

INTRODUCTION
Anterior cruciate ligament (ACL) injury is one of the most controversial injuries in the world of sports. For example, ACL injury represents only 14% of injuries in soccer,1 but causes physiological and psychological modifications that can compromise the progress and career of soccer players. Forsythe et al. showed that only 71% of injured players return to their previous level within one year after the injury and only 81% return within three years.2 If the return to the previous level is difficult after an ACL reconstruction (ACLR), it also appears that return to play (RTP), and at high level, can be hampered by a significant number of reinjury, as shown by Della Villa et al.3 The safest possible RTP is a major sporting and economic challenge after ACLR.4
Hence, implementation of functional assessments is important in the return to sport and RTP decisions for soccer players. If the isokinetic assessment, the hop tests and the psychological assessment seem to be gold standards it is important to note that these assessments are neither scientifically validated nor capable of predicting the risk of recurrence.5,6 Others authors have highlighted the lack of specificity and ecological situations in soccer player assessment as close as possible to their activity.7–10
It is important to develop ecological tests based on the specific skills of the soccer player and on solid scientific algorithms. Thus, the proposed test sequence is based on the “5 factors maximum model” developed by Hewett et al. aimed at prediction of ACL injury risk11 but also on ecological situations that result from the “11 to perf” assessment developed by Clairefontaine at the FIFA Medical Center. The 5-factor maximum model is based on anthropometric, strength and coordination, biomechanics, proprioception and balance, and psychological characteristics.11,12 In addition, it is important to develop quantitative and qualitative tests with reliable and recommended evaluation tools (robotic laximetry, force platforms, etc.). The use of a scientific algorithm predictive of ACL injury that complements the existing tests, while approximating ecological situations, is a clinically relevant means of being able to make a safe decision in the RTP after ACLR in soccer player. Thus, it seems important to us to divide the suggested assessment into two stages (or 2 phases): Clinical using results from standardized tests, and field using results from an ecological situation specific to the soccer player’s environment (Table 1).
THE FIRST STEP: Clinical Assessments
Before performing a sequence of tests allowing the return to the field, it is necessary to ensure the motor abilities of the patient such as walking without limping, or the return to running.
Running
Running activity during rehabilitation of a patient after ACLR is unfortunately usually not sufficiently addressed.13 Often, running activity is a generic term that includes running in water, in-place running, running on a treadmill (with or without altered gravity), or educational running exercises, jogging, stadium running, trail running… Hence, rehabilitative management should focus on gradually increasing running demands through a continuum of exercises and activities in preparation for sprinting and changing directions (cutting/pivoting).
After ACLR, the return to running can be initiated very early (two months postoperatively) as previously proposed (see Rambaud et al. 2018) and but only with normal clinical criteria (no pain, full range of motion, operationalized knee flexion and extension strength).14
However, in current clinical practice, it is commonly during the fourth postoperative month that most patients are allowed to resume running (from three months postoperatively).13,15 This time frame is proposed to consider the biological processes of integration of the graft into the bone tunnels and the general healing of the knee joint.
Even if running induces little stress on the ACL (and by extension, the same for the graft), it remains a stressful activity for the femorotibial and patellofemoral joints, which can result in altered loading and pain, which is seen as a limp (running with low knee flexion, or with a dynamic valgus).16 A clinical assessment and a test battery seems to be essential to consider the start of running and a running program is initiated according to the patient’s abilities found during these evaluations (e.g. Delaware Interval Running Protocol).17 To ensure optimal loading program, the patient’s voice and her/his opinion will be essential. The use of soreness rules is important to avoid major errors in running training.18
Thus, a dialogue must be established, and the program adjusted according to the different elements with which the patient presents (pain, difficulties, fears). Running progression protocol will be continued until interval running protocol, running at high speed, or even sprinting to prepare for side cutting and pivoting activities and return to sport continuum.19
At the time of return to play, a running assessment on a treadmill is useful to evaluate if the running pattern is correct and symmetric. Indeed, even if lower limb dominance can play on asymmetry, it remains rather weak, particularly on lower limb stiffness (between 0 and 3%). The use of an optoelectrical barrier such as the OptoGait (Microgait, Tours, France) can provide an easy way to automate this assessment. Smartphone applications, such as Runmatic (Runmatic App, Dr. Carlos Balsalobre-Fernández), can also provide an overview of the symmetry of the gait parameters (lower limb stiffness) with a recording of eight steps.
