INTRODUCTION
Major League Baseball (MLB) is the professional baseball league in North America representing 30 teams in the United States and Canada.1 Standard season format consists of six weeks of preseason spring training, 162 game regular season, and a ten team post-season format.1 Over the course of a typical season, injury incidence rates have ranged between 0.7-5.13 per 1000 athlete exposures (AEs) across all positions.2–4 These injuries result in significant league wide missed playing time and monetary losses; previous analyses have estimated the cost of placing players on the disabled list to be between $136-695 million per year between 1998 to 2015.5 Due to the physical and financial burden associated with MLB injuries, baseball stakeholders including coaches, owners, players, and clinicians have sought to mitigate injuries.6 A systematic approach to injury prevention research has been suggested by van Mechelen, beginning with injury surveillance to increase understanding of incidence rate over time.7
In contrast to the standard season layout, the 2020 MLB season format was disrupted due to the COVID-19 pandemic. Pre-season spring training was cancelled and four months later resumed in a condensed two-to-three-week format.8 The regular season was condensed to a 60 game schedule over two months, with an expanded 16 team post season schedule. This schedule adjustment increased the number of double headers played within the season and decreased the number of rest days.8 Disruption to pre-season training, inconsistent training regimens, isolation requirements for players who tested positive for COVID-19, decreased equipment access, and increased schedule density8 likely impacted players ability to manage training and playing loads.9 One study investigating injury incidence during the COVID-19 shortened MLB season demonstrated an increased injury incidence rate compared to the previous season (2020 season: 8.66 per 1000 AEs; 2019 season: 5.13 per 1000 AEs).3 Previous studies across multiple professional leagues including the National Basketball Association,10 National Football League,11,12 European professional soccer leagues,13 have also reported an increase in injury rates during the 2020 shortened season. However, most of these studies reported comparisons to a single previous season. Sparse information is available on previous five season data, which may be more representative of injury rate (IR trends), or on the subsequent 2021 season to determine if IR stabilized the following year. Furthermore, previous injury surveillance literature among professional leagues during the 2020 COVID-19 season reported injuries based on anatomic zones3 versus recommended standardized reporting by body region/area,14 or reported on a single pathology,11 making comparison to previous literature difficult.
One way to identify injury incidence among MLB players is through publicly available data.15–17 Publicly available data improves transparency, and allows for collaboration among organizations to improve data robustness and distribution among stakeholders.18,19 This transparency and collaboration amongst organizations is essential to promote an open science environment.20–22 An open science approach allows researchers to independently assess, reproduce, and perform studies for further independent research with data that is easily accessible.20,22 Publicly available data is an example of data that is in line with this open science recommendation, and has been utilized across professional leagues with a high reporting reliability.15,23 Publicly available data is accessed through a computer iterative repeatable process which involves an automated collection of information from webpages, an efficient method of data extraction.15,24 This process improves repeatability, and offers the potential for collaborative league wide injury risk identification and injury mitigation programs.15 The primary aim of this study was to use publicly available data to compare injury rates during the 2015-2019 seasons, COVID-19 shortened season (2020), and the 2021 season stratified by body region and position (pitchers versus position players).
METHODS
Study Design
This was a retrospective cohort study among MLB players utilizing publicly available data through a computer iterative reproducible method18 that has been previously described.15,17 Two data repositories were used to create a data set for this study (Supplemental File 1). The data can be accessed through the Open Science Framework data repository https://osf.io/5akxt/. MLB stakeholders (coaches, sports medicine clinicians, and performance coaches) were included to aid in development of the research question and clinical interpretability of the results. This study was reported following the Strengthening the Reporting of Observational Studies in Epidemiology for Sport Injury and Illness Surveillance (STROBE-SIIS) guideline.14
Participants
Participants were MLB players 18 years or older who competed in at least one season between 2015 to 2021 seasons. For subgroup analyses, players were labeled as a pitcher (starters, middle relievers, relievers) or position player (infield, outfield, catcher, designated hitter) for injury incidence comparisons.
