
INTRODUCTION
Basketball is one of the most popular youth sports worldwide.1 In the United States, basketball is the most popular sport among boys and girls aged 12-17 years and, in Brazil, it represents the sixth most practiced team sport among Brazilians aged 15-19 years.2,3 As a physical activity, basketball provides a myriad of physical, mental and psychosocial health benefits to these age groups, but it also imposes a risk of sustaining an injury during participation.4–7 The incidence of basketball-related injuries (BRIs) varies depending on factors related to the investigated population – age, sex, level of participation – and the injury definition adopted by the study authors, but according to prospective cohort studies and a recent systematic review, the vast majority of BRIs affect the lower limbs.8–12
The prevention of lower limb injuries has become a topic of great concern in basketball.2 The identification of modifiable risk factors is an important step for injury prevention.13,14 In basketball, two commonly reported risk factors for lower limb injuries are landing technique and ankle-dorsiflexion range of motion (ROM), and previous studies recommended the application of specific screening methods to evaluate these variables among basketball athletes.15,16 Two of those methods include the Landing Error Scoring System (LESS) and the Weight Bearing Lunge Test (WBLT), which have already proven their validity and reliability for evaluation of landing technique and ankle-dorsiflexion ROM, respectively.17,18
Despite the use of these screening methods, the influence of landing technique and ankle-dorsiflexion ROM on injury risk is unclear. A previous case-control study conducted with high school and collegiate athletes of eight different varsity sports found no relationship between LESS score and the risk of sustaining an anterior cruciate ligament (ACL) injury, but a more recent prospective cohort study showed that a LESS score of < 5 significantly increased the risk of sustaining an ACL injury among elite-youth soccer athletes.19,20 Studies addressing the role of ankle-dorsiflexion ROM on injury risk also show inconclusive results. A prospective cohort study conducted specifically with youth basketball athletes showed an association between lower ankle-dorsiflexion ROM and the risk of developing patellar tendinopathy.21 Regarding lateral ankle sprains, a case-control study conducted with collegiate athletes found an association between greater ankle-dorsiflexion ROM and the risk of sustaining recurrent lateral ankle sprains,22 but a previous prospective cohort study conducted with army recruits showed that the occurrence of lateral ankle sprains was associated with a reduction in ankle-dorsiflexion ROM.23
The sport and age of the investigated athletes are important reasons for these observed divergencies.20,22 To move the research forward, it is important to investigate these variables among athletes of different ages and sports. Considering the high lower limb injury rate in basketball, the purposes of this study were to describe the period prevalence of BRIs and (2) to examine the association of the history of lower limb injuries with landing technique and ankle-dorsiflexion ROM asymmetry among youth basketball athletes.
METHODS
Study design and participants
This cross-sectional study was developed in association with a state basketball federation in Brazil. The state basketball federation aimed to enhance injury prevention efforts among youth athletes affiliated with the organization. The investigation of the history of BRIs and the evaluation of landing technique and ankle-dorsiflexion ROM by using two screening methods were proposed as a first step. The objectives were presented to the basketball teams during the 2018 pre-season conference and all youth basketball teams competing in the 2018 state basketball championship were invited to participate in the study. Training and match locations were visited by the researchers in previously scheduled days to recruit athletes to participate. Recruitment and data collection occurred between February and July 2018. Eligibility criteria included (1) youth athletes of both sexes, (2) aged between 10 and 19 years old. Professional athletes were not included in the study. Youth athletes who were not able to complete ankle-dorsiflexion ROM and/or landing technique evaluation due to any physical complaint were included in the study, but they participated only by completing the baseline questionnaire. All participants and their parents or legal guardians, for athletes younger than 18 years old, signed a consent or assent form prior to inclusion in the study. The study was approved by the Ethics Committee of the Universidade Federal de São Paulo (number 2880146).
Data collection
Data collection was accomplished in two steps. First, athletes completed a paper-based questionnaire to investigate personal characteristics, training characteristics, and their history of BRIs in the prior three months. In the second step, athletes performed landing technique and ankle-dorsiflexion ROM evaluation in a random order. Data collection occurred after training sessions or official matches, providing a minimum period of ten minutes rest between the end of the activity and the beginning of the evaluations.