After a warm-up on the treadmill, a recording of the flight time and the contact time for each step is made during a 30 seconds running sample, at a speed of 12 km.h-1. According to the work of Morin et al., the stiffness coefficient of the lower limb (its global compression during the acceptance of the body weight during the phase of single-limb support) and be estimated.20,21
Therefore, strength asymmetry of less than 10% for RTP is proposed as healthy subjects present a strength asymmetry lower than 5%, and preliminary studies have shown an increase in the risk of injury if the strength asymmetry is higher than 10%.
Graft Laxity Test
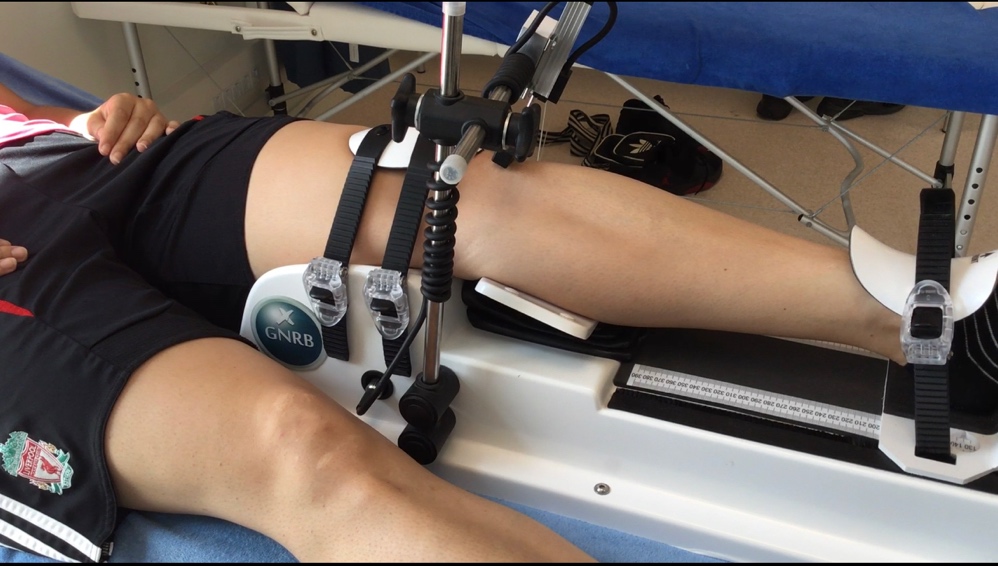
After a normal clinical examination (no pain, full range of motion, no effusion), a test battery can be conducted. Gokeler et al. highlighted the use of a robotic laximeter as a tool to determine one assessment for RTP.22 Too much tibial anterior translation can increase ACL injury risk.22 In addition, graft healing is long time process (approximately 2 years)23 and it is important to be able to assess graft laxity using reliable tools. Lachmann, Pivot Shift, and direct anterior drawer tests are commonly utilized, but robotic laximeter use shows potential for objective data which can inform RTP decisions. A laximeter is a passive test and establishes dynamic elongation curves by comparison of the two knees (Figure 1). The device automatically calculates differential displacement and establishes curve slopes. The cut-off value is the difference of 3 millimeters between the knees24–27 at 134 N for a sensitivity of 70% and a specificity of 99%.27 During RTP assessment, three anterior translations at 250 N can be performed. After examination of the differential at 134 N, the slope differential is assessed. It corresponds to the functional instability risk, which should not exceed 10 μm.N-1. For a result with regard to RTP, we set the differential at 134 Newton to less than or equal to one mm and a slope differential less than five μm.N-1.28–30
.jpeg)
Isokinetic Testing
Although strength tests were reported in only 41% of the studies that describe RTP criteria,31 strength assessment, especially of the quadriceps, is of high importance. Quadriceps strength is correlated with i) functional test performance,32,33 ii) self-reported outcomes34,35 and iii) risk of reinjury.36,37
Strength assessments are performed in different modes (isometric, isokinetic: concentric or eccentric) and various angular speeds. If no standardized protocol is used following ACLR,38 most researchers use concentric peak torque of knee extension and flexion at 60°/s, normalized to body weight (PT60/BW).36,37,39–41 The Limb Symmetry Index (LSI) expresses the performance of the operated side as a percentage compared to the contralateral side. The goal is generally to achieve a PT60/BW-LSI greater than 90%36,37,39,42 but these values are rarely acheived.9 Additionally, the LSI may overestimate the capacities of the operated limb, if the healthy limb is detrained.43 Therefore, clinicians should assess both LSI and reference values.40
