INTRODUCTION
In a 2018 report to Congress, the Centers for Disease Control and Prevention (CDC) classified mild traumatic brain injuries (mTBI) among children aged 18 years and younger as a major public health burden.1 Sports are a leading source of concussion, a form of mTBI, with approximately 1.6 to 3.8 million sport-related concussions (SRC) occurring each year.2 Athletes in the adolescent age group of 10 to 19 years comprise the largest athletic cohort at nearly 44 million participants annually.3 Additionally, nearly 70% of all SRC cases in the United States were reported among adolescent athletes.4 As a response to the growing rate of emergency department visits secondary to concussion among adolescents,5 concussion management groups including the American Medical Society for Sports Medicine (AMSSM)2 and Concussion in Sport Group (CISG)6 have promulgated recommendations for improvements in the recognition, diagnosis, rehabilitation, treatment, and overall mitigation of SRC.
The most common symptoms following SRC in adolescent athletes include deficits in somatic, vestibular, oculomotor, and cognitive systems as well as abnormalities in emotional regulation and sleep.6,7 Postural instability has been identified as a hallmark of SRC8,9 and authors have established that prolonged dizziness, reported in approximately 65-75% of athletes with concussion, is most predictive of protracted recovery.10 For this reason, multimodal sideline assessment batteries assess a variety of symptom characteristics as well as neuromotor capabilities.2,6–8 Specifically, researchers have shown that SRCs commonly disrupt important neurological processes that allow for communication between the vestibular system, cerebellum, and motor cortex, which play critical concerted roles in controlling posture and balance during gait.9,11 Although previous authors have reported that neurocognitive impairments persist beyond subjective symptom resolution, dynamic motor tasks such as gait following concussion may not be adequately assessed clinically.11
Authors exploring deficits in gait among athletes with SRC have shown that no significant differences exist when compared to healthy controls while ambulating alone.12,13 In contrast, researchers have identified deficits in neuromotor capabilities athletes of varying ages with and without concussion during walking within a dual-task paradigm, which combines cognitive and motor demands.14–19 Additionally, a significant dual-task cost (DTC), or the relative change between single-task and dual-task performance,14 has been reported for specific spatiotemporal parameters of gait, including gait speed,13,16–20 cadence,12–14,16,17 stride length,12–14,16,17 step length,18,20 double limb support time (DLS),16,18–20 and single limb support time (SLS)18–20 in athletes with and without concussion using computerized technology. Howell et al21 previously reported good to excellent consistency for DTCs when assessing adolescents during single- and dual-task walking, concluding that healthy controls are effective comparators when assessing subjects with injury. Cognitive tasks incorporated into dual-task gait paradigms have challenged different constructs of cognition, memory, and coordination. The Mini-Mental Examination (MMSE), Auditory Stroop Test, and Brooks Visuospatial Memory Task, which incorporate constructs of memory, auditory perception, and recall, have been used to demonstrate that significant differences in gait parameters exist between adolescents with and without SRC in dual-task, but not always single-task, gait paradigms.12,13,21,22 Authors examining dual-task gait paradigms have also established normative reference values for adolescent athletes using varying methodologies and cognitive tasks, which have provided great insight into remaining deficits even after symptom resolution; however, many studies lack a closed environment mirroring aspects of athletic play wherein athletes’ attention is focused on a manipulatable hand-held object during gait.
Ambulation while manipulating a hand-held object, such as a phone or sports ball, is commonplace in daily activities (e.g., maneuvering through class or school spaces while texting) and athletic play (e.g., catching or focusing on a ball in football or soccer, among other sports, while running in a specific direction). In 2018, Howell et al23 revealed that collegiate athletes with a history of concussion demonstrated significantly decreased walking speed during dual-task gait with neurocognitive tests presented on a hand-held tablet compared to healthy controls. Furthermore, in 2019, Lowe et al20 established baseline data for healthy adolescent athletes during single-task gait without a cognitive component and dual-task gait using a hand-held tablet to perform a visuospatial memory task while walking along the GAITRite® Walkway System. In that study, authors found that both male and female healthy athletes experienced a significant DTC (p<0.0001) for gait velocity, step length, DLS, and SLS.20 However, data for concussed adolescents combining a motor and cognitive (visuospatial memory) task with altered visual attention has not been published. An altered, or larger than expected DTC during a combined motor and cognitive task post-concussion could pose a risk to adolescents returning to daily activity and especially athletic play.24 Studies have highlighted the complexity of concussion as a formal diagnosis given variability in symptomology and recovery timeframes.1,2 Despite the existence of widely adopted return to play (RTP) protocols based on symptomology, no consensus has been reached regarding the consistent assessment of postural stability during gait. Therefore, examining DTC may be a viable and insightful addition to comprehensive assessments of concussion.
