INTRODUCTION
Physical therapy is at the forefront of promoting movement, maximizing health care, and minimizing the medical burden placed on society. It has been identified as a cost-effective means to reduce the medical burden on individuals and society, especially when access to physical therapy is provided early in the course of care.1–3 In particular, sports physical therapy and rehabilitation is crucial to limiting the burden of injuries and pain on athletes.4–6 Despite the focus on active movement-based strategies, restoration of prior activities and overall clinical outcomes is often limited by pain and related deficits such as motor inhibition, altered movement patterns, and activity impairments within sport (i.e inability to perform tasks such as running, jumping etc).
Pain and our society’s understanding of pain have led to growing medicalization of numerous conditions such as non-specific low back pain, various tendinopathies, and an array of arthropathies. Additionally, conditions such as non-specific low back pain are driving factors towards the management of pain over the prioritization of function and movement. Often the front line to managing pain in orthopedic and sports medicine conditions is one of pharmacological nature, including non-steroidal anti-inflammatory drugs (NSAIDs) and opioids, despite numerous documented adverse reactions (gastrointestinal, renal, delayed bony and soft tissue healing, addiction, etc).7,8 Pain is not necessarily indicative of tissue injury, and in sporting environments, it is important to differentiate injury, the impact of pain on the perceived safety of sporting participation, and related pain management.9 The demands of training and competition on athletes and the associated biopsychosocial responses can elicit varying pain responses.10 For the sports medicine professional, safe, low cost symptom modifying tools may have a place in reducing medicalization and unnecessary imaging, pharmacological use, and overall medical utilization while increasing patient autonomy.
POSITIVE UTILIZATION OF PHYSICAL AND MANUAL THERAPY
Orthopedic manual physical therapy is a specialty area of practice that is based on manual examination and a myriad of treatment techniques applied through clinical reasoning. These techniques include integrating exercise, patient education, and other physical therapy modalities to address pain, loss of function, and wellness.11 It is important to note that the definition and application of manual therapy practice is evolving and requires consistency to improve its usefulness in patient care.12 Current definitions and utilization of manual therapy are not passive, and labeling as such discredits its application.13 While the overall strength of evidence supporting manual therapy is limited,14 Level 1 and 2 randomized controlled trials have offered indications for utilization to improve short-term outcomes.15 Manual therapy has been identified as a cost-effective and low risk means to assist in the management of pain and modify symptoms to promote movement.2,14,16 Further, early manual therapy was also associated with a lower likelihood of receiving magnetic resonance imaging (MRI),17 pain management injections, and opioids, as compared with late manual therapy.18 When applied appropriately, there is the potential to reduce overmedicalization of orthopedic conditions often seen in athletics.15,19
A combination of the scientific process and modern methods of information distribution such as social media, have identified the value and importance of exercise not just within the physical therapy profession, but in health care as a whole.20,21 While “active” exercise therapies such as heavy-slow resistance and sprint training hold a primary function in the management of athletes, exercise may not always provide the desired analgesic and therapeutic effect when the athlete is already in pain, be it either acute or chronic.22 Further, in those with chronic pain, exercise induced hypoalgesia is reduced,23 potentially limiting its effectiveness. Thus, persistent pain with various therapeutic exercise or sporting exercise that does not achieve hypoalgesia for an athlete may facilitate chronic pain habits, ongoing medicalization, and likely requires intervention strategies beyond just “active” exercise therapies. Often, athletes are already hitting a prescribed level of exercise load, resulting in an era of load management and that focuses on a sweet spot of comprehensive exercise load. Pain itself is often a barrier to the numerous benefits of exercises and additional strategies and interventions may be needed to maximize the benefits of exercise and enhance sport participation.24 Thus, there is a place in clinical practice for symptom management and addressing pain with manual therapy while maintaining adequate sporting qualities through training.