The ratio of hamstring and quadriceps peaks (Hamstring /Quadriceps ratio) is not a functional ratio, since it compares peaks appearing at different angles, but it is correlated with the risk of injury.37
The single PT60/BW value analysis could lead to a loss of information, which is why studies should focus on the torque profile specific to the angle of knee flexion,44 in order to improve understanding of the deficits identified, and therefore guide rehabilitation.
Since speed and absorption capacity are necessary for most physical activities, especially when changing direction and jumping,45 Edouard et al. suggest testing using faster speeds and the eccentric isokinetic mode.46 Concentric mode isokinetic assessments cannot assess the differences in rate of force development of the muscles.47
Authors criticize the use of isokinetics for strength assessment because of the gap between this mode of assessment and real life, such as analysis of a single motion in a single plane in contrast to the complexity of sports movements. That movements carried out in an isokinetic manner do not approximate the movements that occur in normal activities (isokinetic speeds described as" fast" do not exceed 300°/s, when certain movements, like sprinting, are performed at a much higher speed). Finally, open kinetic chain testing of muscles usually used in closed chain functional tasks has been discussed.46 Biomechanically, this assessment is the measure of the force couple, in a single plane, which we know to be different in vivo.46
This evaluation nevertheless remains the gold standard, but other methods of evaluating neuromuscular performance are being studied. These methods, like force platforms, are to be more functional.
Hop Tests
Hop tests are designed to assess lower quarter function after ACLR and other surgeries and condtions. While some authors have shown good methodological quality for these tests, their validity has been challenged. According to Kotsifaki et al., knee performance is better assessed during landing and not during propulsion, particularly on Single Hop Test (SHT).48–51 Similar validity issues are observed on Triple Hop Test (THT), especially during the concentric propulsion phase as there can be hip, pelvis and trunk compensations.50 Thus, according to Kotsifaki et al. the LSI obtained during vertical jumps seems to demonstrate knee function deficits more accurately than horizontal jumps.49 The quantitative measure of the horizontal jumps to represent lower limb systemic performance which is essential for RTP.
