Introduction
Acute adductor injuries are a common occurrence in sport. The overall incidence of adductor strains across 25 college sports was 1.29 injuries per 1000 exposures, with men’s soccer (3.15) and men’s hockey (2.47) having the highest incidences.1 As with most muscle strains there is a high rate of recurrence for adductor strains; 18% in professional soccer2 and 24% in professional hockey.3 Effective treatment, with successful return to play, and avoidance of reinjury, can be achieved with a proper understanding of the anatomy, a thorough clinical exam yielding an accurate diagnosis, and an evidence-based treatment approach, including return to play progression.
Anatomy
The adductor muscle group is comprised of six muscles that run along the medial thigh: adductor longus, adductor brevis, adductor magnus, pectineus, gracilis, and obturator externus. In general, these muscles attach proximally to the anteroinferior part of the pelvis. They are innervated by the obturator nerve, except the pectineus (femoral nerve) and part of the adductor magnus (sciatic nerve). As their name suggests, the primary action of the adductor group is adduction of the thigh, however their actions include several secondary functions. They play an important role in trunk stabilization, contribute to flexion and extension of the thigh when running, and are used in kicking a soccer ball with the inside of the foot. The adductor muscle group may also act as lateral or medial hip rotators depending on the mechanical axis of the femur. The adductor muscles are typically referred to as a group, but the adductor longus is the muscle most frequently involved in adductor-related groin pain.
Diagnosis
The diagnosis and treatment of adductor strains can be challenging. The term groin strain has been used to describe pain in or around the pubis, but it is important to differentiate between adductor strains and other clinical entities in the pelvic region. Weir et al developed a taxonomy to classify groin pain as adductor-related, iliopsoas-related, inguinal-related, pubic-related, or hip-related.4 However, these conditions can be overlapping, further complicating the diagnosis and treatment approach. Inter-examiner agreement using this classification system was excellent for athletes with a single entity but more difficult for athletes with multiple clinical entities.5 While most muscle strains present with an acute onset of symptoms associated with a distinct injury mechanism, adductor strains often can have an insidious onset, and long-standing adductor-related pain is not uncommon. Furthermore, even when the adductors are the primary source of symptoms, the injury could be a muscle or tendon injury. A tear at the origin of the adductor longus tendon or adductor longus tendinopathy are common. Treating a tendon injury as a muscle strain can be counterproductive.
In the absence of imaging the clinical diagnosis of an adductor strain can be made based on a combination of factors relating to the timing of the onset of symptoms, the location of the symptoms and the actions that most readily provoke the symptoms (Table 1).
The most straightforward presentation of an adductor strain is an athlete with an acute onset of pain in the adductor region necessitating removal from the game. On exam there is tenderness on palpation of the adductor muscles that is exacerbated with resisted adduction and passive stretch of the adductors.
Timing of Symptoms: If an athlete presents with adductor-related pain the day after a game but had no symptoms during the game, this is more likely muscle damage, which should resolve uneventfully. If an athlete presents with a history of chronic adductor-related pain or intermittent adductor symptoms with activity, the index of suspicion moves towards tendon injury.
Location of Symptoms: The location of symptoms on physical exam can be variable. Tenderness along the adductor muscles to the proximal insertion is common. The more proximal the point of peak tenderness the more likely there is tendon involvement. Peak tenderness at the adductor tendon origins with no discernible tenderness into the muscle increases the likelihood of a tendon injury. Pain at or above the inguinal crease points to athletic pubalgia, including related inguinal hernias.6 In cases where there is adductor muscle tenderness, with tenderness at the tendon origin and tenderness in the inguinal region it is probably best to focus on the more proximal symptoms.
Provocation of Symptoms: Obviously with any significant adductor muscle strain there will be pain with resisted adduction. Resisting a distally applied hip abduction force with the knees extended may be more specific for an adductor strain than an adductor squeeze test with the knees flexed. However, the adductor squeeze test (with knees extended or flexed) is used primarily to identify athletes with groin or hip problems as opposed to specifically diagnose an adductor strain.7 In fact, performing the adductor squeeze test with knees flexed, while performing a sit up, called the Resisted Adduction Sit Up Test (RASUT), identifies athletic pubalgia.6 Adductor muscle pain with passive hip abduction may be indicative of a significant muscle strain, especially if symptoms occur with only moderate muscle stretch. As the magnitude of the stretch increases it can become more difficult to differentiate normal stretch discomfort from pain due to a muscle injury. Additionally, with greater motion the discomfort may be at the tendon origin and resisted adduction will be necessary to test for muscle involvement. Thus, resisted adduction tests may be more useful in diagnosing an adductor strain than passive stretches.
