
Background
Point of Care Ultrasound (POCUS) is commonly used in various medical disciplines to assess structures quickly and conveniently such as the heart, lungs and bladder. Musculoskeletal (MSK) ultrasound (US) is quickly growing as a non-invasive and safe manner of assessing musculoskeletal structures (bones, muscles, tendons, ligaments) without the need for expensive or potentially harmful studies such as radiograph or MRI.
MSK-US provides clinicians with a “window” through the skin to examine different tissues including muscle, bone, tendon, and ligament. In addition to structural integrity, visualizing inflammation using MSK-US may support a physical therapy diagnosis and guide appropriate physical therapy interventions. While physical therapists (PTs) are familiar with “therapeutic” ultrasound, MSK-US is not widely used by PTs. The earliest publications of MSK-US use by PTs were in the 1980s, focusing on the quadriceps muscle to describe its size.1,2 In the 1990’s, researchers and clinicians at the University of Queensland identified the activity of the deep multifidus and transverse abdominus muscles in relation to other abdominal muscles in patients with lower back pain.3,4 They discovered that the multifidus was atrophied and the transverse abdominus muscle was delayed in activation in patients diagnosed with lower back pain; they subsequently used MSK-US to provide visualization of patients for real-time feedback during rehabilitation.5 More recently, researchers reported high levels of agreement when PTs using MSK-US were compared with radiologists on 40 cadaveric shoulders.6
“Rehabilitative” ultrasound imaging (RUSI) was the term initially used to describe its use in evaluating soft tissue structures during tasks.7 Since then, 4 categories of ultrasonography have been identified in physical therapy: diagnostic, rehabilitation, interventional, and research ultrasound.8 Because these categories were only recently described, the terminology used in the literature may not be consistent; therefore, this review will follow the descriptions provided by Whittaker et al.8 In general, POCUS consists of diagnostic, rehabilitative, and interventional US; research US is used for scientific purposes:
Diagnostic US: diagnosis and monitor pathology (haemarthrosis, sprains, strains, healing stage, lesions, disease)
Rehabilitative US: evaluate muscle and other soft tissue structure and function (including biofeedback) during physical tasks
Interventional US: guide percutaneous procedures involving ‘dry’ (acupuncture) or ‘wet’ needling (injection)
Research US: measurement; explore muscle and soft tissue structure and function; develop and evaluate screening tools and interventions
Diagnostic MSK Ultrasound
Although PTs do not make medical diagnoses, they evaluate pathoanatomic structures in making a physical therapy diagnosis. Identifying structural lesions beyond the physical therapy scope of practice (such as a fracture) allows the PT to refer patients to appropriate providers if needed quickly. MSK-US has been shown to be a cost-effective measure in diagnosing structural pathologies.9,10
For some MSK conditions ultrasound has been proven to be equal to or better than MRI for accurate diagnosis of meniscal injuries,11 ACL and PCL injuries,12 Achilles tendinopathy,13 peripheral nerve injuries,14 lateral epicondylitis,15 thumb ulnar collateral ligament injuries,16–27 identifying rotator cuff tears,16–27 and supraspinatus lesions.28,29 There are several types of MSK injuries that US may not be comparable to MRI that include distal biceps tendon avulsions,30 plantar plates.31 MSK-US has also been used for the evaluation of acute athletic injury.32,33
Interest is gaining in US’s ability to view muscles both statically and dynamically.34–40 Dynamic US protocols have been published by an international group of experts to help clinicians evaluate structures while recording video during real-time patient examination to improve their understanding of their diagnosis.41–44 Dynamic ultrasound allows for real-time visualization of structures as they move in relation to other structures. For example, the movement of adjacent fascial layers can be evaluated during active muscle contraction to assess fascial mobility. Muscle architecture can be examined under contraction or relaxation for deficits.