Baseline questionnaire
The baseline questionnaire was completely self-reported and composed of open-ended and closed-ended questions. The initial version of the questionnaire was developed by the first author of the study and later discussed and validated by all the authors in a roundtable discussion. Variables related to personal characteristics (age, sex, height, weight), training characteristics (sport experience, sport specialization, frequency and duration of practice sessions) and history of BRIs in the prior three months were collected. The investigation of the history of BRIs was carried out through two open-ended questions about the type and the anatomical location of injuries. Subsequently, all self-reported injuries were categorized by two of the authors of the study based on the first two digits of the classification The Orchard Sports Injury Classification System (OSICS) Version 10.24 Any disagreement was solved by a third author of the study. The adopted injury definition during data collection was “any physical complaint sustained by a player that resulted from a basketball match or basketball training, irrespective of the need for medical attention or time loss from basketball activities”.25
Landing technique evaluation
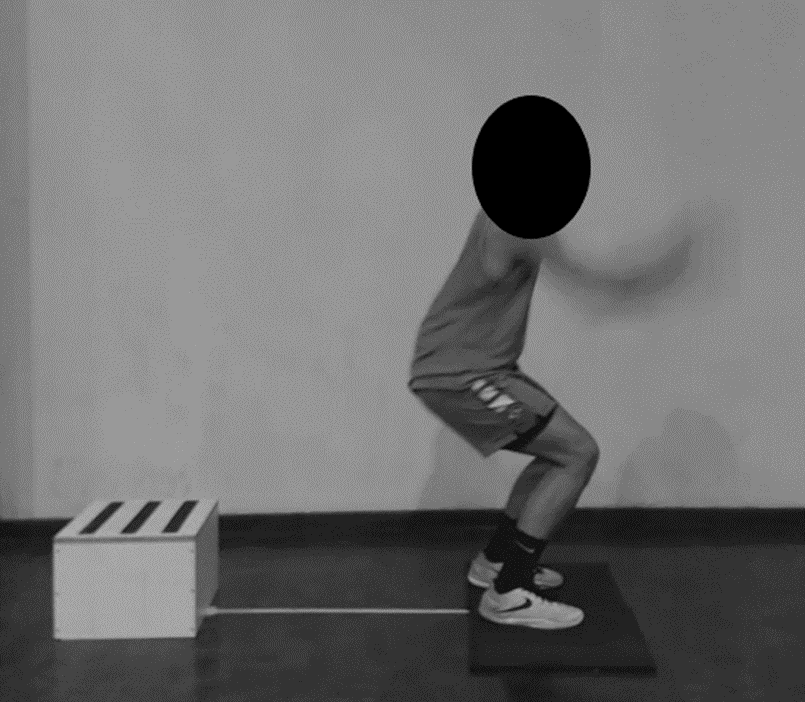
The Landing Error Scoring System (LESS) was used to evaluate landing technique.17 All athletes received instructions and observed a test demonstration prior to the start of the assessment. Test procedures followed the description made by Padua et al.17 Athletes were positioned on a 30-cm-high box and instructed to jump horizontally towards a rectangular landing area – 100-cm-long, 50-cm-wide, and 1-cm-high – positioned at a distance of approximately 50% of their height in front of the box. Immediately after landing, they had to jump vertically as high as they were able and land again on the platform (Figure 1). Athletes completed at least three repetitions for familiarization with the jumping-landing task, which were followed by three valid trials. All valid trials were captured by two webcams (Logitech C920 Hd Pro Full Hd 1080p) placed at a distance of 3.5 m from the lens of the webcams to front of and to the side of the landing area. Both webcams were positioned on a tripod fixed at a height of 1.2 m from lens to floor. The webcams were connected to two independent notebooks and synchronized to the software provided by the manufacturer (Logitech Webcam Software, version 2.80.853.0a).

The jump was considered valid when the athlete (1) jumped from the box with both feet simultaneously, (2) jumped forward and did not perform an excessive vertical movement to reach the landing platform, (3) landed with the entire feet on the platform and (4) completed the task in a fluid motion.17
The authors did not provide any instruction to athletes regarding their landing technique during the test unless they were performing the test incorrectly. All examiners were physiotherapists who had participated in a previous two-hour training session, where they received theoretical and practical instruction about LESS.
After data collection, in a second step, the videos were analyzed by three of the study authors, who were blinded to injury history. Intrarater and interrater reliability were estimated prior to the beginning of the analysis. For reliability analysis, the authors independently scored 24 jumping-landing task videos from eight different athletes at two time points, separated by one week. The intraclass correlation coefficients (ICC’s) were estimated based on a mean-rating, consistency, 2-way mixed-effects model. The ICC’s for intrarater and interrater reliability were 0.87 and 0.81, respectively.