Injury Classification
Injuries were included in this study that occurred from the first game of the regular season to the last game of the post season during team sanctioned events, including games or practices. Injuries that occurred during the preseason or off-season were not included due to inconsistencies observed in the data and inability to corroborate if injuries occurred during team sanctioned events. Injury was defined as any tissue damage or derangement of normal physical function that occurred during a training session or competition that resulted in time loss of one or more days.25 Injury was defined based on a specific joint or body segment as recommended by STROBE-SIIS body region and area guidelines.14
Athlete Exposure
Seasons were defined as 2015-2019 season, COVID-19 shortened season (2020), and 2021 season. Athlete exposure was calculated based on game exposure (AGE) only as determining practice exposure was not possible with this data set. For the 2015-2019 seasons, AGEs were calculated based on all 30 MLB teams playing 162 regular season games per season, 25-man active roster, over the five seasons.3,4 For 2020 season, rule changes to roster size took effect two weeks into the season.3 Thus, AGEs were calculated based on 30 MLB teams playing 60 regular season games, a 30 man roster the first two weeks, 28-man roster the second two weeks, and a 26-man roster for the remaining weeks of play.3,4,8 For 2021 season, AGEs were calculated based on 30 MLB teams playing 162 regular season games per season and a 26-man roster. For all seasons, a postseason exposure adjustment was included to account for post season injuries based on the number of playoff games that occurred each season, with a reduction in the number of active players as teams were eliminated.26
Data Extraction, Data Reduction and External Validation
For a detailed description of data repository used refer to Supplemental File 1. Data were extracted on November 3, 2021. Data extraction, data reduction, and external validation used have been previously described.15,17,25 External validation was performed by two independent examiners using a number generator, randomly selected 100 data points from the data set. External validation was performed for date of injury and injury type for each selected player from other publicly available websites (i.e., ESPN.com, mlb.com, team websites). 83% of randomly selected records were confirmed in outside reports demonstrating excellent reliability for injury reporting. Refer to Supplemental File 1 and 2 for detailed methods and data extraction code.
Statistical Analyses
Injury and illness count data was converted to seasonal incidence rate (IR). IR was calculated by sum of injuries and divided by the sum of player-games, multiplied by 1000 x Athlete-Game Exposures (AGEs)17 and adjusted for number of regular and post-season games each year.26 IR for overall injuries for in-season time frame was calculated by adjusting for monthly AGEs. Rate ratios (RR) were calculated by specific position incidence rate (pitcher or position player) and divided by all other position incidence rate for pre 2015-2019 seasons, COVID-19 shortened season (2020), and 2021 season. A Poisson Regression was performed to investigate the potential differences in injury rates between season time frames (2015-2019; 2020; 2021). AGE was used as an offset for the model to control for differences in athlete exposure each year. Poisson models were performed for all injuries and stratified by position (pitchers and position players). Additional exploratory models were performed on the most commonly injured body regions, including the shoulder, elbow, and groin/hip/thigh region and stratified by position. All analyses were performed in R version 4.1.3 (R Core Team, 2020) using the rvest, tm, and xm12 packages.
