
INTRODUCTION
Low back pain (LBP) is the leading cause of disability and a primary contributor to work absenteeism and loss of productivity globally.1–4 Over 50% of individuals with chronic LBP (CLBP) may not recover until one year later.2 Impairments from LBP include mobility deficits,5 physical disabilities,6 and balance disturbances.7–10 Several studies have identified alterations in muscle recruitment and movement patterns as potential pathomechanisms which further lead to spinal instability.6–9,11 Recently, evidence revealed that dynamic balance is reduced in individuals with CLBP and in individuals with a history of LBP as compared to asymptomatic controls.7,8 The reduced use of the lumbopelvic movement to maintain balance has been reported to be due to the reduced motion of the lumbar spine and hip.12 Furthermore, once individuals with LBP lose their balance, they have more difficulty regaining it, and balance deficits can persist even after their LBP has subsided.8 Although pain is a major factor in CLBP, pain is not the only impairment present in CLBP populations. Balance abnormalities and pain-avoiding compensations could further contribute to an individual’s increased re-injury risk and chronicity.2,8,9 Moreover, individuals with LBP can be fearful of performing dynamic tasks because of a fear of additional pain and injury in response to the movement.2,8,9
Uncertainty remains regarding the best treatment approach for LBP. Evidence suggests that exercise therapy is a moderately effective intervention for treating LBP.6,13 A systematic review found that therapeutic exercises were associated with small-to-moderate effects on pain and with an increased likelihood of return-to-work for patients with LBP.13 Spinal stabilization exercise (SSE) programs are widely used by physical therapists for rehabilitation of patients with LBP.14–17 Evidence has shown that recruitment of spinal stabilization muscles (e.g., transversus abdominis and lumbar multifidi) may be altered in patients with LBP as compared to healthy controls. It has been proposed that SSEs are used to retrain proper activation and coordination of the trunk musculature to increase spinal stability and reduce pain.14–18 SSEs also have been shown to be effective for improving pain, disability, and physical performance in patients with LBP.4,16–18 Systematic reviews have indicated that SSEs were more effective than general exercises for decreasing pain and improving disability in patients with LBP.4,16,18 Furthermore, recent research reports showed that some forms of SSEs have promising outcomes on postural control in patients with LBP.19,20
Although balance has been used as an outcome measure to examine the effects of SSEs on patients with LBP, the balance measures commonly used in the literature consist of only static postural control assessments and lack dynamic component assessments.21,22 For instance, force plates and the NeuroCom Balance Master® measure ground reaction forces and center of pressure (CoP) displacement, and both provide quantified measures of static or semi-dynamic postural control, but do not measure an individual’s ability to maintain balance while performing a purposeful maneuver.8,21,22 Moreover, these static balance tests usually are used in a laboratory setting, are expensive and time-consuming, and often are impractical for use in clinical settings.8,21
In recent years, several tests have been used to investigate dynamic balance in LBP populations, such as the Star Excursion Balance Test (SEBT),7,10,23,24 the Y-Balance Test (YBT),8,25 and the functional reach test.26,27 Of these dynamic tests, the reliability and validity of the YBT has been established specifically for the CLBP population. In addition, the YBT is a shorter version of the SEBT, and is more feasible for clinical practice. The YBT evaluates single-leg-balance, dynamic neuromuscular control, proprioception, and strength of an individual while simultaneously moving the non-stance limb in anterior (ANT), posteromedial (PM), and posterolateral (PL) directions.21,28,29 The YBT is portable and easy to administer, and it requires little training, making it practical to use in multiple settings.8,25,28,29 Recently, a relaiblity and validity study aimed to determine the inter-rater reliability of the YBT and to compare dynamic balance between young adults with CLBP and an asymptomatic group found that the YBT had an excellent inter-rater reliability, with intraclss correlation coefficients ranging from 0.99 to 1.0. In addition, the CLBP group had a significantly lower composite score (p < 0.001) and shorter reach distances in the ANT (p = 0.023), PM (p < 0.001), and PL (p = 0.001) directions than the asymptomatic group.25
Initial evidence regarding the effect of SSEs on postural control in patients with LBP has been encouraging; however, balance measures used in these studies primarily assessed static postural control and did not have dynamic components, which are imperative for performing daily functional activities. Additionally, these static balance tests are impractical for use in clinical settings. Given that dynamic balance is a vital aspect of everyday life and that diminished balance is a well-recognized impairment in individuals with LBP, including athletic patients with CLBP who are physically active, it is important to routinely include a relatively quick and cost-effective balance test in physical therapy (PT) practice, and to incorporate an exercise program that is useful for maintaining and improving balance in LBP populations. However, there is a lack of evidence supporting the effectiveness of SSEs on improving dynamic balance. To date, no randomized clinical trials have been conducted to assess the effectiveness of SSEs on dynamic balance in adults with CLBP using the YBT. Therefore, the primary purpose of this study was to determine the effectiveness of SSEs on dynamic balance in adults with CLBP. The secondary purpose of this study was to examine whether or not the participants who received an SSE program (treatment group) would have greater improvement in pain intensity and disability level than those who received a general exercise (GE) program (placebo group). The GE program consisted of general range-of-motion (ROM) and flexibility exercises.