One of the more unique properties of MSK-US that can be used to assess musculoskeletal pathology is use of Doppler imaging of blood flow. This utilizes the Doppler effect which describes the change in frequency of the sound wave that is seen as an object moves closer to (toward) or farther (away) from the transducer. The amount of movement can be seen as the Doppler shift that can be picked up on an US image using color enhancement. In diagnostic US this is usually used to determine the presence or absence of blood flow, seen with issues like deep venous thrombosis after musculoskeletal injury to the lower,45–48 and upper extremities,49 or even vascular supply to joints).50 Color Doppler imaging is also useful in detecting effusions51 and musculoskeletal inflammation such as soft tissue hyperemia.52,53
Rehabilitative MSK Ultrasound
RUSI is used to provide real-time feedback for physical therapy patients. As mentioned previously, real-time US can be used for patient feedback in re-training activation of the transverse abdominus muscle in patients with lower back pain.5 RUSI has been used to assess muscle function in screening athletes for injury risk (Hides 2016, 2017).54,55 Other rehabilitation applications include pelvic health for urinary incontinence.56,57
Interventional MSK Ultrasound
Physical therapists can integrate MSK-US into their interventions to guide treatment. Silleves et al.58 reported a case of a runner with plantar fasciitis managed with MSK-US imaging to guide decision-making for optimal treatment location and progress. As dry needling has increased in popularity among PTs, the use of MSK-US to assist with needle placement has slowly grown59,60; however, the authors of one study suggested there is no additional benefit to using US-guided dry needling with PT in chronic neck pain patients.61
Typically, interventional MSK-US is performed by practitioners giving injections. While outside the scope of practice for most PTs, MSK-US provides for accurate placement of needles for injection of anti-inflammatory medication or during prolotherapy. Recently, the technique of “hydrodissection” has been introduced in musculoskeletal medicine.62–64 During hydrodissection, MSK-US is used to guide hypodermic needles into muscle and fascia to inject saline while breaking-up adhesions and facilitating fascial mobility.
Research MSK Ultrasound
MSK-US is also used as a measurement tool for soft tissues in research. In the past, instruments to measure muscle mass included bioelectrical impedance, dual X-ray absorptiometry, computed tomography, and magnetic resonance imaging. The use of MSK-US appears to be a simple, fast, safe, valid and reliable way to measure both muscle and tendon length and thickness.65–71 In addition to length and thickness, MSK-US can also be utilized to assess fascicle or pennation angles.72
Muscle thickness can be quantified to represent muscle contraction. A systematic review in 200973 suggested that MSK-US was a valid measure of trunk muscle activation and size during submaximal isometric contractions. Recently, fascia muscle thickness has been measured with MSK-US.74–76 Tissue stiffness can be measured as well, including tendon stiffness and overall tissue tension. Shear wave elastography, for example, has been shown to be a useful measure of quadriceps tendon and muscle stiffness.77–81 Pressure applied with the transducer is compared to the movement of the tissue on the ultrasound, and the tissue stiffness is quantified with a color map.
As stated previously, MSK-US can be used to quantify blood flow in arteries and resultant hyperemia of tissues. Many physical therapy interventions purport to increase blood flow to the treated area. Arterial blood flow can be quantified with MSK-US by vessel diameter and pulse flow during exercise or after interventions.82,83
MSK-US Technology
To perform musculoskeletal ultrasound, the therapist will require an ultrasound sonography device that includes an appropriate transducer. Generally, US transducers are classified as linear or curvilinear for superficial and deep tissue sonography, respectively. Some devices such as the Butterfly IQ (Burlington, MA) use a single transducer capable of both superficial and deep sonography. The transducer is the component that converts electrical energy into sound waves. Piezoelectric crystals within the transducer produce the piezoelectric effect that allows ultrasound waves to produce an image on the screen of the device. A soundwave is created that is sent to the tissue, which is returned to the transducer.