RESULTS
Injury Incidence All Positions
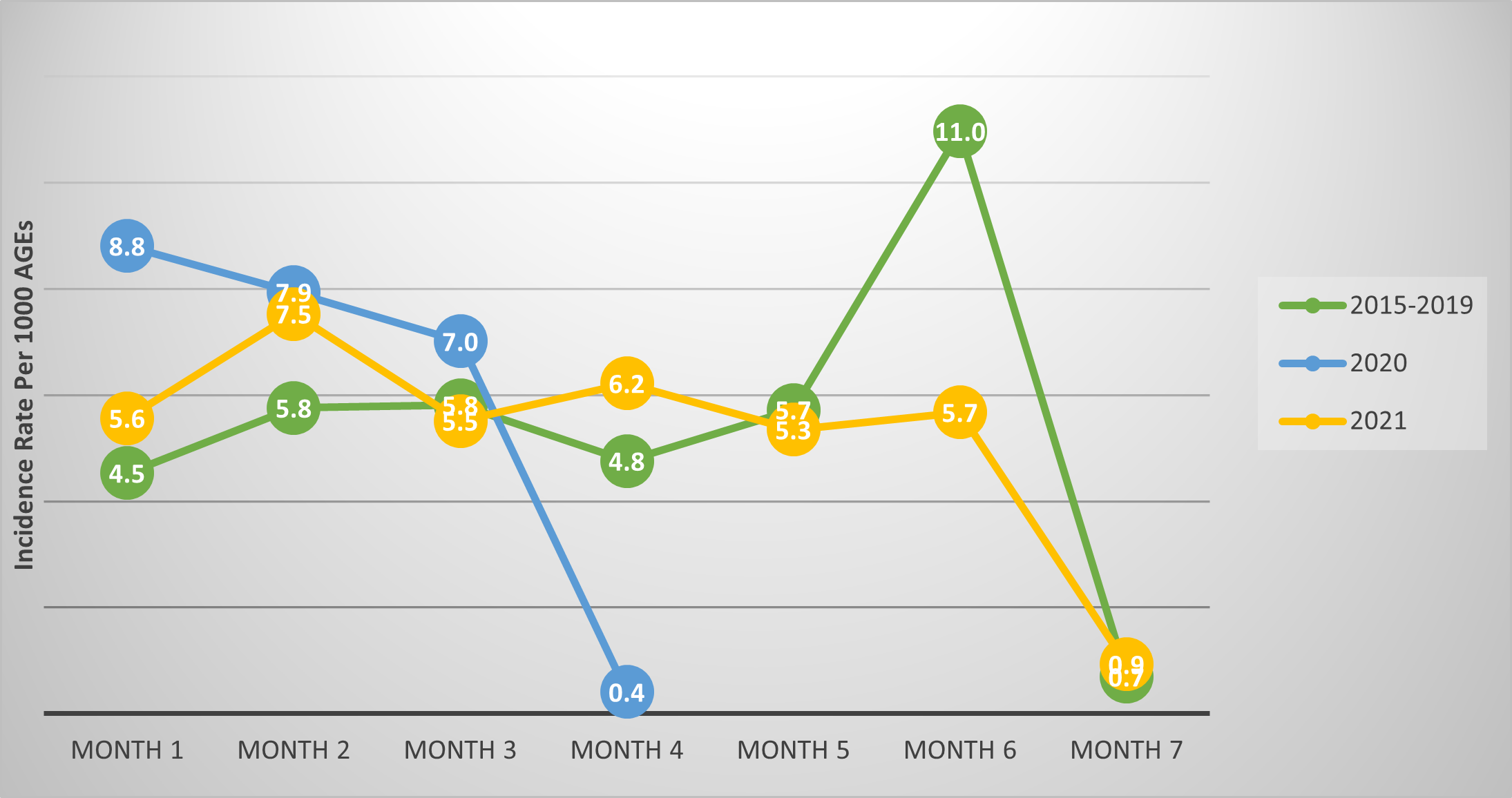
Between 2015 to 2021 seasons, 4,274 injuries were documented across 796,502 AGEs. The 2015-2019 seasons incidence rate was 5.4 per 1000 AGEs overall, followed by an increase to 5.9 per 1000 AGEs during the 2020 COVID-19 shortened season, before decreasing to 5.0 per 1000 AGEs during the 2021 season (Table 1). By month, the IR peaked and was higher during the first two months in 2020 (month 1: 8.2 per 1000 AGEs, month 2: 7.9 per 1000 AGEs), compared to 2015-2019 (month 1: 4.5 per 2000 AGEs, month 2: 5.8 per 1000 AGEs) and 2021 (month 1: 5.6 per 1000 AGEs, month 2: 7.5 per 1000 AGEs) (Figure 1). Compared to previous years, the IR remained elevated in month 1 (5.6 per 1000 AGEs), and month 2 (7.5 per 1000 AGEs) compared to first two months in 2015-2019 (Figure 1).

