





INTRODUCTION
The number of revision hip arthroscopic surgeries is increasing substantially, due in part to the increasing number of initial arthroscopic labral repairs.1 In the last five years, there has been a significant increase in the overall number of arthroscopic hip surgeries, and the number continues to rise.2 As such, revision surgeries are becoming more frequent, with research indicating between 4-10% of initial cases will need a revision surgery.1–3 The mean time between primary labral and revision labral surgery is approximately two years.4,5 The most common indications for revision surgeries are residual bony impingement,4–9 labral tears,4–6,8,9 chondral lesions,5–7 micro-instability,5,9,10 and excessive scarring.4,5,8,9 Preoperative imaging studies show that nearly 80% of those seeking revision hip arthroscopy (RHA) surgery have signs of remaining bony impingement.4–9 Micro-instability can occur as a result of femoroacetabular impingement (FAI), soft-tissue deficiencies, such as labral insufficiency following debridement, capsular resection, or over-resection of bony impingement.9–12 Micro-instability may be a pain generator due to excessive physiologic motion and can put the capsule and labrum at risk for further injury.10–12
Studies investigating the outcomes of physical therapy following hip arthroscopy for labral pathology are limited.13 Thorborg and colleagues reviewed outcomes at one year post-operatively and found clinically relevant and statistically significant changes in function following post-operative rehabilitation for FAI and labral pathology. However, the patient related outcomes still fell behind those of healthy individuals.14 One review found that less than 30% of surgeons performing hip arthroscopy had an associated rehabilitation protocol given to patients.15 Of these protocols, use of bracing, weight bearing status, range of motion (ROM) precautions and limitations, and return to activity timelines varied significantly.15 When no residual bony impingement is present the variations found in both surgical and rehabilitative approach and treatment may be contributing to suboptimal outcomes following primary hip arthroscopy.
The utilization of criteria-based protocols to aid progression of rehabilitation is growing in popularity in other areas of orthopedics. In the anterior cruciate ligament (ACL) population, utilization of a criteria-based progression has been shown to reduce risk of reinjury four-fold.16,17 Following a shoulder stabilization procedure, significant numbers of participants did not pass criteria testing at the expected time of “recovery”.18,19 The use of criteria-based progression versus time-based progression throughout rehabilitation should help to minimize the discrepancy in readiness for return to activity due to regular assessment of patient progress. These progressions can ensure patients move through each phase of rehabilitation and meet specific goals related to motion, neuromuscular control, and strength. The unique difficulties following RHA surgeries can differ from the traditional rehabilitation process and challenge the rehabilitation professional.
Previous clinical commentaries have outlined rehabilitative guidelines for those following primary labral reconstruction or repair, and although these studies present an excellent and thorough framework, they do not consider the additional factors that impact revision labral surgeries.20 This clinical commentary attempts to highlight the differences and present guidelines that are both criterion-driven and time-based to ensure consideration for the individual as well as the complexity of the surgical procedure. Therefore, the purpose of this clinical commentary is to propose a criterion-based progression that considers the intricacies present following a hip revision arthroscopy from early rehabilitation through return to sport.