Various frequencies of sound waves are used depending on the depth of the tissue of interest. Most diagnostic US devices have pre-modulated settings depending on the target tissue. Musculoskeletal tissues are generally more superficial, thus using higher frequencies, while deeper structures, such as the abdominal organs require lower frequencies for best visualization. The sound waves are either reflected to the transducer, absorbed by the tissue, or refracted. Ultrasound waves that are reflected from tissue create an “echo” that returns to the transducer, where the echoes are electronically transformed into digital images at various shades of black and white. The level of reflection (and thus color) is known as “echogenicity”.
Ecogenicity
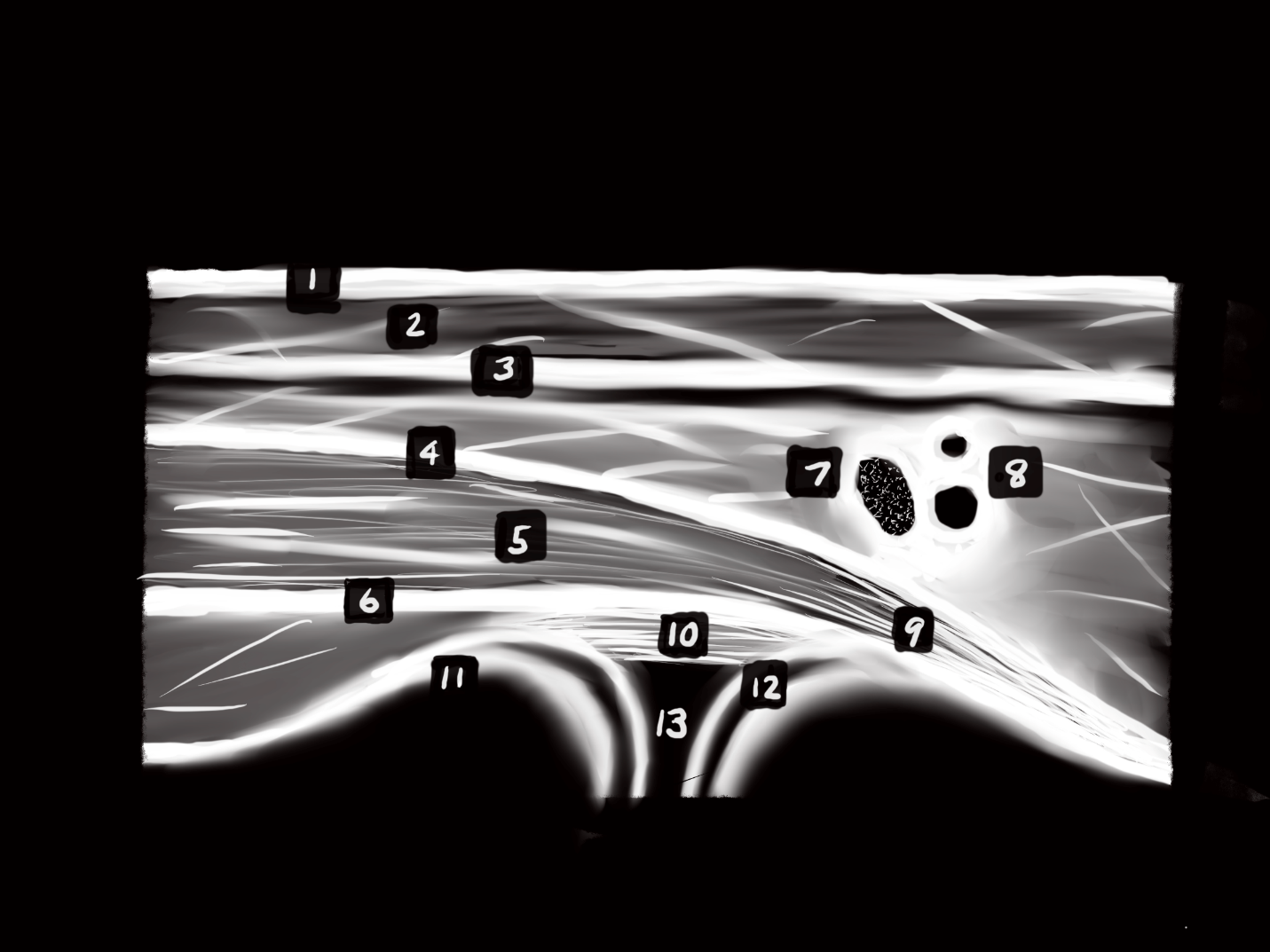
Ultrasonography measures the amount of echo from sound waves produced by the transducer at specific frequencies. Ultrasound “echogenicity” is defined as how bright musculoskeletal structures appear on an ultrasound image relative to other structures. Musculoskeletal tissues viewed on US will be either normal or pathologic tissues, and each displays a varying level of echogenicity. Structures run the gamut from hyperechoic (brighter) or hypoechoic (less bright) on imaging. Structures that are viewed as hyperechoic or echogenic are high in collagen content such as bones, normal healthy tendons, or certain calcifications in soft tissues. Nerves are hyperechoic and appear as a ‘starry night’ pattern on cross-section. A hypoechoic structure is one where the viewed structures appear darker (less white than hyperechoic structures). These structures could include fat, masses, cysts, or inflammation. A structure that is totally black is termed anechoic and usually represents fluid. For example, blood vessels appear as round, black circles in cross-section. Lastly, a structure is termed isoechoic when used to describe similar echogenicity of surrounding tissue. Table 1 provides an ‘echogenicity’ scale of tissues and Figure 1 is a general schematic of different layers of tissue viewed with ultrasound.

Sonography Technique
Generally, a gel is used to promote transmission of sound waves to and from the tissues. This is done to couple the transducer with the body part so that air is not located between the skin and device. When air is introduced between the patient and the transducer the sound waves are more easily reflected away from the structures of importance resulting in a poorer image. Ultrasound gel pads can also be used as an interface between the transducer and bony prominences to minimize artifact.