The software Kinovea for motion analysis (version 0.8.15; Copyright 2006-2011 - Joan Charmant & Contrib.) was used during all the LESS analysis. The raters gave scores to each of the three valid attempts completed by each athlete and the final score was represented by the average value obtained in the three attempts. All LESS items were assessed bilaterally, and a preferred limb was not chosen for the analysis. The score for each item was awarded in cases where the athlete presented the landing error in at least one of the valid attempts made, regardless of whether the error was observed in only one or both lower limbs, in the cases of the items assessed bilaterally.
Ankle-dorsiflexion range of motion evaluation
Weight-Bearing Lunge Test (WBLT), as described by previous authors, was used to evaluate the ankle-dorsiflexion ROM.18,21–23 A one-meter tape line was drawn on the floor and continued up to the wall for one more meter. Athletes were positioned with their heel and second toe aligned on the line. After positioning, the athlete was instructed to lunge forward to touch the vertical line in the wall with their knee, while maintaining foot alignment and heel contact with the floor. The evaluated foot was gradually moved away from the wall until the athlete was able to make only a slight contact with their knee on the vertical line. At that moment, ankle-dorsiflexion ROM was measured placing a smartphone 10 centimeters below the proximal region of the tibial tuberosity (Figure 2). The Ankle-dorsiflexion measurement was performed using the iHandy Level app (iHandy Ltd.), which is a valid and reliable tool for joint angle measurement.26 Lower limbs were randomly evaluated, and the final score was represented by the ankle-dorsiflexion ROM asymmetry observed.

All raters were physiotherapists who had participated in a previous two-hour face-to-face training where they received theoretical and practical instruction on the test. Raters were blinded to the presence of injury history during data collection. We did not conduct an intrarater and interrater reliability analysis of the measurements for ankle-dorsiflexion ROM before data collection.
Statistical analysis
All youth basketball teams affiliated with the state basketball federation were invited to participate in this study and a convenience sample of youth athletes was utilized to describe the three-month prevalence of BRI, landing technique and ankle-dorsiflexion ROM asymmetry in this population.
Descriptive statistics were used to present the distribution of the investigated variables. Shapiro-Wilk test was used to verify the distribution of the data. An univariate analysis, using Independent Student’s t-test and Mann-Whitney test, was conducted to verify differences in LESS scores and ankle-dorsiflexion ROM asymmetry between athletes with and without history of lower limb injuries. Additionally, binary logistic regression was used in a multivariate analysis to investigate the association of the investigated variables with the presence of history of lower limb injuries among the athletes. Covariates and variables identified as associated factors in previous studies were used in the model. The model was adjusted considering multicollinearity and goodness-of-fit. The results were presented as odds ratios (OR) and 95% CI. For continuous variables the ORs indicate the change in odds for a one-unit increase in the independent variable. P-values less than 0.05 were considered statistically significant. The software Jamovi (version 1.6.21.0) was used for the analysis.
RESULTS
One hundred and forty-three male and female youth basketball teams belonging to 44 clubs participated in the 2018 state basketball championship. The state basketball championship categorizes youth by age to form the teams. Male competitions were played in seven categories: U-12 (17 teams), U-13 (20 teams), U-14 (17 teams), U-15 (17 teams), U-16 (16 teams), U-17 (13 teams) and U-19 (14 teams). Female competitions were played in five categories: U-13 (five teams), U-14 (four teams), U-15 (six teams), U-17 (nine teams) and U-19 (five teams).
In total, 540 athletes were recruited to participate in the study. After checking and confirming the eligibility criteria, 534 athletes belonging to 42 teams from 23 clubs were included in the final sample. Six athletes were not included because they were also members of the professional teams in their clubs.
All participants completed the baseline questionnaire. Landing technique and ankle-dorsiflexion ROM assessments were completed by 448 and 500 athletes, respectively. However, LESS results of 86 athletes were not included in the final analysis due to technical problems with the quality of the videos and / or execution errors identified during the analysis, which invalidated one or more jumps performed by the athlete.
Characteristics
The majority of the participants were male (88.7%; n = 474). The median age of the athletes was 12 (IQR = 2) years old and 77.5% (n = 414) of them reported basketball as the only sport modality in which they participate. Detailed information about athletes’ characteristics is described in Table 1.
Prevalence of Basketball-related Injuries
The three-month prevalence of BRIs was 23.2% (95% CI 19.7 – 27), with 158 injuries sustained by 124 athletes. Sprains were the most frequent type of injury (29.1%; n = 46) (Table 2).