Compensatory strategies may not be entirely consistent between individual athletes with SRC.25 Given that individuals with concussion often present with such a variety of compensatory mechanisms during movement, the authors of the current study believe it is essential to examine athletes individually while assessing multiple parameters. For the purpose of the current study, authors focused on normalized velocity (m/s), step length (m), and SLS and DLS as a percentage of a gait cycle (%GC), which may present quite differently from one injured athlete to the next. Consistent with common methodologies in physical therapy for assessing children with deficit,26 the chosen cutoff for considering a parameter to be of concern and warrant further attention is one standard deviation (SD). Specifically, the outcome measure of interest was the DTC experienced by adolescent athletes with SRC on each spatiotemporal parameter of gait.
Therefore, the purpose of this study was to evaluate the DTC in adolescents with an acute or chronic SRC compared to reference values from healthy athlete peers22 for spatiotemporal parameters of gait during walking with and without a concurrent visuospatial memory task presented on a hand-held tablet. Researchers hypothesized that adolescents during the acute phase of concussion and seeking a medical evaluation or follow-up would be likely to experience a DTC greater than one SD compared to healthy athlete peers in at least one spatiotemporal parameter of gait when walking within the dual-task paradigm. This study also aimed to explore any residual deficits compared to their healthy athlete peers that might present during the chronic phase of concussion that could aid in RTP decisions.
METHODS
Participants
A convenience sample of 29 athletes, between the ages of 14-18 years old, with documented SRC was recruited from a regional sports medicine concussion clinic. The Institutional Review Board at the University of Arkansas for Medical Sciences approved the study. All participants and guardians provided written informed consent to participate in the study. Participants were included in the study if they were being treated at a regional sports medicine clinic for a sport related concussion, had participated in sport programs through their school, were between the ages of 14-18 years old, and had a completed informed consent from the parent/guardian. Participants were excluded if they had a recent lower extremity injury or were deemed medically unfit to participate in assessments by the clinic sports medicine physician. Using the protocol outlined below, participants were assessed at each clinic visit until discharge (minimum of one and maximum of three assessments). Therefore, an individual participant in the current study could contribute up to three assessments if that participant continued to be seen in the clinic for a protracted recovery. Data from these assessments were divided into acute and chronic categories based on significant differences in neuropsychological function after a period of 28 days.27
Protocol
Gait parameters were assessed by instructing the participants (n=29) to walk at a self-selected speed on the 5.186 meters long GAITRite® (CIR Systems, Inc.; Franklin, NJ) portable gait analysis walkway for three undivided attention trials in addition to three divided attention trials. During each divided attention trial, a visuospatial memory task was given to the subjects to complete on a tablet (Microsoft Surface Pro, 2016) while walking. Participants used a tablet rather than their own cell phones to achieve novelty and require attention to the device. The task (Pattern Memory by ProProfs.com, available at www.memory-improvement-tips.com), similar to the visuospatial memory tasks commonly included in the neurocognitive testing used in concussion management, consisted of a one-second period of time to view a pattern of shapes arranged spatially on the tablet screen. After this time period, the shapes disappeared. The participants then had to place the shapes in the original position relying upon visuospatial working memory. Participants who typically wear corrective eyewear (e.g., glasses or contact lens) wore them during the assessment. All participants performed this task in the same manner with three practice attempts to learn the task in static stance and data collection during gait beginning at level four of the task. Additionally, the participants initiated the task 2.5 meters prior to stepping onto the pathway to allow the task to continue throughout the entirety of the sensor pathway and to account for acceleration. Investigators monitored each trial to ensure that the participant was actively completing the task throughout the data recording time period. If the participant failed at the task, causing the game to discontinue during a trial, that trial was repeated to ensure that the participant was actively completing the task throughout.