When appropriately applied in an athletic setting, manual therapy may elicit short-term effects that enable a more enjoyable, manageable and sustained exercise experience.10,25 Reductions in pain, increased perceptual recovery and reducing athlete injury anxiety may lead to reduced injury risk and improved confidence in performance.26 In doing so, physical therapists are maximizing their practice by assisting in long-term, comprehensive musculoskeletal management and can facilitate physical activity longevity and favorable health care outcomes beyond an athlete’s playing career.3,10,27,28
LIMITATIONS AND PITFALLS OF MANUAL THERAPY
Physical therapy and manual therapy is not without risk.29 As with all health interventions, providers must weigh the risk against potential benefits of various treatments available to the patient and clinician. The risk of major adverse events in manual therapy is very low, including manipulation to the cervical spine, and has been shown to be lower than the risk of taking various medications and similar to that of exercise and control/passive/sham interventions.30 Furthermore, even with a significant body of research surrounding manual therapy, papers generally provide minimal detail regarding volume, intensity and descriptions of techniques. In general research has indicated limited value to manual therapy because of the common issues of small effect sizes and absence of documented long-term positive effects on outcomes.12
A significant and frequent danger when providing manual therapy is the utilization of nociceptive language.31–33 Language that is dated, focusing on inaccurate pathoanatomic nature in examination34 and injury mechanism,35 specificity of technique,36 and unreasonable expectations of outcomes related to techniques37 are common pitfalls. An overreliance on unsupported biomechanical mechanisms of manual therapy within clinical reasoning and patient education have consistently contributed to pitfalls related to the intervention. This includes outdated manual therapy concepts such as “functional leg length discrepancies,” “sacral torsions” and labeling patients as having joints “out of place/alignment”. Other common unsupported labels include “adhesions” “trigger points” and “subluxations” amongst many others. These concepts have been consistently shown to be unreliable in examination and theory, and can create unnecessary fears, pathoanatomical anxiety, and fear avoidance patterns following examination and treatment.32
These problems have the potential to drive dependency on manual therapy and ultimately limit patient independence and function.20,21 This overmedicalization of manual therapy has led to its perception as a low-value health care option, particularly in the context of long-term outcomes. In sports physical therapy, this can lead to negative feelings and emotions prior to competition and potentially hamper performance capabilities. Creating anxiety in athletes is a known risk factor for future injury38 and a therapist must ensure that modern and informed language match their interventions. Further, delaying safe and efficacious physical training and exercise therapy while waiting to resolve these perceived impairments often leads to deconditioning of athletes and inadequate sporting load.
