBP definition, issues with injury reporting, and small sample sizes. Avenues of investigation within the literature covered a range of topics e.g., spinal mobility, muscular contribution, pre-participation evaluation tools, lower extremity force, and biopsychosocial effect. These showed some promise, however, need further investigation. The widespread prevalence of LBP in rowers observed in this study shows the significance of the injury on this population. Previous back pain history and prolonged ergometer use have been recognized to be significant risk factors. Future research should include LBP definitions and ideally be undertaken prospectively. This would help to support coaches and athletes to consider ways to prevent LBP, increase injury reporting and early rehabilitation for rowers.
ACKNOWLEDGEMENTS
The study protocol was approved by the Ethics Committee of Unitec Institute of Technology, Auckland, New Zealand. The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in the article.
The scoping review protocol was registered prospectively with the open science framework on 7 April 2021. Reference: Athy, V. (2021, April 7). Examining the peer-reviewed literature regarding low back pain in rowing: A scoping review.
Retrieved from osf.io/b6ydj