Injury Incidence Among Pitchers
For pitchers the highest IR was observed in 2020 at 2.2 per 1000 AGEs compared to the 2015-2019 (1.9 per 1000 AGEs), and 2021 (1.0 per 1000 AGEs) seasons. By body region, the highest elbow injury IR of 0.7 per 1000 AGEs compared to 2015-2019 (elbow: 0.2 per 1000 AGEs), and 2021 (elbow: 0.1 per 1000 AGEs) seasons (Table 2). Pitchers demonstrated an increased risk of 3.5 (95% CI: 2.1, 6.0) of sustaining an elbow injury during the COVID-19 shortened season compared to the previous five seasons (Supplemental File 3).
Injury Incidence Among Position Players
For position players the highest overall IR was observed in 2020 at 9.5 injuries per 1000 AGEs compared to 2015-2019 (9.1 per 1000 AGEs), and 2021 (9.0 per 1000 AGEs) seasons. During the 2020 season, the groin/hip/thigh (2.0 per 1000 AGEs) was the most commonly injured body regions during the COVID-19 shortened season; these IRs were elevated compared to the 2015-2019 (groin/hip/thigh: 1.7 per 1000 AGEs) and 2021 (groin/hip/thigh: 1.7 per 1000 AGEs) seasons (Table 3). Although elbow injuries were less commonly reported in position players, elbow injuries were observed the highest in 2020; position players, with a RR of 1.8 (95% CIs: 1.0-3.6) times more likely to acquire an elbow injury during the 2020 shortened season compared to 2015-2019; this risk remained elevated in 2021 compared to 2015-2019 season (1.6, 95% CIs: 1.0, 2.6) (Supplemental File 3).
Poisson Regression
Across all injuries and positions, Poisson regression results revealed no difference in injury rates between 2015-2019 and 2020 seasons (1.1 95% CIs: 0.9, 1.2, p = 0.310) but a reduction occurred in the 2021 season compared to the 2015-2019 seasons (0.9, 95% CIs: 0.8, 1.0 p = 0.046). The 2020 season saw an increase in elbow injuries during the 2020 season compared to 2015-2019 seasons (2.7, 95% CIs: 1.8, 4.0, p <0.001); when stratified by position, this increase only remained significant for pitchers in 2020 (pitchers: 3.5 95% CIs: 2.1, 6.0, p < 0.001; position players: 1.8 95% CI: 1.0, 3.6, p = 0.073). No other differences were observed in the shoulder or groin/hip/thigh. Refer to Supplemental File 4 for further Poisson regression analyses results.
DISCUSSION
Injury rates were similar during the COVID-19 shortened season among pitchers and position players compared to the 2015-2019 and 2021 seasons for combined injuries. Specific to body region, pitchers demonstrated the highest IR for the elbow during the 2020 with the elbow demonstrating an increase in 3.5 times the rate compared to the previous five seasons. Among position players, the groin/hip/thigh was the most commonly injured body region during the COVID-19 shortened season at 2.0 per 1000 AGEs; however, this difference was not significantly different from the pre- COVID-19 seasons.