THERAPIST UNDERSTANDING AND STRATEGY WITH MANUAL THERAPY
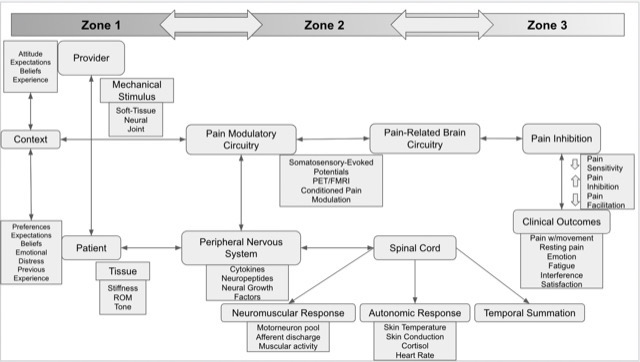
Therapists must understand the current concepts of mechanical input and associated neurophysiologic effects of manual therapy. When a therapist provides a manual intervention, a mechanical stimulus is applied upon an athlete and produces input into the dorsal horn of the spinal cord. This initiating a multi-factorial cascade of neurophysiologic effects stemming from the nervous system. Both the peripheral and central nervous system provide signal pathways that induce responses throughout the body. These include neuromuscular (i.e muscle activity), autonomic (i.e heart rate, cortisol), endocrine (opioid) pain modulatory, and non-specific (context, beliefs fear, expectations, etc) responses (Figure 1).16,35,39,40

With multiple body systems responding to the therapist’s treatment strategy, manual therapy requires patient education pre-, during and post- intervention. Patient education regarding manual therapy techniques needs to include honest discussion of its benefits and limitations. Despite the previously discussed limitations and pitfalls, providers can highlight the importance of understanding of and leveraging of the positive short-term outcomes (inter- and intra-session and between session) for long term improvement in outcomes41,42 With the patient and therapist properly informed and aligned as well as honest expectations discussed, manual therapy can then be reasonably applied.43
PRESCRIPTION, DOSAGE, AND PROGRESSION
The prescription, dosage and progression are a crucial component of manual therapy intervention but are extremely challenging to define. To improve internal validity and stay true to the medical model of research, a prescriptive application of manual therapy within randomized controlled trials has been trialed to varying degrees of success and application.44–47 This has been challenged12,48–50 due to the pragmatic nature of clinical practice, and is a likely contributor to inconsistent manual therapy findings and small effect sizes found in the literature. For physical therapists imbedded in a team setting, reimbursement considerations (i.e number of visits and services billable to insurance) may not be a restriction to provide care. In these instances, diligence must be provided to ensure to not overprescribe therapeutic intervention (exercise or manual therapies). Conversely, the increased frequency of athlete visits combined with their daily internal and external workload demands and the absence of pressure of reimbursement furthers the short-term efficacy of manual therapy utilization.