Femoroacetabular impingement
The primary anatomical considerations that contribute to labral pathology are attributable to femoroacetabular impingement (FAI).21,22 FAI is caused by the abnormal morphological anatomy that changes joint contact between the head/neck of the femur and the margin of the acetabulum.22 As such, the presence of FAI may be correlated with chondral and labral damage in patients with hip pain.21 There are three main types of FAI: cam impingement, pincer lesions, or combined impingement.22 Cam lesions consist of a non-spherical femoral head which can lead to impingement during flexion. This impingement in flexion may cause labral tearing or avulsion from the acetabular rim and potentially damage to the acetabular cartilage.22 Pincer impingement is typically due to acetabular overcoverage, sometimes in conjunction with coxa profunda or acetabular retroversion. This type of lesion typically presents with degeneration of the acetabular labrum and potential ossification of labral tissue as well as chondral damage on the femoral head/neck.22 A combined impingement is consistent with both a cam and pincer pathology which can lead to damage of the acetabular labrum and chondral damage on the acetabulum and/or the femoral head/neck.22 These bony abnormalities can cause and often coincide with capsule, ligament, and muscular dysfunction which often results in abnormal stress and forces through the hip joint.23 Some examples of concomitant pathologies associated with FAI are anterior inferior iliac spine (AIIS) impingement, Iliopsoas impingement, athletic pubalgia, and tearing of the ligamentum teres.23,24 Primary hip arthroscopy is utilized to address these potential bony abnormalities, larbral and/or chondral damage, and associated soft tissue pathology as needed.
REVISION SURGICAL TECHNIQUE
RHA surgeries of the labrum are focused on restoring the suction-seal mechanism and restoring the biomechanics of the hip joint.25,26 This added stability helps decrease the compression forces during hip motion and protects the articular cartilage.27,28 In most revision cases, there are adhesions between the labrum and the capsule that need to be addressed at the time of surgery.29 Whether to repair, augment, or reconstruct the labrum during a RHA depends on the quality of the labral tissue.
If there are minimal adhesions present and the labral quality is good, then any retear or new tear of the labrum can be addressed as in a primary setting. However, in cases of a deficient labrum where a repair is not possible (i.e., hypotrophic labrum, irreparable segmental defect, ossified labrum) then a labral augmentation or labral reconstruction is needed. If circumferential labral fibers are present, then a labral augmentation is preferred to reconstruction as this preserves the innervation of the labrum and the vascularization, which is important for graft healing.1 In cases where the circumferential labral fibers are not present, a labral reconstruction (either segmental or complete depending on the size of the defect) would be needed.26 These grafts can be made with either autograft or allograft tissue.26
Regardless of the labral surgery performed, any concomitant pathology must also be addressed during the RHA.26 Most commonly, this would include additional osteoplasty for under-resection in femoroacetabular impingement, a remplissage technique for over-resection for femoroacetabular impingement, addressing chondral defects, lysis of adhesions, or repair or reconstruction of a capsular defect.29 The remplissage technique utilizes surrounding soft tissue such as the Iliotibial Band (ITB) or Tensor Fascia Latae (TFL) musculature to fill in areas of over-resection, particularly after resection of a cam deformity.30 The abundant blood supply of the capsulolabral recess predisposes that region to adhesions and in cases of patients with significant adhesions, a “spacer graft” between the labrum and the capsule (similar to an augmentation) may be needed to prevent further adhesions.31
POST-OPERATIVE REHABILITATION
Following RHA surgery, the use of a criteria-based progression to advance through rehabilitation phases is proposed and described herein. The criteria-based progression focuses on specific goals to ensure readiness for more progressive loading and flexibility for the revision hip population. Similar to rehabilitation after primary hip arthroscopy, a five phase rehabilitation program is proposed to include: Protection, Endurance, Strength, Power, and Return to Participation/Sport.32
Phase I: Protection
The primary goals of Phase I are protection of healing tissues (bracing, ROM precautions, and load management), symptom management (inflammation and pain), maximize range of motion (ROM) within surgical precautions to reduce adhesion formation, initiate muscle activation, and return to general wellness baselines (sleep, energy, mood, and nutrition).