For a qualitative assessment, use the qualitative analysis of single leg score (QASLS) to evaluate the landing and provide feedback on knee function.52 Indeed, dynamic valgus associated with an increase in the knee abductor moment constitutes a very important risk factor for ACL re-injury as shown Paterno et al.53 During landing test, Hewett et al. highlights a sensitivity of 77% and a specificity of 81% when dynamic valgus appears within the initial 10% of landing.11
Before a more ecological evaluation, the authors recommend assessing the knee on horizontal (SHT, THT), vertical (Single Leg Vertical Jump) and multidirectional (30 cm Side Hop Test, Cross Over) directions. According to the literature, the LSI must be at 90% and the QASLS < 1 in search of an increase in the knee abductor moment.37,52–54
Furthermore, it is important to be able to determine plyometric qualities and coordination in bipedal and unipedal modes (Table 2). Regarding coordination, assessment with the countermovement jump (CMJ) and Abalkov Test can offer information. A difference greater than 6 cm must be found in order to determine good coordination. Regarding plyometric qualities, it is important to perform both the squat jump (SJ) and drop vertical jump (DVJ). The difference should not be below 6 cm. A difference that exceeds 10 cm demonstrates good plyometric qualities. Plyometrics are an essential asset in ACL re-injury prevention.55–57 With the DVJ, we can also calculate the reactive strength index (RSI) which shows the ability of the knee to store and restore energy. According to Flanagan et al. it must be greater than 2.5 in order to show good plyometric quality.58
Proprioception and Balance
Without vestibular disorders, proprioceptive alterations can be assessed via stabilometric analysis which can be performed in bipedal and unipedal modes, with vision or without.
Evaluation of static balance can be assessed by the study of mobility and variations in the center of pressure (CoP) which allows the quality of global proprioception and postural adaptation to be described. Using a stabilometry platform offers the possibility of calculating the Romberg quotient according to Ruhe et al.,59 which quantifies visual dependence in bipedal and unipedal conditions. Visual dependence occurs when a perceptual conflict between different sensory inputs occurs, giving precedence to visual input and creating difficulties in changing frames of reference using vestibular and proprioceptive afferents according Lubetzky-Vilnai et al.60 The Romberg quotient is calculated by the ratio of the surface of the ellipse containing 90% of the points of the center of pressure with eyes closed to that with eyes open; it quantifies the importance of visual input and therefore the importance of vision in postural control. The result is physiologically close to 93% (eyes closed CoP displacement / open eyes CoP displacement; multiplied by 100) with a difference with a standard deviation of 20%.61 To overcome this visual dependence, stroboscopic glasses use associated with visual-motor training has demonstrated effectiveness in reducing reaction time in particular, as well as improving muscle coactivation and muscular anticipation, which then may reduce ACL injury risk.62–66
Dynamic balance should also be assessed, for example, by the Star Excursion Balance Test modified67 or Y-Balance Test. These two tests are also a reliable way to be able to predict lower limb and ACL injury risk. Lee et al. found a strong correlation with knee flexors strength and hip abductors strength.68 Furthermore, Pilsky et al.69 reported that an asymmetry of 4 cm in the anterior distance indicates a high risk of injury to the lower limb that there was a 3.5 times higher risk of injury in the event of a symmetry of less than 90%.
Psychological Assessment
If injury and surgery lead to significant physiological changes, there are psychological considerations, in particular apprehension and confidence, which impact RTP. Paterno et al. showed that athletes with a poor Tampa Scale Kinesiophobia 11 score (19 or more) have a risk factor multiplied by 13 for secondary ACL tears within two years after RTP.70 Straub et al. described a positive correlation in male athletes between symmetrical quadriceps strength and psychological aspect upon RTP.71 Similar results were reported by Webster et al. and Kim et al. who showed a correlation between symptoms, function, and psychological status at RTP.72,73
In the authors’ opinion, the Anterior Cruciate Ligament-Return to Sport after Injury (ACL-RSI) is the best way to assess psychological qualities of the player during RTP. Langford et al. suggest that it is possible to identify athletes at risk of no RTP for psychological reasons after ACLR.74 Ardern et al. highlight that psychological variables measured with ACL-RSI are the only predictors of RTP before injury.75 Therefore, it is important to be able to detect the risk profiles of players who are overconfident in their RTP when compared to their physiological qualities. Conversely, specific psychological preparation for RTP can be initiated if the ACL-RSI score is not satisfactory. Kitaguchi et al., during an evaluation at six months after ACLR, shows ACL RSI cut off values of 81.3% (sensitivity = 0.8 and specificity = 0.6) and a score of 55% (sensitivity = 0.69% and specificity = 0.82) as a predictor of RTS at one year.76
Vertical Force – Velocity Profile during a Squat Jump
Samozino et al.77 relied on Newtonian dynamics laws to create a mathematical equation that allows the calculation of the values of force, speed and power using the following values: body mass, jump height and lower limb extension distance when pushing. It then becomes easy to obtain a reliable estimate of the force-velocity-power relationship of the lower limbs as well as the tracing of the individual force-velocity profile using data from a force plate. The athlete must perform a SJ with body weight alone and add 20% of body weight to each vertical jump. The test stops when the player cannot jump more than 10 cm. (Figure 2).