METHODS
Study Design
This study was a double-blinded randomized clinical trial, to compare two exercise programs: SSE vs. GE on dynamic balance, pain intensity, and disability level in adults with CLBP. The two independent variables were group, which was a between-subject factor, and time, which was a within-subject factor. The independent variable of group had two levels: (1) the treatment group which received SSEs, and (2) the placebo group, which received general ROM and flexibility exercises. The independent variable of time had four levels: baseline, and 2 weeks, 4 weeks, and 8 weeks after intervention. The three dependent variables were: (1) dynamic balance measured by the YBT, (2) pain intensity measured by the Numeric Pain Rating Scale (NPRS), and (3) disability level measured by the Modified Oswestry Low Back Pain Disability Questionnaire (OSW).
Participants
The sample size for this study was determined based on a priori power analysis using G*Power version 3.1.9 using a small-to-medium effect size of 0.20 and an alpha level of 0.05.30 Based on the analysis, 40 participants were needed to ensure an adequate power level of 0.80 for a mixed-model analysis of variance (ANOVA) test. Participants were recruited regardless of ethnicity, sex, or race through flyers, word of mouth marketing, and emails. Approval from the Texas Woman’s University institutional review board was obtained for the study, and it was registered with ClinicalTrials.gov (NCT03597191). Once the participant agreed to participate in the study, the participant signed a written informed consent form. Consenting participants were screened for their eligibility, and those who qualified were assigned randomly to one of the two groups. Eligible participants were individuals who had CLBP (back pain for a duration of more than 12 weeks).2 Additional inclusion criteria included: (1) age of 18 to 65 years; (2) ability to understand, speak, and follow verbal instructions in English; and (3) a minimum pain intensity score of 2/10 using the NPRS in the past week.
Participants were excluded from the study if they have had or reported any of the following: (1) serious spinal conditions, such as fracture, infection, or tumor; (2) signs of nerve root compression; (3) a history of lower extremity or lumbar spine surgery; (4) a history of hip, knee, or ankle pain in the previous two years; (5) current pregnancy; (6) systemic disease (e.g., rheumatologic or neurological disorders); (7) vestibular or other balance disorders; (8) ongoing treatment for inner ear, sinus, or upper respiratory infection; (9) a concussion within the previous three months; (10) a history of falls or fear of falling; and (11) a need for any form of walking aids (cane, walker). Participants were screened with neurological tests, which included reflexes, sensation, strength, and the straight-leg-raise (SLR) test for the lower extremities to further assess their eligibility for the study. The SLR test was considered positive when pain referred below the knee was present during passive SLR testing and was used to rule out participants with lumbar radiculopathy. These neurological tests are parts of a standard PT examination used in clinics for assessing neurological signs and symptoms. In addition, a physical examination was performed based on the test procedures described by Hicks et al.14
Instrumentation and Outcome Measures
The Y-Balance Test Kit (Functional Movement Systems, Inc. Chatham, VA) was used to assess dynamic balance in this study. This kit contains a single central stance platform with three moveable reach indicators arranged in the ANT, PM, and PL directions. Dynamic balance of an individual is quantified by measuring how far the individual places the reach indicator relative to the stance platform while maintaining a unilateral stance. A farther reach distance is indicative of a greater dynamic balance.28 The YBT has been shown to be a reliable measure of dynamic balance, with intraclass correlation coefficients (ICCs) ranging from 0.85 to 0.91 for intra-tester reliability, and from 0.99 to 1.00 for inter-tester reliability.28 The reliability of composite reach scores has been reported to be good-to-excellent, with the ICCs being 0.91 for intra-tester and 0.99 for inter-tester reliability. The YBT has a minimal detectable change of 8.62 centimeters.28 The reach distances were measured in centimeters and were averaged and normalized to the participant’s leg length. Leg length was measured twice for each leg, and the two measurements were averaged. In particular, participants’ leg length was measured to the nearest millimeter using a tape measure from the inferior tip of the anterior superior iliac spine to the distal border of the ipsilateral medial malleolus with the participant lying supine on an examination table.25 The composite score was calculated by taking the average between the right and the left reach distances for all three directions and then summing the averages of the three reach directions. The score was then divided by three times the average leg length and multiplied by 100.31 The YBT composite scores were used for statistical analysis and collected at baseline, two weeks, four weeks, and eight weeks after intervention was initiated.