Surgical restrictions following RHA vary significantly between surgeons and procedures. It is important to ensure surgical precautions are followed as per individual protocol. The range of motion expectations at this point are similar to the typical restrictions seen following primary. Extension and external rotation (ER) are limited to decrease tension on the healing anterior capsule, labral repair, and to protect the incisions. Active hip flexion is also limited to reduce stress of the hip flexor muscles.33 Weight-bearing during this phase is reduced to protect the repair, and the amount varies with surgeon’s discretion. Compared to a primary labral surgery, the time of restricted weight-bearing may be extended, especially if a micro-fracture is performed. Table 1 portrays some of the frequent surgical restrictions that are seen by the authors. These restrictions are utilized to guide and modify appropriate exercise selection in the early phases of rehabilitation. The restrictions of ROM, positioning, and weight bearing are all incorporated to protect the capsule, reduce stress on the repair, and reduce stress on the joint. Additionally, each of these restrictions and limitations is highly individualized to the patient and particularities of each case and as such, exist on a continuum. Due to the general variability in surgeon preference it is highly encouraged that the progression of range of motion, weight bearing restrictions, and exercise selection is based on post-operative restrictions individualized to each patient.
Symptom management should focus on controlling pain and reducing inflammation. With lengthy revision surgeries, post-operative joint effusion can be a significant issue. This can cause pain and impact muscle activation via arthrogenic and neurogenic inhibition.34 Manual therapy techniques including lymphatic drainage massage can be used to help manage post-operative swelling.35–37 The lymphatic system plays a big role in removing excess interstitial fluid and returning this fluid to the circulatory system. The use of continuous passive motion can help facilitate a pumping action, by creating a sinusoidal oscillation in intra-articular pressure, which will aid in moving blood and edema fluid away from the joint and periarticular tissues.38
Following suture removal, scar mobilization can be beneficial to manage pain and to prevent adhesion formation that may impact ROM and pain in later stages.39 Utilization of passive circumduction is standard for early post-operative care due to its propensity to reduce scar tissue formation. Research has shown there to be a 4.1x increase in scar tissue formation in hips that do not receive circumduction.40 The use of the medication Losartan has become more common following hip procedures to ameliorate cartilage deficits41 and reduce postoperative fibrosis via the blocking of transforming growth factor Beta-1.42 Figure 4 shows an early stage exercise to introduce ROM.

The gluteal muscles are essential in pelvic control during gait and single leg stance. Seventy percent of the abductor force required to maintain pelvic stability in the frontal plane is provided by muscles that insert into the greater trochanter.20 The maximal hip extension ROM achieved during gait is shown to increase the forces on the anterior hip joint.43 Consequently, general decreases in force output from the gluteal muscles during extension and the iliopsoas muscle during flexion causes an increase in anterior hip joint forces.44 A solid foundation of good gluteal maximus, medius and minimus muscle activation and control during Phase I is important, before initiating endurance and progressing gait training. Figure 2 is an exercise utilized once weight bearing restrictions are lifted to promote gluteus maximus activation.

There is controversy regarding compensation patterns and movement dysfunction in rehabilitation.45 Do they cause pain and dysfunction or are they normal variations of human movement? Alternative neuromuscular strategies are commonly observed in individuals with mechanical hip pain and patients post hip arthroscopy.23 In particular, weakness of gluteus maximus with overactivation of hamstrings and lumbar extensors, weakness of gluteus medius with overactivation of tensor fascia latae are often observed in this population. Additionally, weakness of the deep hip rotators and anterior core is often seen.46–48 Individuals undergoing revision surgery have spent months if not years experiencing hip pain, which conform with compensatory movement patterns and hip muscle weakness.2 Being aware of these patterns is important both for the clinician and the patient. An easy way to incorporate the patient into discerning these compensatory patterns is by using subjective assessment of work or fatigue during a task. This can help to tie in the patient’s attention to movement while also incorporating awareness into their exercises by use of internal feedback.