The GAITRite® portable gait analysis walkway and the corresponding GAITRite® software were used to record temporal and spatial parameters. Prior to each participant’s trials, investigators entered data for leg length, which was measured as the distance from greater trochanter to floor for each leg. For the purposes of this study, parameters that were captured by the GAITRite® include: gait velocity (cm/s); step length (cm); DLS, defined as the percent of the gait cycle (%GC) when both feet are on the ground; and SLS, defined as the %GC weight bearing through a single limb. The walkway is 5.186 meters long and embedded with sensors recording footfall pressures at 80 Hz, which allows calculation of temporal and spatial markers of gait. The software averages the three gait trials under each walking condition providing means for each parameter. The GAITRite® system has been shown to be a reliable and valid measure of gait for healthy individuals.28
Statistical Methods
Normalized velocity is calculated by the GAITRite® system by dividing the gait velocity captured by the GAITRite® (cm/s) by the participant’s leg length (cm) and then converting the value to meters per second (m/s) for reporting. The data were then compared to the reference values established using the same methods in the healthy athlete participants for all spatiotemporal parameters of gait by Lowe et al.20 Comparisons were stratified based on the frequency of female and male acute and chronic cases that experienced a DTC for each of the parameters of interest that were either within or above one SD of values produced by healthy athletes. Additionally, as concussion management protocols are typically personalized to athletes’ specific capabilities, symptoms, and concussion severity, individual DTC values for each spatiotemporal parameter of gait were also recorded for male and female athletes with acute and chronic concussion during a preliminary and follow-up testing timeline.
RESULTS
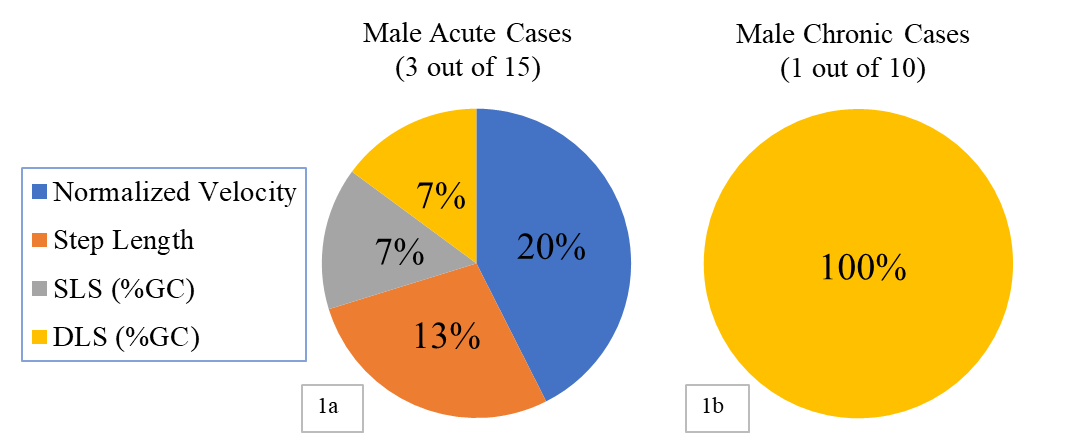
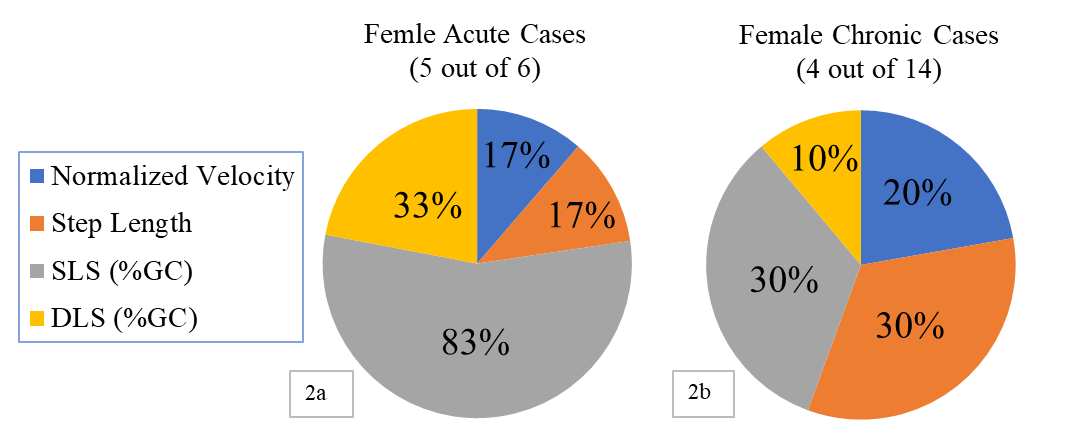
Twenty-nine adolescent athletes with concussion (Table 1) contributed to data collection in several assessment periods during their time in a sport medicine concussion clinic. The 17 male participants with SRC contributed to 25 total assessments, 15 of which were acute and 10 of which were chronic. For the 12 females with concussion, 20 total assessments were recorded, 6 of which were acute and 14 of which were chronic. Table 2 provides means and standard deviations for healthy subjects with and without a concurrent visual cognitive task.20 Table 3 demonstrates the percentage of male and female acute and chronic cases that experienced a DTC greater than one SD compared to healthy subjects for at least one parameter.