Examiners
Two investigators participated in this study. Investigator #1, the primary investigator (PI) was blinded to participants’ group assignment and intervention and performed the eligibility screening and standard PT examination for all participants. In addition, the PI collected the pre- and post-intervention measurements of dynamic balance using the YBT, pain scores using the NPRS, and disability level using the OSW. Investigator #2 was blinded to participants’ pre- and post-intervention measurements and was responsible for group allocation and administering the intervention, either an SSE program or a GE program, to participants in both groups.
Procedures
Eligible participants filled out an intake form, including questions about demographic data (age, sex, height, weight, occupation, limb dominance), duration of symptoms, painful side of the LBP, and physical activity level (minutes per week). The leg dominance was determined by asking the participants to report their preferred leg used when kicking a ball.32 In addition, participants completed the Fear-Avoidance Beliefs Questionnaire (FABQ) and Patient-Reported Outcomes Measurement Information System®-29 (PROMIS-29), which were used to describe the participants of this study. All participants were asked to rate their average pain intensity in the low back in the past week and to rate their current pain level using NPRS. Next, participants were asked to complete the OSW. The FABQ, PROMIS-29, NPRS, and OSW have been reliable and valid tools for assessing LBP-related fear-avoidance beliefs, participants’ traits, pain intensity, and perceived disability, respectively.33–38
Next, the YBT was used to assess participants’ dynamic balance. Each participant’s leg length was measured bilaterally in centimeters and was used to normalize reach distances because leg length has been shown to be a factor affecting YBT performance.39 Next, each participant was asked to slide a reach indicator along a pipe in the three testing directions: ANT, PM, and PL on both legs as described in details by Alshehre et al.25 The PI was responsible for giving verbal instructions and visual demonstrations of the YBT, as well as recording the YBT measures. The trial was discarded and retried when the participant (1) moved the foot of the stance leg from the platform or crossed the marked line, (2) kicked, pushed, or stepped on the reach indicator, (3) touched the floor with the reaching leg, or (4) lost balance before returning to the standing position. To reduce fatigue, participants were given a rest of a minimum 10 seconds between each reach and 30 seconds between each direction of testing.40 The reach distance was measured to the nearest centimeters by reading the line at the proximal edge of the reach indicator. Three successful test trials in each direction (ANT, PM, and PL) on each leg were recorded and normalized to the leg length and the composite score was used for data analysis.
Interventions
Participants in the treatment group were instructed in the SSEs, modeled after the SSE program designed by Hicks et al.14 Each participant was instructed to perform four exercises in total, one exercise from each of the following four categories: (a) abdominal bracing, (b) quadruped, (c) prone plank, and (d) side plank exercises. Each exercise was progressed and advanced in difficulty by increasing repetitions, hold times, and/or extremity movements. For the SSEs, the progression of exercises was based on the participants’ performance at each supervised PT session based on pre-established criteria by Hicks et al.14 The SSE program and criteria for progression are listed in Appendix A.
The placebo group performed a GE program, consisting of ROM and flexibility exercises for the low back and lower extremities. Each participant was instructed to perform four exercises in total, one exercise from each of the following four categories: (a) knee to chest, (b) lower trunk rotation, (c) prone press-ups, and (d) hamstring stretch exercises. These exercises were progressed by increasing repetitions and pain-free ROM. The exercise programs and criteria for progression are listed in Appendix B.