The profile which is created is compared with a theoretical optimal profile. For a maximum power value, there must be a balance between the qualities of force produced during the jump and the speed at which the jump is made, thus allowing optimization of performance. If the slope of the measured force-velocity line is greater than the slope of the optimal profile, it is necessary to focus on force production. Conversely, if the slope measured is lower than that of its optimal profile, then training must be focused on the development of velocity.
THE SECOND STEP: FIELD (FUNCTIONAL TESTING)
Game Simulation
Welling et al.78,79 highlighted the fact that RTP tests are often not administered in a sport-specific environment. For example, it is uncertain whether performance during hop tests can be transposed to a sport-specific situation in which a patient must react to opponents, teammates, and the ball. Indeed, the actions of dual- task, taking information, processing and decision-making, the specific movements in dual-task, work/performance in a fatigued condition, or even the execution speed of specific gestures are parameters that must be observed during the RTP. However, assessments have many limitations related to the validity and reproducibility of potential tests. To address these issues, the authors have empirically chosen to use a match simulation type session for 45 minutes where the soccer player reproduces the game demands according to position and level of practice80,81 or directly with group of players.
The use of such an observation for the position and the level of the player does not allow a high reproducibility of this session, hence this approach is not used as a “test”. During these 45 minutes, the values of acceleration, deceleration, change of direction, jump, tackle, contact, ball handling skills, high speed running (between 14,4 km/h and 19,8 km/h), very high speed running (between 19,8 km/h and 25,2 km/h), and sprint (with acceleration and deceleration)are assessed according to the athlete-specific references. During these 45 minutes, we evaluated only the most intense 5 minutes, period with the greatest density of activities during a session (bount of sprint, acceleration, braking…). A quantitative and qualitative analysis is carried out through GPS tracking and a biomechanical study of movement control (with videography) during dynamic movements (cutting, braking, sprinting, landing jumps). The authors acknowledge that this assessment has limits, however, it has the advantage of estimating the soccer player’s ability to perform the specific demands that await them when returning to the team.
Repeated Sprint Ability (RSA)
Metabolic energy reserves are essential during recovery.82 Indeed, the athlete’s physiological abilities will impact the quality of RTP. The RSA test represents a reliable assessment that can be adapted to the majority of team sports. This test assesses the athlete’s ability to repeat maximum efforts with quality by measurement of the difference between the ideal performance area and the actual area (distance and volume) of the RSA achieved. The maximum speed the player achieves can be quantified via GPS. In addition, there is a strong correlation between the result of the RSA Test and VO2max and the athlete’s oxidative power, a key performance factor in soccer.83,84 In the literature, the results of this test are between 6 to 12 efforts of 20 to 40m with 30 seconds of recovery.