Overall Injury Incidence
Injury rates increased minimally during the 2020 season, but not to a clinically meaningful level compared to 2015-2019 and 2021 season. Notably, the IR during the first two months of the season demonstrated peak IR that was higher than the first two months of 2015-2019 season IR. During the COVID-19 shortened season, players experienced a delayed and condensed spring training, a period of time in which MLB players are usually able to gradually increase their skill specific workload prior to the regular season.8 Access to training facilities after the postponement of spring training was variable prior to the delayed start of spring training in July 2020.8 Once resumed, spring training was reduced to two to three weeks, less than half the allotted time compared to previous seasons.8 Additionally, a condensed schedule (60 games in two months, versus 162 games in six months) with an expanded post season (16 versus eight teams) occurred, increasing the amount of doubleheaders played in a season with decreased rest days.8 Furthermore, COVID-19 isolation protocols restricted players from playing or training once they tested positive to prevent the spread COVID-19, likely having a de-training effect on individual players.8 Although protocols were in place throughout the league, abrupt cancellations due to COVID-19 outbreaks amongst teams likely impacted training regimens and game schedules.8 Despite these abrupt changes in routine among players, overall injury rates were not significantly different based on crude injury rates or the Poisson model results. Only one study was identified that investigated IR changes among MLB players comparing 2019 and 2020 IR across multiple body regions.3 Platt BN et al confirmed the current findings that injury rates increased during the COVID-19 shortened 2020 season compared to previous seasons.3 However, Platt BN et al demonstrated a higher IR in 2020 compared to the current results (8.66 per 1000 AEs versus 5.84 per 1000 AGEs), and regression modeling strategies were not performed impacting the ability to control for variation in athlete exposure for seasonal comparisons. The differences in IR noted may also be due to varying season time frame comparisons (2019, versus 2015-2019 and 2021) or differences in exposure calculation (AGE versus AE); furthermore, our study accounted for post-season AGEs which may have attributed to our lower IR reported. However, external validation was performed and reported in this study which demonstrated excellent reliability for injury reporting improving clinical interpretability. Further studies investigating incidence rates stratified by season time frame and body region are recommended to determine if specific body regions are impacted at varying times of the season by changes to preseason or season formats.
Injury Incidence Among Pitchers
The elbow demonstrated the highest injury incidence among pitchers during the 2020 season, representing an increase of 3.5 times the rate of the previous five seasons. Elbow injuries often lead to significant disability among MLB pitchers, leading to highest number of days on the MLB Injury List.27 In a 2017 study examining 15 seasons from 1998-2015, 30% of elbow injuries among MLB pitchers were season ending, 28.4% involved ligamentous structures, and pitchers that incurred an elbow injury lead to surgery more often than position players (pitchers: 40% versus position players: 17.6%).27 The baseball pitching motion places substantial forces at the elbow, at upwards of 115 N/m.28–30 The structures at the elbow working to resist these high forces at the elbow are static structures including the ulnar collateral ligament30 working in conjunction with dynamic structures such as the flexor carpi ulnaris, two structures often implicated at the elbow when pathology occcurs.31 Furthermore, kinematic variables including shoulder abduction angle,22 timing and amount of trunk rotation and lateral tilt,28,32 play a role in forces measured at the elbow. However, as a pitcher presents with fatigue via acute work load changes, kinematic variable changes have been documented. Electromyographic activation of the flexor carpi ulnaris decreases,31 maximum external rotation decreases, and knee extension at ball release decreases. These kinematic and EMG activation changes likely contribute to the subsequent decrease ball velocity in a single extended pitch outing.33 The influence of fatigue on kinematic variables, change to spring training schedule, and the increased density of games played during the 2020 season may have played a role in the increased incidence rate of elbow injuries observed,8 despite the in season changes to expand roster size during the 2020 season.3 Sports clinicians should carefully monitor pitchers for changes in pitch volume that acutely increase or are sustained for longer bouts of time and implement appropriate recovery and injury mitigation strategies to minimize elbow injuries.