On the first visit, the participants in both groups were instructed in the exercises at a level that they could perform without pain. All participants were provided exercise handouts and also were asked to fill out an exercise log form to track the frequency of their home exercise sessions and to determine their compliance. In both groups, Investigator #2 instructed and corrected performance when necessary, and progressed the exercise program for each participant. As such, when participants performed the exercise with proper technique and without any rest breaks, they were instructed to progress to the next level of the exercise and were asked to discontinue the previous level of that exercise from their program. The proper technique was achieved by instructing the participants to tighten their abdominal muscles while breathing normally and maintaining a steady continuous muscle contraction with no recruitment of accessory muscles.41 Participants were instructed to perform the most updated exercises at home once a day at least five times a week.
The participants were asked to attend a total of four to eight supervised PT sessions and one follow-up session after the four-week intervention was completed for exercise progression and to ensure that they performed the exercises properly. Each session took about 30 to 45 minutes for exercise progression or an hour for collection of outcome measures and exercise progression. The intervention frequency and duration were chosen to reflect common PT practice. Each participant also was asked to perform their assigned exercise program at least five times per week, and the on-site visits were counted toward the required exercise frequency. After the 4-week intervention, each participant was asked to continue their exercise program at home five times a week for another four weeks. On their follow-up visit at week eight, the participants were instructed on how to progress their exercises.
All participants were instructed to bring the exercise log to each visit and to submit it to the investigators at the eight-week follow-up in order to determine compliance with the program. The average compliance was calculated using the completed exercise sessions divided by the prescribed exercise sessions. This equals to the number of exercise sessions completed out of the total possible exercise sessions. For this study, the average compliance for completing the prescribed home exercise program for the first four weeks (supervised PT sessions), the last four weeks (unsupervised PT sessions), and the total compliance for the duration of the study for both groups was calculated.
Data Analysis
All statistical analyses were performed using SPSS Statistics, Version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including frequencies, means, and standard deviations, were calculated for the demographic data of the participants and the outcome measures (YBT composite score, NPRS, and OSW). Independent t-tests were used for ratio data to determine if there was a difference between groups at baseline, including demographic data, such as age, weight, height, body mass index, and duration of symptoms, and baseline outcome measures. Chi-square analysis was used for non-ratio data to determine between-group differences for non-parametric baseline data, such as sex, onset of symptoms, pain distribution. Three separate 2 (group) x 4 (time) analyses of variance (ANOVAs) with repeated measures were used to determine any differences in the three outcome measures between groups. Follow-up analysis was performed if there was a significant interaction. The alpha level was set at 0.05 for all statistical analyses.