Dual Task
Optimal training of an athlete will assist the player to evolve from a situation with control to a situation where they will readily adapt to chaotic environments.85 Need another sentences here, about how one gradually increases the chaos? (before you get to the “last stage”……)The last stage (maximum chaos) is divided into two parts with partial integration into the team and then full integration into the team environment.85 This is an essential moment in the rehabilitative process because cognitive demand is very high. The athlete will be required to manage their own body in space but also the ball, teammates, opponents, and instructions from the coach. This increasing cognitive load can disturb the neuromotor control of the athlete if the motor patterns are not automatic.86,87 This is especially important during movements that require deceleration, cutting or landing, commonly occurring during sequences of play with high uncertainty, such as a defensive or pressing situations.80 A loss of biomechanical quality of knee valgus control or trunk lateral flexion can be directly related to an increased risk of ACL injury.88
It is important to put the athlete in a situation of dual tasks and to assess the quality of movement.85,86,88 If a major deterioration occurs during dual-task conditions, what will happen in a complex cognitive context as indicated above? This concept is therefore considered during match simulation (during cutting with uncertainty, 1 vs 1), as well as in via the single limb landing test with impaired visual input. This is a first level of assessment of the cognitive aspect related to the dual task, information processing and decision-making. However, it must be noted that the level of complexity of the proposed analysis tasks is lower than the multiple cognitive demands that occur during a game situation.
Workload
To optimize recovery, the athlete’s ability to support the daily and weekly training loads of their competition group and her/his position should be highlighted.89–93 Indeed, it is recommended that to optimize the RTP and athlete should be albe to support approximately 90% of the workload of the highest load of the highest session workload of the week of their training group.93 This is the athlete’s ability to progress group training while maintaining both the quality of neuromotor control during dynamic movements in the game, acceleration levels, speed, and the quantitative aspect related running distances and training intensity.
There are many methods for workload assessment. The Foster method is the most common for evaluation of the internal load.94 Regarding the external load, GPS analysis is the most commonly used measure, assessing the number of acceleration, deceleration, cutting, and jumping tasks that occur, as well as distances covered at the various speed intervals.
Deceleration
Current video analysis studies of ACL injuries have identified pressing and tackling as the most common patterns for ACL injury in soccer. Pressing is a situation that leads to the demand for sudden deceleration. It seems important to assess the biomechanics during decelerations, in particular kinematics hip adduction and knee abduction.95,96
However, there is a difference between the literature and clinical practice, as most authors analyze the biomechanics of deceleration using a force platform integrated into the ground and several cameras.95,96 Such analysis is not possible on the field of play. It is possible to measure this deceleration via GPS revealing the intensity and distance of the athlete’s braking.97,98 Fortunately, latest generation smartphones can collect slow motion from 120 to 240 frames per second. The biomechanical analysis can then be performed with free software such as Kinovea®, whose reliability and validity have been demonstrated.
Agility Tests
It is commonly advised to assess the movement qualities during specific movements. There are agility tests for this: the Modified Illinois Agility Test, the AFL Agility run test, the T-test, the Reactive shuttle agility run, the new curve sprint test, and the zigzag agility run, for example Each of these tests involves analysis of the athlete’s ability to express their neuromuscular capacities in a context of dynamic movement with greater specificity to their discipline and to the demands they will encounter during RTP.99 The T-test requires acceleration, in particular the rate of force development, which is the quality most impacted by ACL injury,100 deceleration, but also the ability to make 90° cuts and backpedal at maximum intensity while maintaining postural control.
The new curve sprint test (Figure 3) is similar to the sprints found in team sports and in particular in soccer, which requires asymmetrical movement of the athlete at maximum intensity, knee-trunk control, and contributions of the ankle-foot complex.101 Researchers have shown that during soccer game, players mainly repeat sprints of less than 10m but more than sixty times.102,103 Caldbeck showed that sprints were rarely in a straight line, but in 85% of cases curvilinear.104 Hence, to once more closely approximate the reality on the field, the authors recommend the use of a test recently developed by Filter et al.101 called the curve sprint which is characterized mainly by its reliability, specificity and simplicity, it can be performed easily and precisely in the arc of the penalty area, within a radius of 9.15m and over a distance of 17m. The athlete must perform two sprints in one direction then two sprints in the other direction.

