INTRODUCTION
Baseball is one of the most popular sports in Japan, and on average, shoulder injuries occur in baseball players at a rate of 13%–35%.1–4 Additionally, it is difficult for an athlete to recover from a shoulder injury and resume their preinjury performance levels. After undergoing surgery for intrinsic shoulder impingement, Peduzzi et al.5 evaluated the effects of getting back into sports. However, 120 of 135 patients (90%) who underwent surgery returned to their athletic activities thereafter, with 52% engaging in the same sports at the same level. Only 48% of pitchers who received surgical therapy for superior labral lesions could resume playing, according to Fedoriw et al.,6 and only 7% of participants maintained their performance level. Considering all these factors, it is important to investigate the risk factors for shoulder injuries, as these are often multifactorial.3,7,8 Among them, repetitive throwing has recently been in focus.3,9 In 2014, the Major League Baseball published the Pitch Smart guidelines.10 These guidelines include specific pitch count limits, such as 120 pitches per day for athletes aged 19–22 years. Additionally, Murray et al.11 showed that the maximum shoulder external rotation angle during pitching decreased because of repetitive throwing. Chou et al.12 found that after 100 repeated tosses by high school baseball pitchers, their shoulder horizontal adduction angles at their maximum shoulder external rotation positions (MER) increased. Escamilla et al.13 reported that shoulder kinematics did not change after 105–135 pitches. According to these studies, there is no agreement on how repetitive throwing alters the shoulder’s kinematics. Few studies have examined how the shoulder kinematics change with repeated throwing; therefore, further research is required.
When someone pitches, motion and energy are transferred from the lower extremities to the upper extremity in what is known as a kinetic chain.14 For the upper extremities to move smoothly and stay injury-free, the thoracic spine, which sits between the lower and upper extremities, must be controlled, which requires strong trunk muscles.15 Aguinaldo et al.16 investigated the connection between pitching-related thoracic movement and shoulder joint strain. In the early cocking phase, Aguinaldo et al.16 suggested that early thoracic rotation enhanced shoulder rotational force and speculated that early thoracic rotation may contribute to throwing-related overuse injuries. Furthermore, according to Douoguih et al.,17 early thoracic rotation during the early cocking phase was linked to a noticeably increased risk of upper extremity injuries that required surgery.