RESULTS
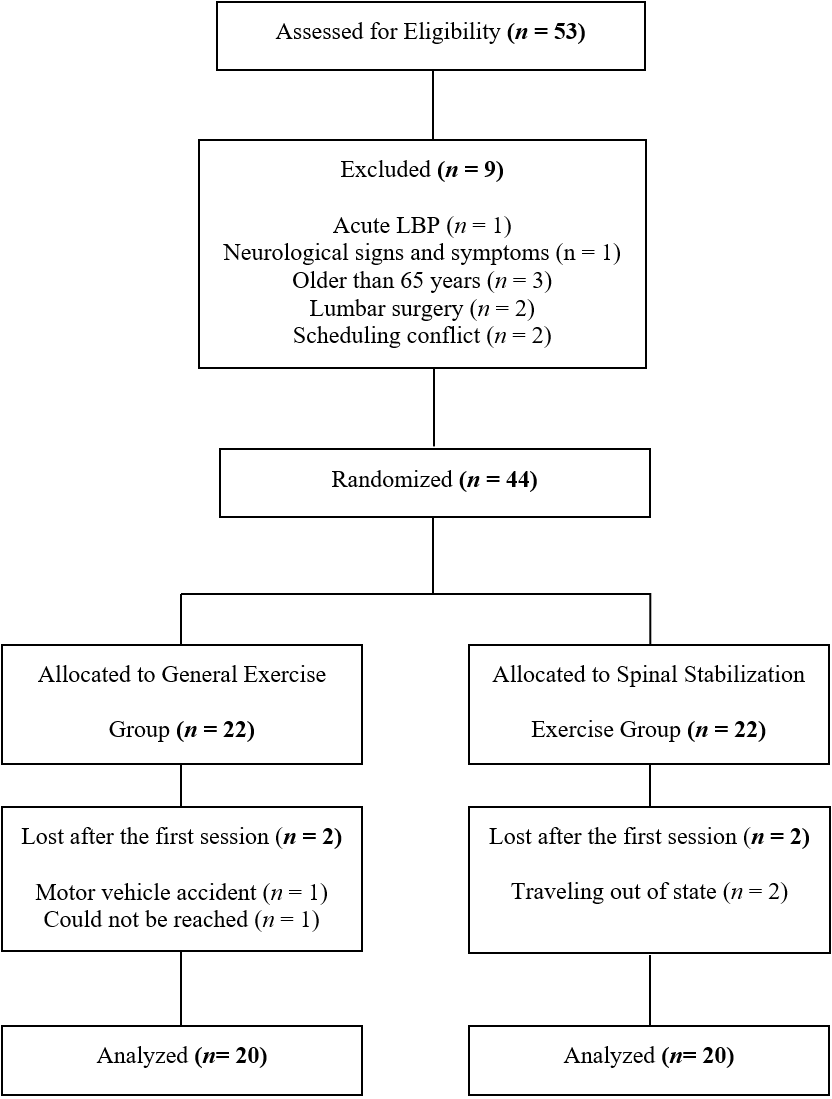
Fifty-three participants were recruited for the study and were also assessed for other outcomes. The CONSORT diagram in Figure 1 summarizes the screening, enrollment, randomization, and analysis of participants for this study. The 40 participants who completed this study were generally young with an average age of 39.9 ± 12.5 years and a range of 21 to 64 years. Both groups had lower physical activity levels (99.7 ± 145.1) than the recommended weekly minutes by the 2008 guidelines for adults, which is a minimum of 150 minutes per week.42 All participants had CLBP without signs of lumbar radiculopathy, with symptoms averaging for 95.2 ± 87.5 months. In addition, the participants had an average NPRS score of 3.5 ± 1.6 and an average OSW score of 18.1 ± 9.1, indicating that participants, in general, had relatively low pain intensity and a mild disability level. Table 1 describes the characteristics of the participants who completed the study.

Outcome Measurements
Table 2 displays the means and the standard deviations for the YBT, NPRS, and OSW at each time point. All three outcome measurements showed no significant differences between groups at baseline, except in the YBT composite scores. There was a significant difference in the dynamic balance between groups (t = -2.575, p = 0.014), with a lower YBT composite score in the GE group (72.9 ± 14.0) than in the SSE group (82.1 ± 7.7). Therefore, 2 x 4 ANCOVA with repeated measures was performed with the baseline YBT composite scores of all participants were used as covariates. The ANCOVA results revealed a statistically significant interaction of group by time for dynamic balance (F = 7.146, p < 0.001, partial η2 = 0.162), which indicates that there was a difference between the GE and SSE groups in dynamic balance over eight weeks as presented in Figure 2. Six separate 2 x 2 ANCOVAs with repeated measures were used to test for between-group differences in dynamic balance. A significant difference was found between groups from four weeks (p < 0.001) and eight weeks (p = 0.007) compared to baseline, and from two weeks to four weeks (p = 0.002), with the SSE group demonstrating higher YBT composite scores than the GE group. However, there were no statistically significant differences from baseline to two weeks (p = 0.098), two weeks to eight weeks (p = 0.107), and four weeks to eight weeks (p = 0.413) between groups. In addition, a significant main effect of time on the dynamic balance was found. Both groups demonstrated a significant improvement in dynamic balance from baseline to two weeks (p < 0.001), 2 weeks to 4 weeks (p = 0.023), and two weeks to eight weeks (p = 0.004), but there was no statistically significant difference from four weeks to eight weeks (p = 0.144) (Figure 2).