Fatigue
Van Melick et al. highlighted a reduction in quality of jumping tests which under fatigue conditions and is seen in athletes who had ACLR compared to healthy subjects. Studies are contradictory concerning the role of fatigue in the risk factors of ACL injury106–110; however, it may be important to assess the player under fatigued and non-fatigued conditions. A significant deterioration in quality and/or performance with fatigue should at least inform the professional regarding the athlete’s current ability to RTP at the same intensity as before the injury. Therefore, the authors recommend carrying out hop tests on the field in an ecological condition. The landing test should be performed with a force platform in a non-fatigued state and then in a fatigued situation53,99 after the training session including RTP and agility tests. These landing tests are each time carried out in single and dual task conditions.65,86 The impact of fatigue can also be analyzed during a game simulation, both from a qualitative (neuromotor control of movement) and quantitative (activity intensity) point of view.
Horizontal Force - Velocity Profile
Sprint force-velocity profiling is a subject of growing interest to inform the RTP, especially in soccer players. These profiles may contribute strongly to the production of the horizontal component of the reaction force on the ground111 and therefore influence the lower limb theoretical maximal force (F0) capabilities . Mendiguchia et al. found a decrease in maximum horizontal power with an ability to produce force at the start of the acceleration phase, 20% deficit after injury while the value of F0 was almost unchanged.112 These authors have hypothesized that this deficit could be the cause of mechanical overload in the hamstring. Therefore, players who have ACLR with a hamstring graft should benefit from this assessment.
Soccer players must sometimes combine running at high speed with a non-linear trajectory, for example while driving the ball and cutting. Baena-Raya et al.113 were interested in the potential relationship between the variables of the individual force-velocity profile and the ability to cut. They report that the variables F0 and the lower limb maximal power (Pmax) capabilities were strongly associated with performance during changing direction in soccer.113 These authors showed that the ability to orient the ground reaction force vector horizontally (RFmax) was associated with enhanced performance on cutting tests.
IS NEUROMOTOR CONTROL THE KEY?
External and internal pressures may include a combination of spatiotemporal constraints, differing levels of cognitive complexity, and fatigue. These scenarios will impact the athlete’s ability to execute a movement task effectively and may also predispose them to positions associated with heightened injury risk. During the most intense and demanding moments on the field, athletes may only have milliseconds to scan the surrounding environment and decide upon and execute an appropriate movement.
Perceptual and cognitive load must be viewed with the same level of importance as the physical components of performance toward which the rehabilitation professional devotes much rehabilitation time.
Optimal movement technique and appropriate training load are important in both the gym and on the pitch, and the focus should not solely be on reaction and response time, but rather also include accuracy and error rate (inappropriate execution of movement in response to a specific stimulus) Monitoring an athletes’ agility success rate during progressively greater game-like training scenarios may provide practitioners with an enhanced appreciation of the player’s readiness to train; this is also an important avenue for future research. The effect of motor task difficulty on cognitive performance as an error rate can be masked with a delay in reaction time and can increase injury risk for the athlete. Therefore, simultaneous assessment of reaction time and error rate can provide a broader understanding with regard to cognitive effects on performance during complex tasks that require dual tasking, which present in most, if not all sports.
A greater number of decision-making scenarios and shorter time periods to react to those decisions are some examples that might contribute to ACL injury and should be considered by clinicians after surgery, during rehab scenarios. Future research into injury mechanisms should also consider the contextual factors surrounding the injury to ensure the chaotic complexity of match play is at the forefront of discussion.114–116
CONCLUSION
Clearly, strength, neuromotor agility, psychological, and cardiovascular fitness are required for a safe RTP, and authors have suggested that ecological situations used to study these parameters are important to implement. Novel concepts are highlighted regarding assessments for both clinical and field measurement use, which together capture a more complete picture of neuromotor control in the athlete. Neuromotor control is crucial in terms of the quality of movement, whether during specific and analytical tasks, or tasks with cognitive load, and those that occur in a situation of fatigue. Assessing facets of neuromotor control in standardized or ecological situations with reproduction of the cognitive load required during participation is key to a safe RTP.
COI STATEMENT
The authors declare that they have no competing interests.