Twenty percent of male and 83% of female acute assessments demonstrated such a DTC. The percentage of acute assessments that demonstrated a greater DTC compared to reference values from healthy counterparts was different between males and females for each of the spatiotemporal parameters of gait (Figure 1a and 2a, respectively). In general, most male participants in the acute phase experienced the higher DTC for normalized velocity while most females did so for SLS.
_and_chronic_(1b__one_out_of_10)_cases_that_.png)
_and_chronic_(2b__four_out_of_14)_cases_th.png)
Additionally, 10% of male and 29% of female chronic assessments demonstrated a DTC greater than one SD compared to healthy athletes. For the 10% of male participants assessed in the chronic phase, the increased DTC was experienced in DLS only (Figure 1b). For the female participants assessed in the chronic phase, the higher DTC was distributed across the four parameters (Figure 2b).
DISCUSSION
The present study adds important insight into the need for comprehensive clinical assessments of gait in adolescent athletes with SRC. Lingering deficits in dynamic balance during stance have been previously identified by the current authors utilizing clinical assessments of balance.29 Additionally, for the past decade, the literature has highlighted the importance of assessing dual-task gait among adolescent, collegiate, and adult athletes. Moreover, healthy reference values and DTCs have been frequently used to assess adolescent athletes with concussion when exploring the impact of dual-task paradigms on spatiotemporal parameters of gait. The current study contributes novel findings suggesting that varying compensatory mechanisms exist in male and female adolescent athletes with acute or chronic SRC when combining a cognitive and gait task, further promoting the use of the DTC as a viable adjunct assessment following SRC.
Results from the present study reveal that a considerable number of male and female cases with acute concussion, approximately three out of 15 male assessments and five out of six female assessments, experienced a DTC greater than one SD compared to peers without injury. This finding is similar to those of previous studies that have revealed significant differences between healthy adolescent athletes and those with concussion (typically tested within 10 days after injury) in several spatiotemporal parameters of gait.13,14,16,18 The current study also found that the increased DTC was not experienced for the same spatiotemporal parameters of gait or to the same degree by males and females with acute SRC, suggesting that different compensatory patterns to perform dual-task gait may be evident based on sex in similar samples. Recently, Kieffer et al30 found that even in collegiate athletes, who are presumed to function with more developed neuromuscular abilities, DTCs for several parameters of gait varied irrespective of sex but were overall higher for females. When assessing adolescent athletes within 14 days of concussion, Howell et al16 found that females typically experienced a significantly greater DTC for cadence (not measured in the current study), whereas a separate study reported inconsistent variability in several cognitive, neuromotor, and oculomotor functions according to sex.30 With respect to varying gait strategies, Table 4 provides valuable data for individual assessments by each participant during initial testing who experienced a DTC greater than one SD compared to healthy references in at least one parameter of gait. Male participant A and female participant B, both with acute SRC, experienced the DTC on at least three parameters, representing athletes with the most negative side effects of a concussion who may require personalized balance and gait training in addition to eventually progressing through a RTP protocol. Perhaps more alarming was the presence of participants who were already classified as having chronic SRC at initial testing, namely female participants E and H, and still experiencing a higher DTC than references on at least one parameter of gait. This finding suggests that a classification of chronicity and perhaps symptom resolution may not be sufficient alone in determining an athlete’s readiness to safely return to sport.