Exercises commonly used during this phase are geared toward both protecting the repair and gradually reintroducing active hip-based movements, within the restrictions of the surgeon. Table 2 highlights exercises utilized throughout the rehabilitation process. The Phase I column in Table 2 presents suggested exercises with the main focus being correct muscle activation during the exercise, starting with active-assisted and moving to active range of motion as the patient is able to re-establish adequate neuromuscular control. Active hip flexion can commence after two weeks due to tissue healing guidelines. Although commonly perceived as overused in hip pathology, the psoas muscle is important in hip flexion and requires adequate strength to perform daily tasks.43 Figure 3 portrays the hip roll exercise which is integrated to promote psoas activation. In this figure, the patient is palpating their hip flexor muscles. Based on anatomical location and insertion, activation of the more laterally based muscles would be considered more rectus femoris bias while activation of flexors located more medial would be considered more psoas. Although isolation of the psoas is unlikely, this exercise is used to promote submaximal activation of both a commonly weak and potentially overused muscle in hip pathology.43

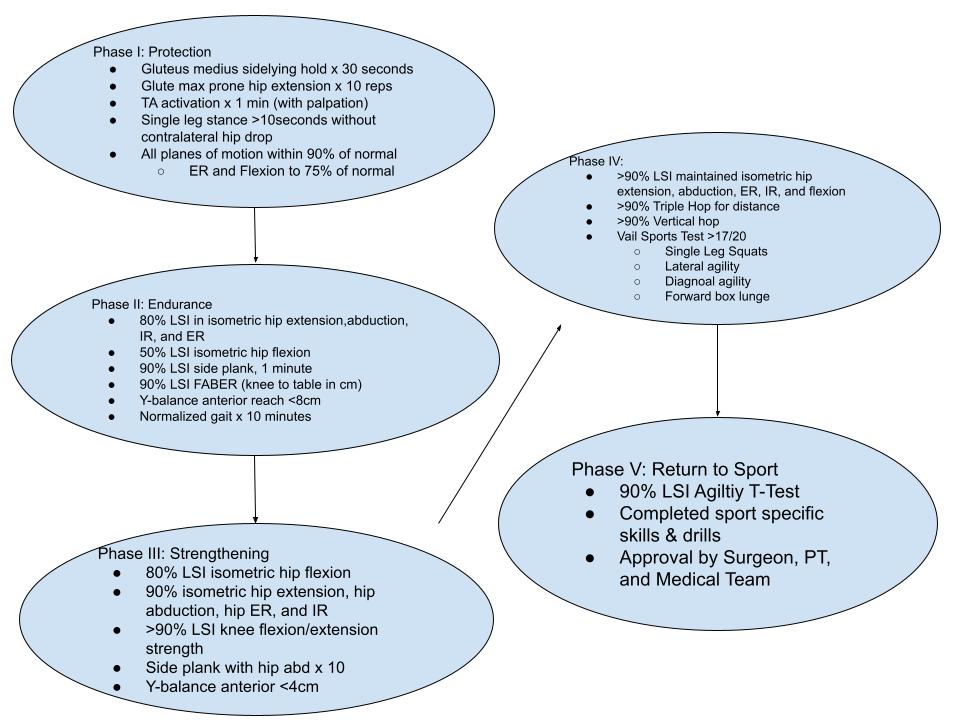
Located in Figure 4 is a flowchart highlighting criteria to progress between the five phases proposed in this commentary. The criteria to progress to Phase II requires appropriate muscle activation, pelvic control in single limb stance and adequate ROM of the hip necessary to progress gait and perform functional movement tasks in the endurance phase. The ROM criteria are set to allow for appropriate functional motion with walking and transitional movements such as sit to stand.20 The ROM expectations for ER and flexion are less due to typical surgical restrictions placed upon these motions in early rehabilitation.33 Prone hip extension, TA activation, and the gluteus medius side lying hold tests allow for assessment of muscle function that is less aggressive than dynamometer testing, which is inappropriate at this stage of healing.20 These particular tests are chosen to assess for gluteal activation and core stability in early rehabilitation, as they will set the stage for more dynamic strengthening later and their correct performance will determine compensatory patterns that may be present in hamstring, latissimus dorsi, or hip flexor muscle groups.20 Single leg stance testing is utilized to assess the ability of the lateral hip muscles in achieving a neutral pelvis on one limb, necessary for gait.20

Phase II: Endurance
Phase II, or the endurance phase, focuses on the introduction and improvement of muscular endurance for the ability to perform activities of daily living (ADLs) without pain or dysfunction. These dysfunctions could involve movement deviations and/or compensations. The main goals for this phase are normalizing active ROM (AROM) compared to the non-injured side, building endurance in hip musculature to allow progression to full weight-bearing with a non-antalgic gait pattern, and reestablishing tolerance to joint and tissue loading in preparation for future strength exercise progressions in Phase III. Exercises should be provided in an endurance set-rep scheme with three sets of 15-20 repetitions, performed two to three times per week.49 Continuing to focus on neuromuscular re-education is paramount for the hip revision population in order to deconstruct pre-surgical compensation patterns and promote ideal muscle firing pattern for the hip complex that were established in Phase I. Initiating cardiovascular and work capacity training is also important in this phase.