_at_baseline__and_2_weeks__4_weeks_.png)
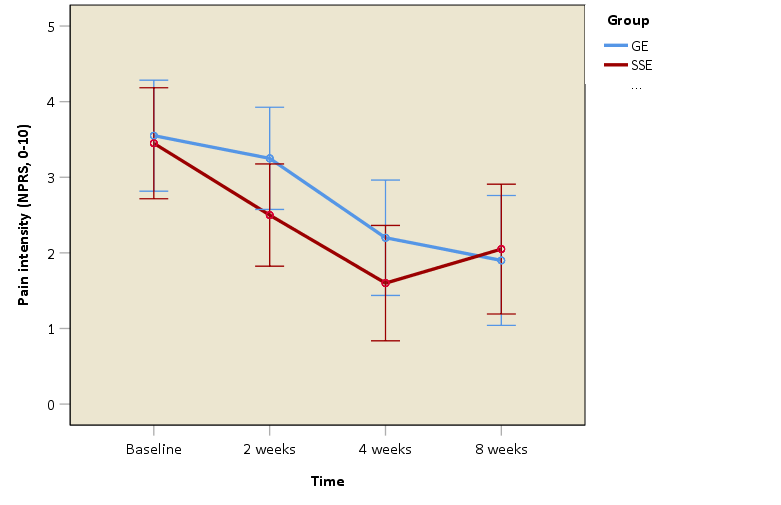
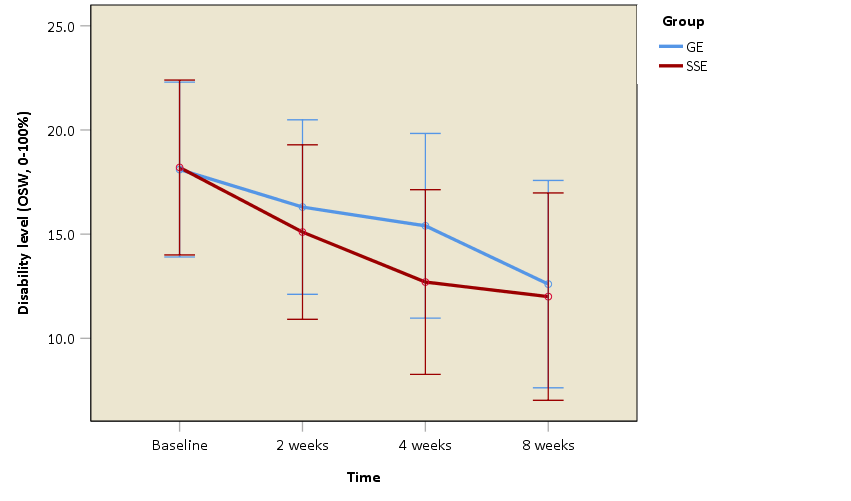
The ANOVA with repeated measures for the NPRS and OSW scores revealed no statistically significant interaction of group by time (F = 1.185, p = 0.319, partial η2 = 0.030), (F = 0.538, p = 0.605, partial η2 = 0.014), respectively. However, there was a significant main effect of time (p < 0.001) for both the NPRS and OSW scores. However, a significant main effect of time (p < 0.001) for both the NPRS and OSW scores was found. Post-hoc pair-wise comparisons showed significantly lower NPRS scores from baseline to two weeks (p = 0.007), from two weeks to four weeks (p < 0.001), but there was no statistically significant difference from four weeks to eight weeks (p = 0.818) (Figure 3). Similarly, post-hoc pair-wise reveled that both groups demonstrated a significant reduction in disability level from baseline to two weeks (p = 0.017), from two weeks to four weeks (p = 0.047), but there was no statistically significant difference from four weeks to eight weeks (p = 0.117) (Figure 4).
_at_baseline__and_2_week.png)

Home Exercise Compliance
Table 3 lists the means, the standard deviations, and the compliance rates for home exercise compliance for both groups. No significant differences in compliance between the two groups for the duration of the study. However, paired t-tests for within-group differences revealed that the home exercise compliance was significantly higher during the first four weeks after initiating the intervention as compared to the last four weeks of intervention for both groups (t = 2.456, p = 0.024 for GE group, t = 2.163, p = 0.044 for SSE group). This indicates that all participants regardless of group performed their home exercises more often in the first four weeks, which included supervised PT sessions than they did in the last four weeks, which had no supervised PT sessions.