Treatment
While there have been no randomized clinical trials testing different treatment programs for adductor strains, programs with similar progressions have been described.8,9 Nonoperative treatment for adductor strains is standard and can successfully return athletes to play with low risk of reinjury. A criterion-based rehabilitation program with 3 stages has been described9 whereby the athlete must be clinically pain free (stage 1) before progressing to controlled sports training (stage 2) and then to full team training (stage 3). The time to return to play will be dependent on the extent of injury. Athletes with complete tears (grade 3 on MRI) unsurprisingly take longer to return to play.9 However, for partial tears the recovery time was similar between grades 1 and 2.9 The later stages of rehabilitation will vary depending on the sport the athlete is returning to, but the same principles apply throughout the process regardless of the sport.
In the acute phase (24-48 hours) the goal is to limit the proliferation of the initial tissue disruption. Early and repeated application of ice can reduce tissue metabolism and limit tissue damage.10 In the subacute phase (2-7 days post injury) the goal is to protect the site of injury while the scar forms between the fractured muscle fibers. However, immobilization can result in excessive scar tissue.11 Therefore, early mobilization avoiding excessive stress on the injured fibers is recommended.
Reactivation of the adductors with hip adduction exercises can progress along a continuum from low intensity submaximal isometric and concentric contractions at short muscle lengths, to high intensity maximal eccentric contractions at long muscle lengths (Table 2). This progression of hip adduction strengthening exercises should account for the combinations of contraction intensity, muscle length and contraction mode.
Maximal voluntary force production is lowest for concentric contractions and highest for eccentric contractions and therefore, maximal isolated eccentric contractions are categorized at a higher level than maximal isotonic contractions. However, isotonic contractions that are performed in the full available range of motion (ROM) can involve reinjury risk in the transition from the eccentric to concentric phase, as this occurs at a long muscle length, where there is significant passive tension on the muscles, and the contractile ability is compromised by the length-tension relationship. The Copenhagen adductor exercise was developed as an isolated eccentric exercise, but can be performed as an isometric exercise, and as an isotonic exercise. Regardless of contraction mode it is a high intensity exercise, and it is difficult to modify intensity. Performing the Copenhagen adductor exercise isotonically involves a lot of stress in the eccentric to concentric transition because it occurs at a longer muscle length than during the concentric to eccentric transition. Therefore, the exercise should be progressed carefully, starting at short muscle lengths with isometric contractions. The Copenhagen adductor exercise is primarily beneficial as an exercise for healthy adults to prevent adductor strains and other groin injuries. It’s effectiveness in adductor strain rehabilitation is not as well established but it has been used in successful adductor strain rehabilitation.9,12
Return to Sport Strength Testing
Readiness for return to sport can be established using general agility tests (e.g. Illinois agility test) and sports specific tests that stress the adductor region. However, it is important to consider the isolated function of the hip adductors to ensure that the repair process occurs with a complete restoration of the function of the injured structure. Therefore, an objective validated assessment of hip adduction strength is essential, and it is beneficial to assess the strength in comparison to the antagonist hip abductors. Such testing can be performed on an isokinetic dynamometer, but availability and limited validation bring both practical and scientific limitations. Testing with a hand-held dynamometer for sidelying hip adduction and abduction has been validated12,13 and offers a more practical solution.
The key requirements for hip adduction strength testing are that (1) a comparison can be made between the involved and noninvolved sides, (2) a comparison can be made between the agonist (adductors) and antagonist (abductors) muscle groups, and (3) that the unit of measurement for strength allows comparisons across populations (e.g. comparison to uninjured teammates).
In comparing strength between legs, it is essential that each side is tested independently. Squeeze tests where both limbs contract maximally at the same time cannot be used to assess symmetry in adduction strength between limbs. The laws of physics and neurophysiology invalidate such tests. Newton’s third law states that for every action (force) there is an equal and opposite reaction. If one squeezes a dynamometer between the knees in the bent knee adduction squeeze test, or between the feet in the straight leg squeeze test, Newton’s third law dictates that the force on the right side will equal the force on the left side. This limitation is not overcome by separating the legs and squeezing a frame with a force transducer on each side, as is described using the ForceFrame device (Vald Performance, Queensland, Australia).14 It follows that squeeze tests have not been shown to be effective at identifying strength deficits between limbs but have been effective at identifying athletes with groin and hip pathology versus healthy athletes.7
The neurophysiological limitation of comparing strength between limbs while performing simultaneous maximal efforts with both limbs, is referred to as the bilateral deficit.15 The bilateral deficit phenomenon is characterized by a lower force generated when two limbs perform a maximal effort bilaterally compared with the sum of the forces generated by the two limbs when performing the effort unilaterally. While the bilateral deficit has not been studied specifically for clinical assessment of weakness no studies have validated bilateral testing for identifying unilateral weakness.