Following RHA, the flexion, abduction, external rotation (FABER) position can be utilized to slowly integrate functional ER ROM and to reintroduce a previously irritating position. The FABER test is utilized to assess soft tissue restrictions in the anterior hip. Tissue tone or guarding of the psoas can be seen in ER or FABER positioning and may be symptomatic for some patients. Use of gentle contract-relax from proprioceptive neuromuscular facilitation (PNF) concepts can integrate reciprocal inhibition to reduce psoas or TFL guarding. Gentle joint mobilizations are another technique to help neuro-modulate the hip joint following revision surgery.50 Ensuring a restriction is capsular as opposed to bony should be established before utilizing higher grade mobilizations in this population.51 Assessing internal and external rotation ROM both in positions of capsular tightness and muscle tension (hip extension versus hip flexion) should help to determine discrepancies in motion that would bias capsular restriction versus ROM restriction. Manual therapy techniques can be utilized in the neuromuscular re-education process to address muscle hypertonicity, pain, and dysfunction. Pain and tone in the adductors, psoas and TFL can be present and may affect progress in this phase of post-operative rehabilitation if overlooked.
Normalizing gait to ensure functional ambulation for the patient to return to typical ADLs is essential during this phase. When progressing weight-bearing, respecting surgical precautions and gradually reintroducing weight to the joint is paramount. The use of scales is common to incrementally introduce a percent of body weight while using crutches to desensitize the joint to external forces. Slow progression from two crutches to one crutch over multiple weeks may be necessary to avoid rebound inflammation, pain, and gait dysfunction. The use of pool walking, aquatic treadmills, Alter-G treadmills, and the TRXⓇ can be used to systematically increase load on the joint. This, in particular with hip revision cases, is important to allow the joint adequate and individualized time to adjust to body weight. Patience during this phase can be the difference between appropriately training the hip complex muscles to accept load during functional activities and perpetuating long-standing compensatory patterns. It is paramount that criteria-based progression be used in gait training versus time-based progression due to the variability in crutch weaning time.
During this stage, integration of neurocognitive challenges to single leg balance, lateral and posterior hip strengthening progression, and deep rotator strengthening is valuable. Refer to Table 2 for the exercises included in this phase. Resistance should be added to open kinetic chain exercises and once adequate lower extremity strength and proximal stability has been restored the addition of closed kinetic chain exercises should be introduced. This will prepare the hip joint to accept heavier loads in the later phases. Additionally, monitoring the degree and location of fatigue as well as undesirable signs and symptoms of overuse during a task can help to prevent delays in recovery and symptom exacerbation.