When practicing in an athletic training room or sports physical therapy clinic, the time-cost benefit of a technique must also be considered. The clinician’s clinical reasoning and ongoing evaluation of patient response is essential in appropriate and effective dosage of manual therapy. A clinicians preference and confidence with a specific intervention or technique has been shown to impact outcomes,35,41 which may be important when considering that multiple variations of manual techniques and interventions can result in similar outcomes.12,41,51 If an athlete is a responder to manual therapy, the dosage of should be based on achieving a clinically meaningful improvement to focally addressed symptoms (i.e 7/10 knee pain) and be related to a functional chief complaint (sport impairment i.e impaired jumping performance). Changes to the type, time, frequency, intensity, and volume of manual related to athlete improvement demonstrates the pragmatic nature of application.48–50
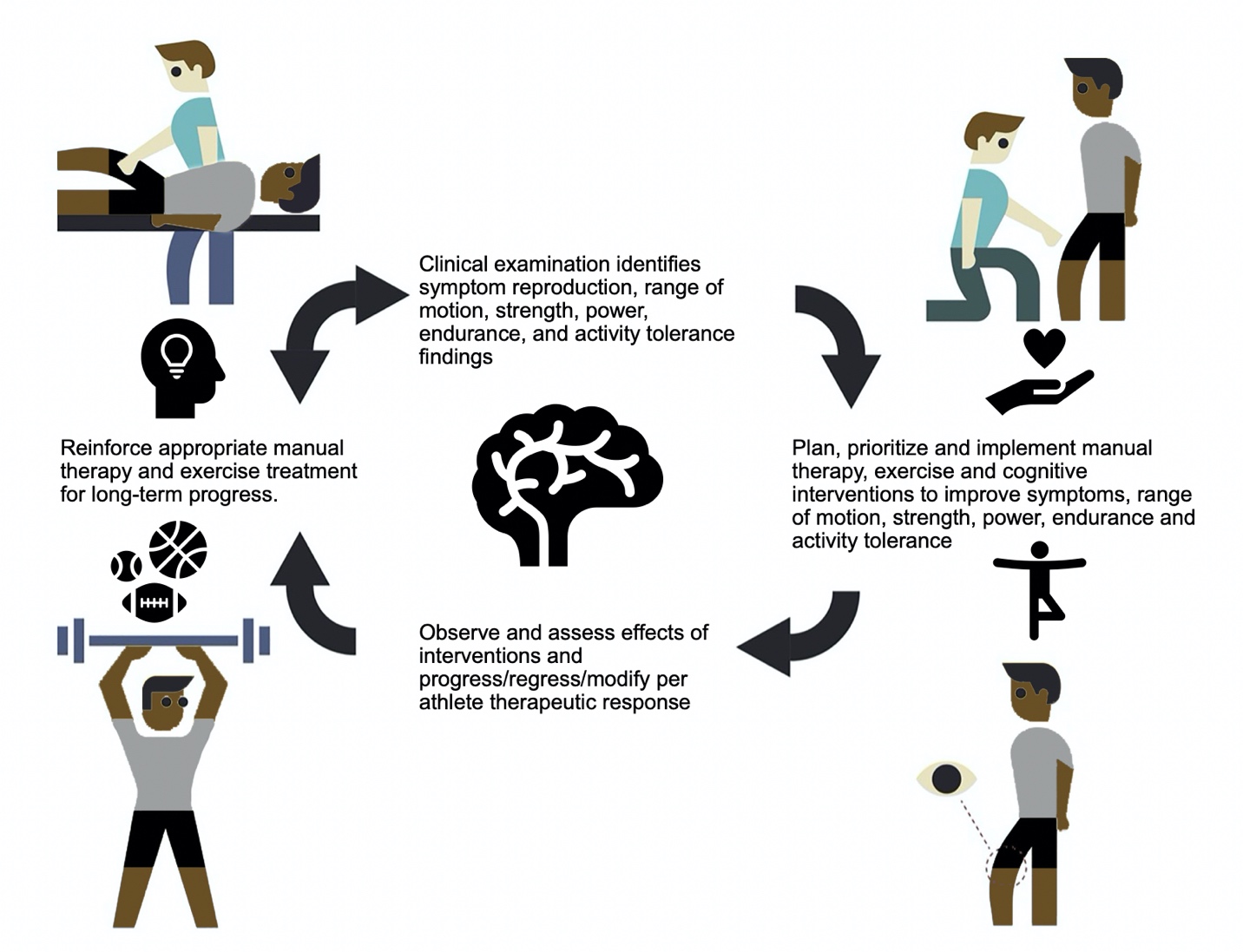
Consistent re-evaluation of functional movements and athlete limitations (i.e running, jumping, cutting, etc) should be performed within session to assess the short-term effectiveness of applied manual therapy techniques. This may also allow the therapist to identify if different techniques may need to be applied or if the individual is not responding to the specific intervention (Figure 2).41,51,52
__174446_.jpeg)
To improve athlete autonomy and independence, long-term application of manual therapy should be appropriately titrated so as not to foster dependence on any one provider or manual therapy technique.13,53 A transition to symptom-modifying mobility exercises that mimic or reinforce previously applied manual therapy interventions may replace the therapist as symptoms are reduced and function is restored. Ultimately this accomplishes the goal of creating athlete independence and transitioning to techniques that focus on active exercise variations.13 This progression is necessary for the athlete in order to promote long-term autonomy in their musculoskeletal management, physical attribute development and overall performance enhancement.
PRACTICAL IMPLICATIONS IN SPORT
There is an inherent time-cost benefit to all intervention forms available to physical therapists which makes intervention selection quite important. When providing athlete care, the provider must consider the demands placed on the athlete, both within and outside the sporting realm. When comparing outcomes against other “passive” therapies within the physical therapy evidence-base, manual therapy consistently is identified as more efficacious when compared to other interventions (electrophysiologic agents, taping, etc) outside of education and exercise. Recently a comparison of the effects of manual therapy has been likened to that of biophysical agents and other traditional modalities.54 As athletes seek to manage pain and continue competing and training, it is not a question of if the athlete will receive “passive” therapies, rather it is a question of which “passive” therapy will provide the most effective and efficient results within their comprehensive care model that includes ample exercise activity via the sport and its associated training.