Clinicians must have a keen knowledge of regional anatomy and palpation skills to ensure proper position of the transducer over the target tissue. The transducer should be held perpendicular to the skin with the indicator directed proximal and/or lateral; this standard positioning orients the examiner with the image. Most commonly, MS-US views can be viewed in either a short axis (transverse) or long axis (longitudinal). The short axis (SAX) is performed through the transverse plane of the intended tissue, while the long axis (LAX) is performed along the longitudinal length of the tissue (See Figure 2). When possible, it is best to visualize both to get an accurate representation of the entire tissue.
_and_in_the_longit.png)
Proper technique and adequate technology are essential for an accurate diagnosis. Improper technique can lead to artifacts, which can lead to an inaccurate diagnosis. A unique artifact in MSK-US is “anisotropy” where tissues of fibrillar structure, such as tendons and ligaments, have reduced ecogenicity based on the angle of the transducer. This can result in mistaken interpretation of pathological defects.
Education & Training
Although access to diagnostic ultrasound equipment has improved in cost and convenience, the ability to perform and interpret MSK-US requires training and experience. The use of MSK-US in PT practice is supported by the American Physical Therapy Association (APTA) and is generally not prohibited by state regulations; however, reimbursement may be denied unless the PT is credentialed to perform diagnostic ultrasound as a certified and registered MSK sonography practitioner (RSMK-certified).
Several companies provide education and training on MSK-US including virtual and hands-on courses, while some manufacturers such as Butterfly IQ (Burlington, MA) provide instructional videos. SonoSim (Santa Monica, CA) provides an affordable and portable POCUS simulation that includes a ‘dummy’ transducer to provide both didactic and psychomotor skills needed for MSK-US. Several excellent textbooks are available specific to MSK-US as well.84–86
Conclusion
Physical therapists have an opportunity to embrace technology and integrate MSK-US into their practice. Emerging research continues to support its use in PT for a variety of patients, including diagnosis, treatment, and research.