A key point of Phase II is returning to performing ADLs. Educating patients on how to best micro-dose their ADLs to promote function and minimize micro-inflammation during this phase is crucial for hip revision patients, who often cannot tolerate even minimal activity. This particular point can be guided by subjective symptoms or fatigue. Significant education regarding spacing activities over the course of a day or over multiple days rather than performing the entirety of a task is encouraged. The goal is to minimize micro-inflammation which can cause arthrogenic inhibition, while progressing capacity for load tolerance. Gaining independence with ADLs and gait can be a big accomplishment for RHA patients and achieving this milestone should be acknowledged. However, further advancement and new goals should be made. It is important they continue to progress with strengthening in order to create healthy habits and increase their chances of preserving their hip function.49 An in vivo study by Bergmann et. al,52 showed that the average person loaded their hip joint at 238% body weight while walking at 4km/h, 251% with climbing stairs, and 260% with descending stairs. Giarmatzis et. al,53 and Luepongsak et. al,54 have shown that changes in gait speed and running can increase hip joint forces. Achieving superior strength is important in dissipating these forces and maximizing long term outcomes following RHA surgeries and will be addressed in the next phase.
Refer to Figure 4 for the criteria for progression from this phase. These tests aim to ensure adequate muscular strength in the gluteal complex and hip flexor muscles. All isometric testing is done utilizing hand held dynamometry (preferred) or by achieving a 4 strength grade using manual muscle testing in standard positions. The lateral trunk endurance test is a reliable and valid measure to assess core stability, pictured in Figure 5.55 The anterior reach of the Y-Balance test has been shown to have predictive validity for injury occurrence across adults and athletes alike, particularly if side-to-side discrepancy is >4cm. However, these studies are not specific to the hip population.56,57 In the authors’ opinion, at this stage of rehabilitation a < 8cm difference is utilized as an achievable measurement to begin assessing symmetry in dynamic balance, and this will be progressed upon in the next phase. All of these components set the stage for strengthening, by establishing an adequate muscular base of strength, endurance, and neuromuscular control.

Phase III: Strengthening
The strength phase, or Phase III, focuses on increasing load and building strength in the muscles of the lower extremity and core. At this stage of rehabilitation, exercise prescription should be changed according to strength parameters. Exercises should be performed in 3-6 sets of 3-5 repetitions at a higher load, 60-80% of one rep maximum for novice to experienced individuals respectively.49
Table 3 ranks exercises based on percentage of maximum voluntary isometric contraction (%MVIC) for gluteus maximus and gluteus medius strengthening, and it is recommended they are included in this phase of rehabilitation. Neuromuscular activation of 40-60% MVIC is recommended as a minimum for a strengthening effect59 while around 70% MVIC is thought to elicit an optimal strengthening effect and achieve desired adaptations in muscle morphology, such as hypertrophy.58 However, the use 1RM can be difficult and potentially unsafe to achieve and assess in the rehabilitative setting. In a recent meta-analysis by Lea et.al, rate of perceived exertion (RPE) has been shown to be a valid measure of exercise intensity and exertion.60 As such, utilizing RPE can be monitored to ensure sufficient load is being applied. Considering this information, a 60-80% intensity of 1RM can be estimated at about 6-8/10 or 14-17/20 using an RPE scale.60 Introduction of rate of force development (RFD) during these exercises in the later stages of Phase III can help build confidence with moving faster and without fear. Utilizing speed in exercise tasks can promote this RFD bias. RFD correlates to maximum voluntary contraction in the early phase of a contraction, requires increased discharge at the motor unit, and can be developed by heavy resistance training.49 By improving the RFD in this phase, it helps to set the stage for power training in phase IV.
The criteria for progression to Phase IV are referenced in Figure 4. Achieving adequate strength of the muscles of the hip complex, compared to the non-injured limb (limb symmetry index), to assess muscular function is important to prepare for the power phase. Maximized strengthening of both internal and external rotator muscle groups is important in the homeostasis of the hip, with particular research supporting the deep external rotators, although a specific ratio has not been confirmed. Tateuchi et al.61 showed increased anterior hip joint forces in the deep squat when weakness in the deep external rotators was present. Meinders and colleagues showed that maximal activation of the deep external rotators resulted in decreased hip contact force angles and reduced acetabular loading.62 Examples of exercises for these muscle groups are seen in Figures 6 and 7.