While a full comparative review is beyond the scope of this commentary, the practicing sports clinician must consider how to compare and weight the cost-benefit of the numerous and easily applied manual therapy techniques with other pain and symptom modification modalities that are available. Manual therapy may have a challenged evidence base, varying non-specific mechanisms of action, and variance in application, but clinicians must acknowledge that not all symptom modification techniques are equal when comparing against other forms of intervention within physical therapy practice.15,19,44,55,56 In fact, the field of manual therapy likely acknowledges these deficiencies more than the those who use theory-based, non-outcome informed application of modalities such as electrical stimulation, ultrasound, and lasers. Practically speaking, the cost of machinery and technology and time required for utilization is often not worth the minimal potential benefits, which has led to changes in ethics statements, physical therapy education, reimbursement and overall trends of use.57–60 Meanwhile, manual therapy, which is an entry-level skill, may provide a cost-effective, mobile, and efficacious intervention that is consistently supported by clinical practice guidelines15,19,56,61,62 which provide related intervention comparisons and recommendations.
A multi-factorial, multi-disciplinary approach is necessary to improve outcomes within sports medicine settings. Within that construct, the benefits of manual therapy which includes building therapeutic alliance via touch, improving function via safe, cost-effective short-term pain modulation and facilitating education and exercise to be more impactful when they are limited less by pain and anxiety.
MANAGEMENT EXAMPLES
The following are examples of how clinically-reasoned manual therapy within a multi-modal musculoskeletal care model facilitates conservative management in an athletic setting:
Case #1
Acute Lateral Ankle Sprain
Clinical Vignette
The athlete reports to physical therapy 72 hours following an acute ankle inversion and resultant lateral ligament sprain. The Ottawa Ankle Rules are negative and the athlete desires to return to play within two days. Visual examination reveals moderate swelling and ecchymosis of the ankle region. The objective examination reveals limited ankle dorsiflexion in supine and weightbearing, the ability to resist manual strength assessment in all-planes, impaired balance during performance of a single leg squat test and antalgic pattern with running gait. The patient notes that their confidence in running is limited by pain that is 7/10 on the Numeric Pain Rating Scale.
Intervention
The athlete reports applying ice and compression therapy independently. The therapist elects to provide anterior to posterior graded mobilization to the talus on the tibiofibular joint. Ankle dorsiflexion range of motion is improved in supine but not in weightbearing. The therapist then performs an ankle dorsiflexion mobilization with movement technique until near symmetry is restored in a weightbearing ankle dorsiflexion test. A single leg squat test is again performed to compare pain and movement quality, both of which are improved. Following this improvement, running is attempted, with a noted decrease in the NPRS to 4/10. Local eccentric inversion and plantar flexion strengthening, single leg balance and lower compound lower extremity strengthening exercise were prescribed following this bout of manual therapy. The athlete is educated on continuing their compression and ice therapy independently. Education is provided on the natural history of ankle sprains, the encouragement of early weightbearing and returning to sport when able to meet the Pain, Ankle impairments, Athlete perception, Sensorimotor control, Sport functional performance (PAASS) criteria.19,63
The athlete follows up with the physical therapist prior to competition. Manual therapy is provided again, with the prior two techniques performed prior to assessment of the PAASS constructs with further reduction in pain on all assessment. Due to lingering ankle dorsiflexion limitations during single leg squat and 3/10 pain with activity, the therapist decides to utilize a talocrural and rearfoot distraction manipulation.45 The athlete is able to pass PAASS criteria and is provided a semi-rigid brace to compete in.
On future visits, the therapist provides a home exercise program consisting of banded self-mobilization with movement into dorsiflexion that mimics previous manual therapy techniques that the athlete can perform independently prior to sporting activity. Manual therapy is tapered off during future visits and is performed as needed according to pain presentation and when indicated post-exercise for recovery. Education and exercise programming is provided to the athlete on continuing a lower extremity single leg balance and strengthening program and to continue in order to reduce the risk of future lateral ankle sprain and chronic instability.
Case #2
Acute Low Back Pain
Clinical Vignette
A basketball athlete is boxing out an opponent. The opponent then outjumps the athlete who is in a flexed, athletic position. The opponent lands on the athletes back, forcing the athlete into loaded flexion and rotation before both fall onto the floor. The athlete attempts to continue participation but reports being unable to continue due to worsening perceived lumbar spine tightness. Evaluation by the physical therapist reveals no radicular symptoms and sensory and motor function is normal in all extremities. There is notable increase in tone of the paraspinal musculature on palpation assessment. Range of motion is limited in flexion (forward bending) and extension (backward bending), to a lesser extent. There is no glaring strength loss but a Gower’s sign is noted on the return from forward bending assessment. Slump assessment is negative for radicular symptoms.