The current study also revealed further inconsistencies in the progression of biomechanical strategies for gait in a dual-task paradigm after participants still in the concussion clinic surpassed the threshold for chronicity (>28 days27) during follow-up testing. Table 5 provides information for male and female athletes with chronic SRC who continued to experience a DTC greater than one SD compared to healthy athlete controls. Female participants D and G experienced a DTC within one SD compared to healthy athletes in normalized velocity during the acute phase (Table 4), but then demonstrated a DTC higher than one SD for the same parameter after meeting the threshold for chronic classification. Given that slowed average gait speed has been highly correlated with concussion severity and prolonged recovery after SRC,14,17,24 special attention may be warranted for athletes with elevated DTCs in this parameter. Additionally, although male participant B improved the DTC of his average gait speed and step length, he may have shifted his compensatory strategy to DLS, as evidenced by an increased DTC during the chronic phase (Table 4 and 5). These scenarios of fluid compensatory strategies were not consistent for each participant and varied between males and females; however, athletes like participants B, D, and G, who continued to experience gait deficits 28 days after initial injury, may be at higher risk for reinjury even after progressing through a symptom based RTP protocol.
Modern protocols suggest that, on average, symptom resolution may occur as soon as seven to 10 days following SRC, and most graduated RTP programs progress student athletes back to physical activity mainly guided by subjective symptom resolution.2,6 However, other researchers have identified athletes who reported symptom resolution after 21 to >28 days of initial injury and continued to either walk with significantly slower average gait speeds, smaller cadences, and shorter stride lengths or experience significant DTCs compared to healthy controls. Furthermore, Howell and colleagues24 found that adolescent athletes who experienced reinjury after RTP had consistently demonstrated a significant gait speed DTC across time, similar to participants D and G from our study. Therefore, it is evident that more work needs to be done to adequately assess postural stability in gait for adolescent athletes after SRC in addition to symptoms based RTP protocols. Currently, there is no consensus on a viable tool for assessing spatiotemporal parameters of gait following concussion. Based on the findings of the current study, the GAITRite® Walkway System combined with DTC assessment may provide data valuable in identifying deficits in gait that may otherwise go undetected by multimodal assessments such as the Sport Concussion Assessment Tool (SCAT-third or fifth edition), which assesses subjective aspects of ambulation and limited constructs of postural stability during a tandem gait test.2,6
LIMITATIONS
This study used a sample of convenience in a relatively small group of adolescents with a narrow age range. Ideally, all athletes would have been assessed first during the acute phase of SRC and again in a progressive manner throughout the chronic stage. Additionally, not all athletes were able to contribute to assessments beyond initial testing, either due to worsening symptoms or meeting criteria to initiate a RTP protocol. More robust studies with a longer duration and a sample population from more than one medical facility would contribute to improved generalizability of these findings. Furthermore, a more racially and ethnically diverse sample of adolescents with concussion would contribute to generalizability. Data collection was performed using an expensive piece of equipment, not readily available to most clinicians. Further research comparing data obtained using the same visuospatial memory task during gait with incorporation of more traditional and clinically feasible tools (e.g., 10 Meter Walk Test) could provide valuable and practical insight to more clinicians in a variety of settings. Additionally, the complexity of the visuospatial memory task was not customized to the subject’s individual cognitive or motor capacities. Therefore, given the broad potential impact of concussion on neurocognitive capabilities, the attention, detailed understanding, and processing of all testing requirements may have varied for each participant.
CONCLUSIONS
The findings of the current study support the continued need for comprehensive assessments of postural stability in gait for adolescent athletes with SRC. High variation in DTCs that were greater than one SD compared to healthy subjects for several spatiotemporal parameters of gait highlights the potential need for customized rehabilitation plans prior to eventual RTS. No two athletes in the limited sample of the current study demonstrated the same compensatory strategies, mitigation patterns, or potential deficits during single- and dual-task gait with a SRC classified as either acute or chronic in nature. DTC analysis using the GAITRite® Walkway System may be a valuable adjunct to current assessment strategies following concussion among adolescent athletes. However, given potential constraints regarding financial, set-up time, and training requirements for the GAITRite®, future work is warranted to explore viable clinical assessment tools and/or strategies with strong agreement with higher order technologies for evaluating spatiotemporal parameters of gait. Additionally, future studies may build upon the framework established by this preliminary study by incorporating longitudinal designs with assessment of all subjects at varying stages following concussion with inclusion of matched controls from similar schools.
Conflicts of Interest
The authors have no conflicts of interest.
Funding
Supported by NIGMS IDeA Program award P30 GM110702 through the Center for Translational Neuroscience at the University of Arkansas for Medical Sciences.