The ankle (30.4%; n = 48) and knee (21.5%; n = 34) were the most affected anatomic locations (Table 3). Lower limb injuries accounted for the majority of the reported musculoskeletal injuries (69.7%; n = 110) and the three-month prevalence of lower limb musculoskeletal injuries was 17.2% (95% CI 14.1 – 20.7).
Landing Technique and Ankle-dorsiflexion Range of Motion
The mean LESS score among the investigated athletes was 5.45 (± 2.34) points. There was no statistically significant difference between LESS scores in the groups with and without a three-month history of lower limb injuries (p = 0.167) (Table 4).
The median ankle-dorsiflexion ROM obtained was 37.2° (IQR 9.1°). There was no statistically significant difference between the ROM asymmetry values obtained by the groups with and without a three-month history of lower limb injuries (p = 0.961) (Table 5).
Factors associated with Lower Limb Injuries
Table 6 describes the results of the multivariate analysis. Binomial logistic regression model showed that the category of the athlete was the only factor associated with the presence of a three-month history of lower limb injuries. LESS score (p = 0.105) and ankle-dorsiflexion ROM asymmetry (p = 0.529) were not associated with the presence of a three-month history of lower limb injuries.
DISCUSSION
The aims of this study were to describe the period prevalence of BRIs and to examine the association of lower limb injuries with landing technique and ankle-dorsiflexion ROM asymmetry among youth basketball athletes. The three-month prevalence of BRIs among the investigated athletes was 23.2% and the majority of the reported injuries affected the lower limbs. The ankle and knee were the most common anatomical locations affected by injuries and sprains were the most common type of injury. There was no association of landing technique and ankle-dorsiflexion ROM asymmetry with the history of lower limb injuries. Multivariate analysis showed that the category – meaning youth athletes were categorized by age for competition – was the only variable associated with the history of lower limb injuries.
Two previous studies conducted with youth basketball athletes found different period prevalence of BRIs, with values varying from 19.6% to 39%.27,28 The prevalence of BRIs may vary according to injury definition, seasonality of data collection, population characteristics and recall bias. Both previous studies adopted a ‘time loss’ injury definition and investigated a one-year prevalence of BRIs among youth basketball athletes with a similar mean age, but the level of participation and the weekly basketball exposure of the athletes varied across the studies. According to the age category, some athletes tend to present a greater probability of suffering a BRI. Pappas et al. also found an increase in injury rates for the five most common basketball injuries presenting to emergency departments when comparing 7- to 11-year-old category to 12- to 17-year-old category.29 One possible explanation for this difference is an increase in total exposure and intensity of basketball activities and findings of the multivariate analysis may offer support for this hypothesis.29,30 Leppänen et al. investigated competitive athletes participating in basketball activities for 9-10 hours/week and Vanderlei et al. investigated boys and girls participating in a sport initiation program – with a low level of training and competitiveness – during 6-7 hours/week.27,28 A broader injury definition was adopted in this study to investigate the three-month prevalence of BRIs in a sample of competitive athletes, but the injury prevalence found was similar to that reported by Vanderlei et al.27 It may have occurred because the recall period was lower, and the majority of the participants were from categories of initiation in competitive basketball – U-12 and U-13 – and presented a low weekly basketball exposure. A three-month recall period was adopted to reduce the influence of recall bias that may have affected prevalence estimations, but on the other hand this choice increased the influence of the seasonality of data collection in the results. Data collection was conducted during the beginning of the 2018 regular season and the three-month recall period included off-season months. Regarding anatomical location and type of the reported injuries, the current findings are similar to those reported in a recent systematic review and two prospective cohort studies conducted with high school and collegiate athletes. These studies results indicated that the majority of the BRIs affected the ankle and knee, and sprains were the most common type of injury.10–12
There was no association between landing technique and ankle-dorsiflexion ROM and the history of lower limb injuries. These associations are not well established in the literature. Smith et al. found no association between LESS scores and ACL injuries among high-school and collegiate athletes of eight different sport modalities, but Padua et al. showed that a LESS score > 5 was associated to an increased risk of sustaining an ACL injury specifically among elite-youth soccer athletes.19,20 In the present study only basketball athletes were investigated, and the outcome was not ACL injury. Mean LESS score for total sample was 5.34 and both groups – with and without history of lower limb injuries, had a mean LESS score > 5. Regarding ankle-dorsiflexion ROM, three previous studies identified an association between ankle-dorsiflexion ROM, measured using the WBLT, and lower limb