The side plank with hip abduction (Figure 5) is shown to have the highest studied gluteus medius recruitment (103% MVIC).58 As such, utilization of the side plank with hip abduction test allows good understanding of the patient’s ability to recruit the gluteus medius which has direct impact on ambulation and more advanced activities such as running and jumping. Upon completion, this phase should allow for significant functional improvements and a return to low intensity exercise and functional tasks without pain or dysfunction.63
Phase IV: Power
Phase IV, or the power phase, is the last required phase before fully allowing patients to return to light impact-based activity. Continuing into this phase is highly dependent on three factors: (1) number of hip surgeries & revisions, (2) patient expectations, and (3) surgeon expectations. These three factors will help to determine the necessity to progress to a power-based phase and to plan for appropriate expectations following RHA surgery. Should all three of these factors align and Phase III criteria have been met, it is anticipated the individual will have established good neuromuscular control, adequate strength, and the ability for the hip joint and surrounding tissue to accept load without exacerbation of hip pain.
In the author’s experience, in cases of multiple revision surgeries the history of muscular inhibition and compensatory patterns, aberrant joint loading, and the psychosocial factors increase the difficulty in returning to high level activities, and as such expectations should be modified. Presence of joint line space <2mm has been shown to have poor longevity after RHA and a higher probability of total hip arthroplasty/replacement in the future.64,65 Discussion with the medical team regarding joint space narrowing and history of microfracture may be a valuable tool in deciding whether return to higher intensity activities is advisable.64,65 Additionally, psychological readiness scales can be utilized to assess patient’s expectation and to help clinicians in making appropriate and informed decision regarding to sport and participation in later stages of rehabilitation.66 Similar to the earlier phases, the exercise prescription in this phase should also change in conjunction with normal power guidelines.49 Exercises are performed under light to moderate loads, with a prescription of 3 sets of 3-6 repetitions and an emphasis on rate of force development. Power exercises should be scheduled 2-3 times per week and within a session, performed before strength exercises.49
Power exercises apply the maximum amount of force as fast as possible on the basis that force times velocity equals power.49 This training can take many shapes, but during rehabilitation it is important to start slowly and gradually increase speed and load. Plyometric exercises are often a good starting point and can be easily modified to accommodate patient anxiety. Plyometric progression should start with double leg exercises that minimize impact such as use of a shuttle press or TRXⓇ system which can promote a lengthened amortization phase initially and gradually challenge speed as patient comfort and mechanics improve. As tolerance improves, challenging overall load by increasing external resistance and then progressing to jump-down landings can be utilized for improving power. Sagittal plane jumping movements are progressed to frontal and multi-planar movements. Once adequate tolerance to double leg jumping is established without concern, progression to single leg loading such as single leg bounding or hopping can be incorporated. It is necessary to have established good control in jumping at or above full body weight prior to progressing to bounding or hopping. Continued strengthening is important in this phase, and increasing load as tolerated can be an efficient way to increase power.49
Figure 1 shows the progression criteria for the Power Phase. Unique to this progression are components of the Vail Hip Sports Test (VHST) which utilizes testing components that attempt to load the hip in typical impingement angles to assess overall tissue load tolerance and movement patterns.67,68 The four test components include: single knee bend, lateral agility test, diagonal agility test and forward lunge onto box test.67 Additionally, performance on the VHST has been shown to be correlated with hip extension and external rotation strength.68 Triple hop and vertical hop tests have both been shown to be reliable tests following ACL reconstruction and can be adapted for other lower extremity conditions.69 Hop tests are convenient and reproducible in most clinical settings for discerning power differences between lower extremities.69
Return to Sport
Progression to this phase is individual and highly variable in this patient population. This decision is based on prior history, complexity of surgical procedure, recommendation of surgeon and team, and personal goals of the patient. If performed strategically, this phase can be very attainable despite revision status. In the case of clearance from the full medical team, the suggestion is to ensure greater than or equal to 90% limb symmetry index (LSI) in strength testing and power testing, as outlined in the previous Phases. The agility T-test is added due to its validity and reliable in assessing lower extremity speed, leg power, and agility.70 The agility T-test, strength LSI, power LSI, quality of motion during these tests along with clinical decision making by the health care team will help ensure safe return to sport following hip labral revision surgery. Communication with the patient, coaching staff, medical staff, and strength coaches should be utilized to establish a smooth transition of both load and sport specific training. Ideally, slow integration of sport-specific exercises should be introduced into late stage rehabilitation and increasing difficulty implemented as mastery is achieved. A general guideline should start with sport-specific tasks in isolation, non-contact drills, contact drills, scrimmage or practice situations, and eventually a return to unrestricted competition. Full description of the return to sport phase is beyond the focus of this commentary.