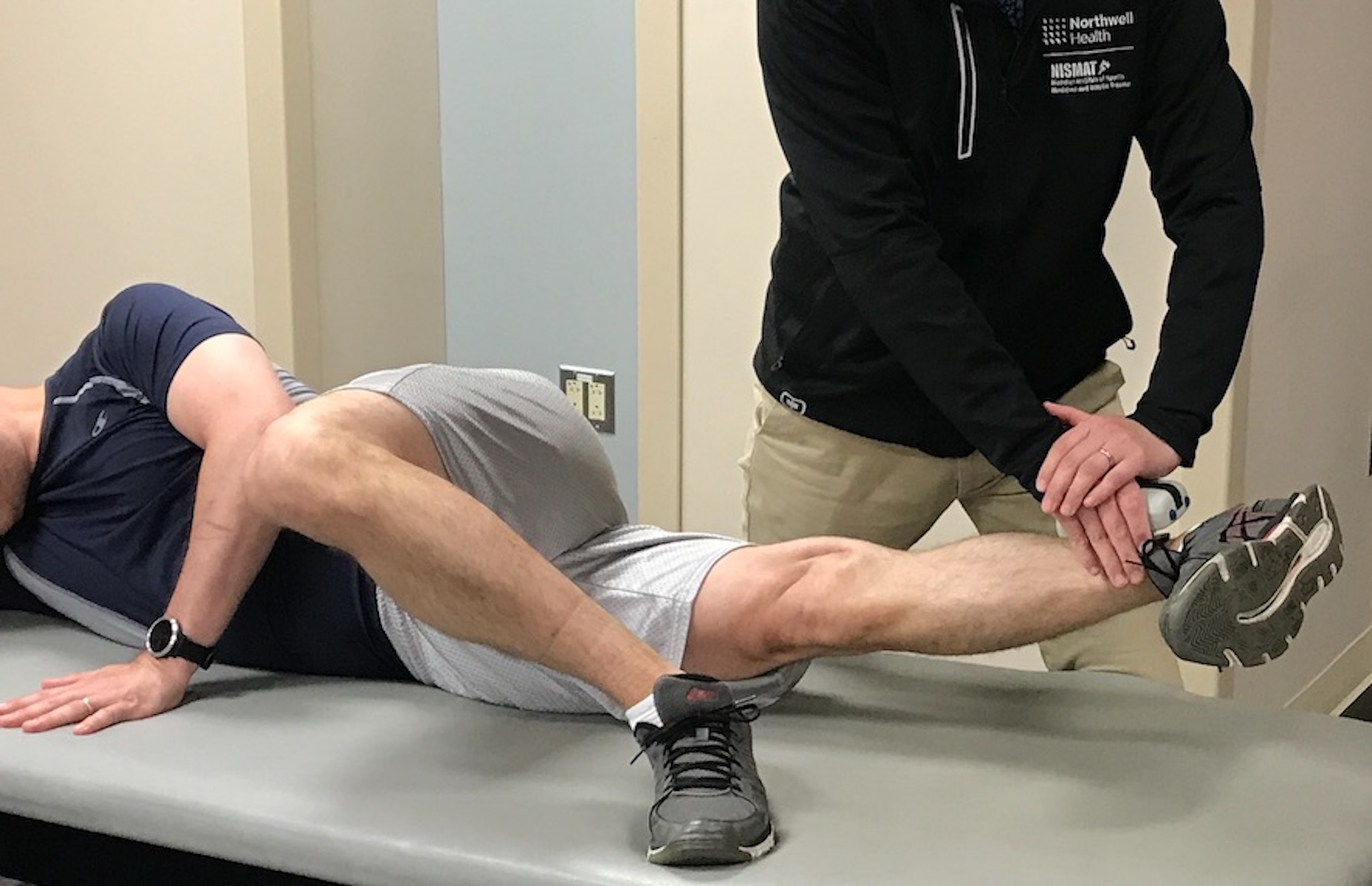
While these two limitations (Newton’s third law and bilateral deficit) highlight the importance of unilateral testing for hip adduction strength assessments, it is important to emphasize the role of stabilization for achieving a valid result. In testing hip adduction strength in side-lying, the subject can oppose their hip adduction force (upwardly directed force) with their torso and shoulder pressing against the table they are side-lying on (downward directed force) (Figure 1). However, if one tests hip adduction strength unilaterally in supine, one must provide an opposing force to stabilize the torso to allow the subject to generate a maximal effort without rotating the upper body away from the direction of the adduction force. Such tests performed without stabilization against the countermovement may be reliable, but they are not valid tests of the maximal adduction strength.

The importance of being able to test the hip abductors in addition to the adductors is that weak adductors relative to abductors can be a risk factor for a future adductor strain.13 Therefore, the rehabilitation process should restore a balance between the agonists and antagonists in addition to balancing the involved and noninvolved sides. Lastly, it may be important to compare hip adduction strength in the rehabilitating athlete to their peers, to ensure that strength matches the requirements for the sport. In this regard the standard unit of measurement for hip adduction strength is Newton-meters per kilogram body mass (Nm/kg). Hip adduction force in Newtons, or Newtons relative to body weight do not provide a valid comparison between individuals varying in stature and weight.
Conclusion
When an athlete can perform sports specific functional testing symptom free at a performance level comparable to uninjured peers and has normal hip adduction strength (within 10% of the noninvolved side and within 10% of the ipsilateral hip abductors) there should be low risk of reinjury on return to play. Importantly, by providing the athlete with objective criteria on their readiness to play they will be less likely to have fear avoidance upon return.