Intervention
The athlete states that moist heat and laying prone relieves their symptoms. They are fearful to try and touch their toes. The treating therapist elects to perform soft tissue mobilization to address the increased tone about the paraspinals before re-addressing the fear of movement. Re-assessment of forward and backward bending reveals normalizing extension range of motion but apprehension persists with lumbar flexion. Graded lumbar central posterior to anterior mobilization was provided to identified painful segments. Traditional mobilization grades 1 and 2 are described as oscillations before the end range of motion to theoretically assist in pain control. Grade 3 and 4 mobilizations are various oscillations at end range tissue resistance to theoretically increase range of motion. Although the validity of the grades are up for debate, the actual application of grades 1-4 likely operate mechanistically within the neurophysiologic effect spectrum of manual therapy mechanisms.35 In this case, the grade of mobilization started as low grade, and was progressed per their reported pain response with posterior to anterior assessement and associated carry over to functional movement. Upon re-evaluation, pain was decreased with forward bending and the patient states that they had decreased apprehension to move. The athlete was then provided quadruped lumbopelvic range of motion exercises and cardiovascular exercise for 20 minutes that did not exacerbate their symptoms. Education was provided on the natural history of low back pain and the positive expectations as the individual was absent of radicular pain. The athlete remains apprehensive of sporting activity and their next competition is in 48 hours. The athlete’s home exercise program consists of continued low intensity cardiovascular activity and the same lumbopelvic range of motion exercises, and they are set for follow up assessment in the athletic training room three hours prior to the upcoming competition. As they noted symptom reduction with heat and extension, they were educated on continuing those therapies as indicated.
Upon evaluation prior to competition, the athlete has nearly restored their range of motion in all planes. However, Gower’s sign persists, with residual pain that is 3/10, and they note some apprehension in absorbing contact similar to the mechanism of injury during skill training. The athlete is educated on the purported neurophysiologic mechanisms of spinal manipulation and agrees to the treatment. The athlete is provided a side lying lumbar manipulation with immediate reassessment of forward bending. Pain and movement quality are improved, and the therapist introduces quadruped and closed chain motor control/strengthening exercises to reinforce the reduction in symptoms and improved movement tolerance. The athlete notes improved confidence and in consultation with team physicians and key stakeholders, the athlete returns to competition.
The following day, the athlete is instructed on mobility exercises that simulate the manual therapy techniques. Further proximal trunk and lower extremity strengthening drills are installed into their resistance training program in communication with the acting strength and conditioning coach. Manual therapy is provided as indicated only if the symptoms worsen or required further medical evaluation.
CONCLUSION
Education and exercise are the foundation of physical therapy intervention. When considering the barriers to these pillars, which include pain, anxiety, fear of movement and further injury, it is reasonable to consider the utilization of manual therapy as an adjunct to improve patient comfort, confidence, and to leverage short-term outcomes in a sporting environment where participation of exercise is already necessary. The primary goals of manual therapy are to reduce pain and promote safe and efficient movement. This is paramount in a sports setting, as short-term symptom modification is a significant driver in improving athlete comfort, confidence, and safety and thus potentially influencing athlete availability to rehabilitation, training, and competitive participation. Manual therapy is generally safe and cost-effective within a sports-medicine environment compared to, or performed in combination with alternative forms of care (pharmacologic, electrophysical, etc).17,18 A balanced and updated approach must be taken, as overdiagnosis and overmedicalization via manual therapy may result in more harm than good. A modern and clinically-reasoned approach can make these treatment interventions efficacious and move beyond the “passive” label by facilitating continued activity.
Disclosures
The authors state no conflict of interest in the creation of this manuscript.