Psychological Considerations
Dick, et al. and Chang et al. show a strong correlation between mental health and hip pathology.71,72 Evidence suggests that history or presence of mental health issues negatively impacts outcomes following FAI surgery.71,72 Presence or history of mental illness may have contributed to previous failed hip labral procedures, and although it cannot be assumed as a reason for failure, it may be a contributing factor in the rehabilitation process. Additionally, Dick et al., and Cheng et al. show that consideration for the presence of mental health issues following hip labral repair may prepare the clinician for the potential presence of persistent pain in both early and late rehabilitation post-operatively.71,73 Browning and colleagues showed that patients with pain catastrophizing and kinesiophobia following arthroscopic hip surgery had poor RTS outcomes at one year.74 The use of psychological readiness scales throughout rehab may help to assess areas of fear avoidance or anxiety regarding RHA rehabilitation and return to prior levels of function. Recently, the Hip-RSI, a modified version of the ACL-RSI, has been proven to be both valid and reliable in assessing psychological readiness following hip arthroscopy.66 The Short Form-36 and Tampa Scale of Kinesiophobia66,75,76 are additional options to evaluate fear of motion, although not specific to post-operative hip surgery.77 In addition to the use of validated outcome measures, the incorporation of pain neuroscience education may be helpful in addressing and assuaging fears and habits that may negatively impact rehabilitation.
Another component of rehabilitation for the RHA patient is the importance of self-efficacy.73 Albert Bandura defined self-efficacy as the perception of one’s ability to succeed in a specific situation. Jochimsen et al.73 found that poor self-efficacy has been shown to correlate with higher pain levels. There is evidence that also suggests that high self-efficacy can improve adherence to a program, improve physical function, and decrease pain.73,78 Thus, as healthcare workers utilizing discussion of vicarious experiences, persuasion, and even positive reinforcement to maximize a patient’s perception of efficacy during their rehabilitation may be important. The referral to a psychologist can be an invaluable tool to address any psychological concerns present throughout rehabilitation.
CONCLUSION
When considering the typical difficulties that those who undergo RHA experience, the proposed criteria-based progression allows for patient individualization throughout the course of therapy. With a history of multiple hip labral surgeries, the timeline for recovery may lengthen and vary based on the complications that may be present. By removing the time-based criteria traditionally seen post-operatively, and utilizing a criteria-based progression, we can assist patients to be better equipped to achieve the motion, strength, stability, power, and function for returning to their maximum potential. The criteria proposed in this commentary is a working guideline to encourage the clinician to perform regular assessment of motion, endurance, strength, and power as tissue healing occurs and progress based upon suggested criterion.
Acknowledgements
The assistance of Kristyn Petracek, Jenna Hodge, Meghan Gallegos, Brett Mueller, and Devyn Kammert for their contribution to this project is gratefully acknowledged.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no conflicts of interest.