DISCUSSION
The results of this study show that four-week supervised SSEs were superior to GEs in improving dynamic balance in adults with CLBP after eight weeks of intervention. This implies that the SSE group was able to demonstrate better dynamic balance than the GE group for the first four weeks after initiating intervention, which included home exercises and supervised PT sessions. Then, the SSE group maintained the improvement of the first four weeks but showed no improvement in dynamic balance during the last four weeks, which included the participants performing exercises at home with no supervised PT sessions. However, there was no difference between the GE and the SSE groups in dynamic balance during the last four weeks of the intervention. These results support previous studies,19,20 which have shown that those with LBP who received SSEs for four weeks had significantly improved balance as compared to a control group. However, these two studies utilized different methods than the method used in the current study to assess balance, as Kim et al.19 and Rhee et al.20 used a pressure platform and force plates, respectively, to measure CoP excursions for balance ability. The authors of the prior studies hypothesized that SSEs might have improved neuromuscular responses to compensate for postural control deficits in patients with LBP.19,20
Given that balance is a motor control process which regulates movement quality and creates stability; improved neuromuscular control in this patient population can be achieved in part through strength from the lumbar spinal stabilizer muscles.43 Previous evidence has shown a delay in the firing of the deep abdominal muscles and decreased recruitment of the transversus abdominus and lumbar multifidus muscles in patients with CLBP as compared to asymptomatic individuals.14–17 Evidence also suggests that altered lumbar proprioception in those with LBP may cause reweighting of visual and vestibular sensory inputs to compensate for impaired proprioception in order to maintain an individual’s balance.44 An SSE program is a motor control intervention which has been used to retrain proper activation and coordination of the trunk musculature to increase spinal stability and reduce pain.14,18 In particular, spinal stabilization muscles, such as transversus abdominis and lumbar multifidi have been reported to play a major role in maintaining postural stability. Proper activation of these muscles in a feedforward mechanism reduces displacement of the body’s center of gravity.15 Based on these findings, it is speculated that SSEs may minimize faulty movement strategies and compensatory muscle contractions by properly coordinating abdominal and back musculature during functional tasks in the SSE group, which possibly led to better dynamic balance performance following the SSE program.
In contrast, a previous study reported that four weeks of SSEs combined with usual PT care (hot pack, ultrasound, and transcutaneous electric nerve stimulation) compared to usual PT care alone did not show greater improvement in postural control in patients with CLBP.45 However, balance was assessed differently between the studies. Salavati et al.45 assessed postural control using a Biodex Balance System®. In the current study, balance was measured using the YBT, which could be considered a more challenging balance task. It also could be argued that the two studies measured different constructs related to balance.
After the four-week supervised intervention, there was a trend that the GE group improved in dynamic balance during the last four weeks of the study. The GEs were designed to be similar to the SSEs in terms of frequency, duration, and number of one-on-one supervised PT sessions as well as contact time with the treating physical therapist. It is likely that the GEs, which consisted of ROM and flexibility exercises for the low back and lower extremities, could be learned more easily and performed independently at home by the participants, whereas SSEs may require supervised PT training. The SSEs could be considered a more complex exercise regimen and may require higher cognitive skills to be learned and performed as compared to the GEs. In addition, in terms of exercises intensity, it could be argued that level three of the GEs could be easier to perform, whereas level three of the SSEs could be considered more difficult, requiring more effort and PT supervision to perform correctly. Therefore, it is possible that the SSE group did not show continued improvements on dynamic balance because the effort needed to perform the SSEs was not to the same level of intensity it was for the first four weeks, which included PT supervision. However, it is also not certain whether the SSE group used proper exercise form during the unsupervised portion of the intervention. In addition, evidence has demonstrated that lower-extremity flexibility could affect YBT performance in healthy populations.46,47 Therefore, the GE group could have potentially increased lower-extremity flexibility after eight weeks of intervention and therefore could have been able to reach farther distances during the YBT. However, lower-extremity ROM was not assessed after implementing the intervention in this study, so it was not certain whether the improvement on the YBT performance is the result of increased lower-extremity flexibility.