injuries. Backman and Danielson prospectively investigated youth basketball athletes and showed that an ankle-dorsiflexion ROM < 36.5° were associated with an increased risk of developing patellar tendinopathy during the season.21 In a case-control study conducted with collegiate athletes of eight different modalities, Kobayashi et al. found that an ankle-dorsiflexion ROM > 49.5° were associated with an increased risk of suffering recurrent lateral ankle sprain, but, on the other hand, a large prospective cohort study conducted with army recruits showed that an ankle-dorsiflexion ROM < 34° was associated with a five-fold risk of suffering a lateral ankle sprain.22,23 Based on these results, it is unclear if restriction of or excess of ankle-dorsiflexion ROM are associated with the occurrence of lower limb injuries. All three previous studies used the absolute ankle-dorsiflexion ROM value as the outcome. In the present study, ankle-dorsiflexion ROM asymmetry was adopted. Mean ankle-dorsiflexion ROM asymmetry for total sample was 2.30 and there was no difference when comparing the group with and without history of lower limb injuries. Absolute ankle-dorsiflexion ROM may be a more relevant variable to be further investigated. Age, sex, sport, and the injury defined as the outcome are potential factors that could influence this association.19,20 This study investigated only basketball athletes and participants were younger than the athletes investigated in these three previous studies. The majority of them were beginning in competitive basketball with a low weekly basketball exposure. Additionally, the outcome was lower limb injuries in general and not restricted to ACL injuries, patellar tendinopathy, or lateral ankle sprains. LESS and WBLT were proposed and previously investigated as screening tools for specific lower limb injuries, but the statistical power did not enable the consideration of these specific injuries as the outcomes in the current analysis.15,16 Statistical power was cited as a limitation by the authors of a previous study, and they raised the need for multicenter initiatives to better elucidate these associations.19
This study described the prevalence of BRI’s and investigated landing technique and ankle-dorsiflexion ROM among a large sample of youth athletes from a specific sport. Regardless of these strengths, the study has some limitations. First, a cross-sectional study is not the ideal study design to measure injury rates and describe injury patterns due to the seasonality of data collection. Additionally, the associations found in a cross-sectional study are subjected to reverse causation and cannot establish causal relationships between the investigated variables and the occurrence of lower limb injuries. Second, a broader injury definition was adopted, all BRIs were self-reported and, due to recall bias, athletes were more prone to report substantial injuries and to potentially forget minor complaints. For ankle-dorsiflexion ROM evaluation, although previous face-to-face training on data collection procedures was conducted, it was not possible to conduct a reliability analysis of the raters because data collection occurred in different locations and had a different set of raters in each location. Ankle-dorsiflexion ROM asymmetry was used as the outcome because the laterality of the injuries was not collected. Previous studies adopted the absolute ROM of the affected limb as the outcome of the analysis which may affect the association.21–23 Lastly, although broader inclusion criteria were established, the majority of the sample was composed by male athletes from U-12 and U-13 basketball teams. All male U-12 basketball teams and 75% of the male U-13 basketball teams affiliated with the State Basketball Federation were investigated, but difficulties recruiting female and older male athletes reduced the external validity of the current findings.
Establishing the epidemiology and modifiable risk factors for injuries are essential to inform the development and the implementation of injury prevention interventions among different group of athletes.13,14 These results may influence future studies including prospective investigations to bring more solid data about the epidemiology of BRIs among youth basketball athletes and to better elucidate the role of landing technique and ankle-dorsiflexion ROM as risk factors for lower limb injuries in this population. For clinical practice, although the current prevalence data is insufficient, in the absence of large prospective cohort studies, these results may be useful for clinicians to direct their injury prevention efforts for the most common BRIs observed among youth basketball athletes. Finally, clinicians should be cautious to infer the injury risk of youth basketball athletes solely based on the results of screening tests, such as LESS and WBLT. Screening tests may be applied, but we need to consider the multicausality of sports-related injuries and the predictive capacity of these tests when interpreting their results.
CONCLUSION
The three-month BRIs prevalence among youth basketball athletes was 23.2%. Although ankle sprains were the most frequent injury, landing technique and ankle-dorsiflexion ROM asymmetry were not associated with the history of lower limb injuries. The age category of the athlete was the only variable associated with the history of lower limb injuries.
Competing interests
The authors declare that they have no competing interests in the subject matter or materials discussed in this manuscript.