Injury Incidence Among Position Players
During the COVID-19 shortened season, the groin/hip/thigh demonstrated the greatest IR by body region among position players at 2.0 per 1000 AGEs, this body region is often the most commonly reported injury site among position players in previous seasons.34 Previous literature demonstrates a similar AE for combined lower extremity injuries at 2.0 per 1000 AEs.3 Amongst major and minor league players during the 2011-2016 season, hamstring strains were the most commonly reported pathology.34 Other injuries reported among baseball players to this region include extra-articular injuries such as adductor and quadriceps muscle strains or avulsions, and contusions; intra-articular injuries can also occur including labral pathologies and femoral acetabular impingement.35 Groin/hip/thigh injuries can occur during acute bouts of quick acceleration or deceleration moments during base running or fielding, or via cumulative sport demands of repetitive fielding, throwing, batting, representing longer chronicity of symptoms.35 Although there is an elevation in IR in the groin/hip/thigh region observed during the COVID-19 shortened season compared to previous seasons, the results of the Poisson regression did not demonstrate this to be statistically significant, likely due to the wide and overlapping 95% CIs reported. However, it is notable to consider the potential detraining effects as impacted by density and disruption of the 2020 game schedule and isolation protocols that may have influenced recovery and training strategies contributing to the groin/hip/thigh injuries reported.8 Detraining of type II muscle fibers occur in as little as two weeks of inactivity, and 8% of one rep max strength decreases have been shown after one month of detraining periods.36 These disruptions may have also impacted acute and chronic workload increases compared to previous seasons.37–40 Increased cumulative training workloads have been previously associated with susceptibility to overtraining syndrome9,41 and acute injury25,42 which may have influenced the IR seen in the groin/hip/thigh.
Clinical Implications
This study and previous literature provide a framework for injury surveillance, the first step in the sequence of injury prevention recommended by van Mechelen and colleagues.7 Furthermore, this paper informs baseball stakeholders on the resulting injury burden when abrupt changes in season and training occur (i.e. COVID-19 pandemic, seasonal lockouts during negotiations) followed by an accelerated return to sport. Although the differences in overall injury incidence may not be clinically significant, players are at the highest risk for the most vulnerable injuries, particularly the elbow among pitchers, and groin/hip/thigh injuries among position players. By investigating the 2021 season, which demonstrated decreases in injury incidence, this allows for strong pre and post season comparisons when abrupt seasonal changes occur. Longer periods of ramp up with titrated loading strategies, coinciding with targeted elbow and thigh injury prevention programs may allow for improved recovery and injury mitigation strategies needed to combat the increased risk for acute elbow and groin/hip/thigh injuries during return to baseball following abrupt cessation of sport such as the COVID-19 pandemic or other work stoppage scenarios.2,40
Limitations
This study is not without limitations. Only MLB players were assessed, decreasing generalizability of the results to other professional baseball leagues or amateur baseball players. Further, the public data set utilized does not allow for missing data to be quantified, which may impact the precision of these results. However, external data validation was performed with other publicly available data to increase the interpretability of these results. Additionally, injuries were classified by IOC standard labels to the nearest anatomical body part14; injuries reported based on pathology (i.e. ulnar collateral ligament tear, hamstring strain, oblique strain) were inconsistently reported, decreasing the potential clinical interpretability of these findings. Finally, an estimated player-game exposures were used to calculate IR based on typical games played each season. Athletes by position may have different exposure to sport, which was not possible to calculate with these data, impacting the clinical interpretability of these findings.
CONCLUSION
Combined injury rates were similar during the Covid-19 shortened 2020 season among all positions compared to the 2015-2019 and 2021 seasons. By body region, the elbow was the most commonly injured body region in 2020 among pitchers, with the elbow demonstrating an increase in 3.5 times the rate compared to the previous five seasons. Among position players, the groin/hip/thigh demonstrated the highest IR in 2020. Baseball stakeholders may consider longer periods of ramp up and loading strategies; these loading strategies may allow for improved recovery and injury mitigation strategies following training disruptions. Injury mitigation strategies should give attention to the most vulnerable injuries, particularly the elbow and groin/hip/thigh region among all MLB players.
Conflict of Interest
The authors report no conflict of interest.