The results of this study also indicate that all participants, regardless of intervention, made significant improvement in dynamic balance after eight weeks. A point of discussion here is that it is apparent that YBT performance may require both spinal stability and ROM/lower-extremity flexibility since both exercise programs seemed to help improve dynamic balance performance after eight weeks. It is also important to note that the small magnitude of change observed in dynamic balance in this study during the last four weeks may be due to the unsupervised nature of the exercises. In this study, home exercise compliance was significantly higher during the first four weeks after initiating the intervention as compared to the last four weeks for both groups. This indicates that all participants performed their home exercises more often in the first four weeks, which included supervised PT sessions, than they did in the last four weeks, which had no supervised PT sessions. Evidence has shown that PT supervised SSEs were shown to be more effective than the unsupervised PT SSEs in patients with LBP.41
All participants regardless of the intervention they received showed significant improvements in pain intensity and disability level over eight weeks. However, the decrease in pain intensity and disability level did not exceed the MCID or MDC, which is 2 points for the NPRS and 10 points for the OSW in patients with CLBP.36,48 This finding agrees with a pooled analysis that reported no significant benefits for pain or disability between SSEs versus other forms of active exercises. The authors indicated that improvements were minimal and not regarded as clinically significant.49 In addition, Salavati et al.45 reported that four weeks of SSEs combined with usual PT care as compared to usual PT care alone resulted in no significant improvement in pain and disability ratings in patients with CLBP. The trend toward better results in pain intensity and disability level suggests that significant changes may take longer than eight weeks to become detectable.
The current study is unique because it is the first to assess the effectiveness of SSEs on dynamic balance in adults with CLBP using the YBT. This study evaluated dynamic balance in a multi-planar manner while performing dynamic tasks that considerably challenged the stability of the spine. This study also demonstrates that the YBT is able to detect change in dynamic balance over time, suggesting that the YBT may be a useful tool for clinicians to assess dynamic balance deficits in patients with CLBP and monitor treatment progression. A better understanding of impairments associated with LBP would assist clinicians in developing personalized intervention programs and individualizing exercise prescription to address those identified at high risk for recurrent LBP.
Strengths and Limitations of the Study
Strengths of this study include the implementation of a double blinded, concealed allocation randomized clinical trial design in which the participants and the investigators were blinded. Specifically, one investigator was fully blinded to the participants’ group allocation and intervention while the other investigator was blinded to the participants’ pre- and post-intervention measurements. All participants were not informed whether they were assigned to the placebo or to the treatment group. Therefore, the design of the study provided control over potentially important sources of bias, so that the observed effects of the implemented interventions were less likely to be due to chance. However, there are limitations in this study. First, participants were recruited by means of advertisements; therefore, it is possible that individuals seeking medical care for their LBP are different from those responding to an advertisement, thus limiting the generalizability of the study results. In addition, only individuals with CLBP were enrolled in the study. Therefore, the findings are not applicable for individuals with acute or subacute LBP. Another possible limitation is that participants reported low pain intensity, mild disability level, and low physical activity level which limits the generalizability of findings to non-athlete individuals with mild pain and disability levels. Lastly, although efforts were made to control the potential influence of confounding factors that may affect YBT performance, factors such as knee and ankle strength and joint ROM were not investigated.
Recommendations for Future Research
Future studies are warranted with supervised SSEs and long-term follow-up to examine the effectiveness of these exercises on dynamic balance in individuals with LBP. In addition, future studies should consider measuring participants’ lower-extremity ROM across the study. Lastly, future research is needed to determine which directions of the YBT are the most sensitive to dynamic balance changes in LBP populations.
CONCLUSION
The results of this study show SSEs to be more effective than GEs in improving dynamic balance, but not pain intensity nor disability level in adults with CLBP. Specifically, four weeks of supervised SSEs along with a home exercise program is more effective in improving dynamic balance than GEs in participants with CLBP in four weeks. However, GEs appeared to have an effect equivalent to that of SSEs after four weeks of supervised intervention and another four weeks of unsupervised intervention. In addition, all participants had reduction in pain intensity and disability level over eight weeks after the intervention. However, no differences were found between groups, and the decrease in pain intensity and disability level did not exceed the MCID or MDC. The results of the study provide evidence for clinicians to include SSEs for improving dynamic balance in the management of patients with CLBP.
ACKNOWLEDGEMENTS
The authors would like to thank the Texas Physical Therapy Foundation for funding this study.
DISCLOSURE STATEMENT
No conflicts of interest were present in this study.