Although thoracic movement control is essential to prevent shoulder injury, changes in thoracic kinematics occur during pitching. Therefore, all adverse effects of recurrent throwing on trunk muscle function should be examined.
This study aimed to determine the effects of pitching repeatedly on the endurance of trunk muscles and kinematics of the thoracic spine and shoulder. After repeated tossing, hypothesized that the trunk muscular function would decline and the throwing action would change.
MATERIALS AND METHODS
Participants
Twelve healthy male recreational baseball players were recruited to participate in this study. Players who had previously injured upper or lower extremities injuries or who had shoulder pain at the time of testing were excluded. The study protocol was approved by the Research Ethics Committee. Informed consent was obtained from all the participants.
Experimental protocol
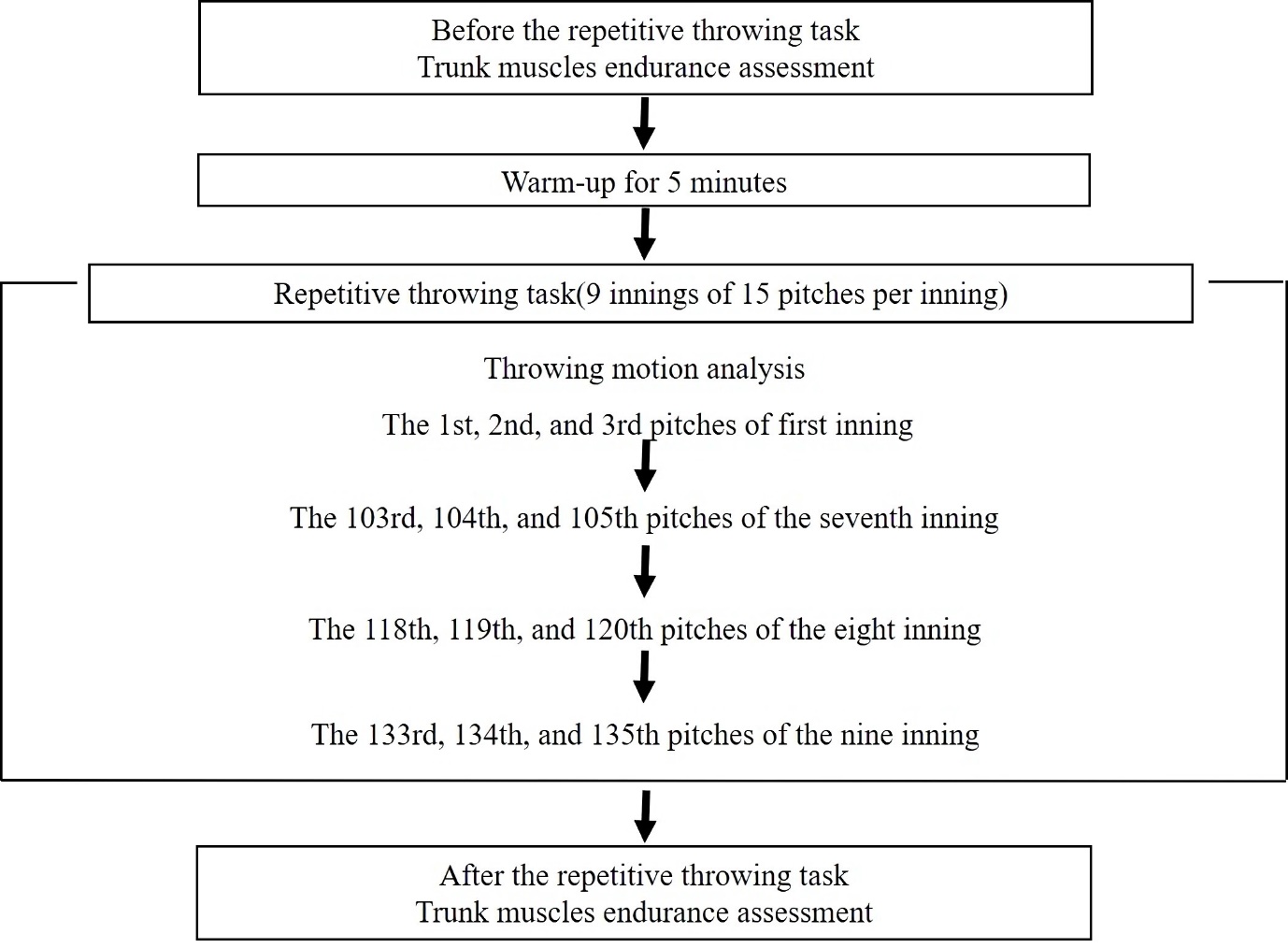
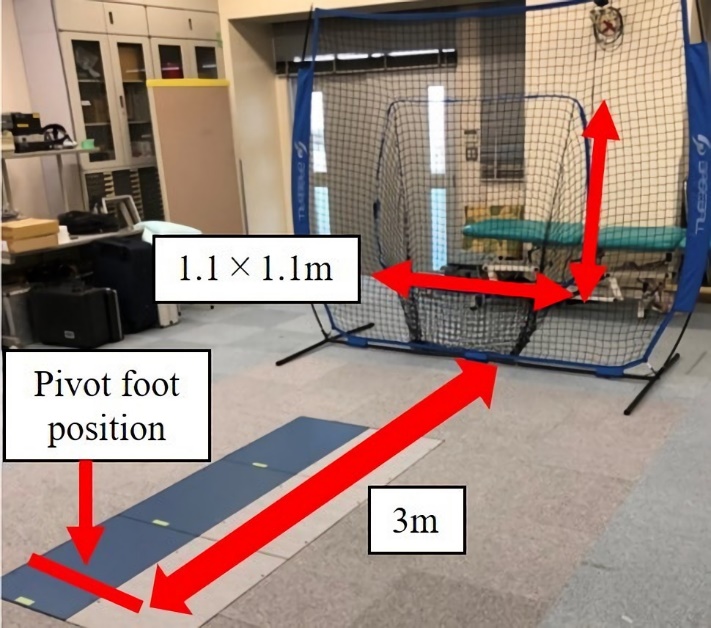
The repetitive throwing task and measurement protocol are shown in Figure 1. The repetitive throwing task was based on the reports of Dale et al.18 and Yanagisawa and Taniguchi.19 All participants were allowed five minutes to warm up and stretch using their preferred routine before the repetitive throwing task (i.e., shoulder and trunk stretching and plyometrics). Next, they threw 135 fastballs (~9 innings with 15 throws per inning at ball intervals of 15 seconds) at maximum effort from the set position toward the target. The distance between the pivot foot of the participants and the target was set at 3 m, and the size of the target was 1.1 × 1.1 m. The target was placed on the extension line of the force plate that was used during 3D motion capture (Figure 2). An official baseball (ZETT Corporation, Osaka, Japan) that weighed 145.0–147.0 g was used during the repetitive throwing task. Five minutes were provided as rest time between each inning.


Before and following the repetitive throwing motion, trunk muscular function was assessed. The throwing motion was monitored during the 1st, 2nd, and 3rd pitches (1st inning), the 103rd, 104th, and 105th pitches (7th inning), the 118th, 119th, and 120th pitches (8th inning), and the 133rd, 134th, and 135th pitches (9th inning). Additionally, the ball speed was measured using a radar gun (Pocket Radar; Pocket Radar Inc., Santa Rosa, CA USA) while assessing the throwing motion. An analysis of ball velocity was performed to ensure that the ball speed had not dropped. Moreover, ball velocity did not drop in all innings (1st inning, 54.1 ± 6.7 mph; 7th inning, 55.6 ± 6.1 mph; 8th inning, 55.6 ± 5.5 mph; 9th inning, 56.9 ± 6.4 mph).
Trunk muscle endurance assessment
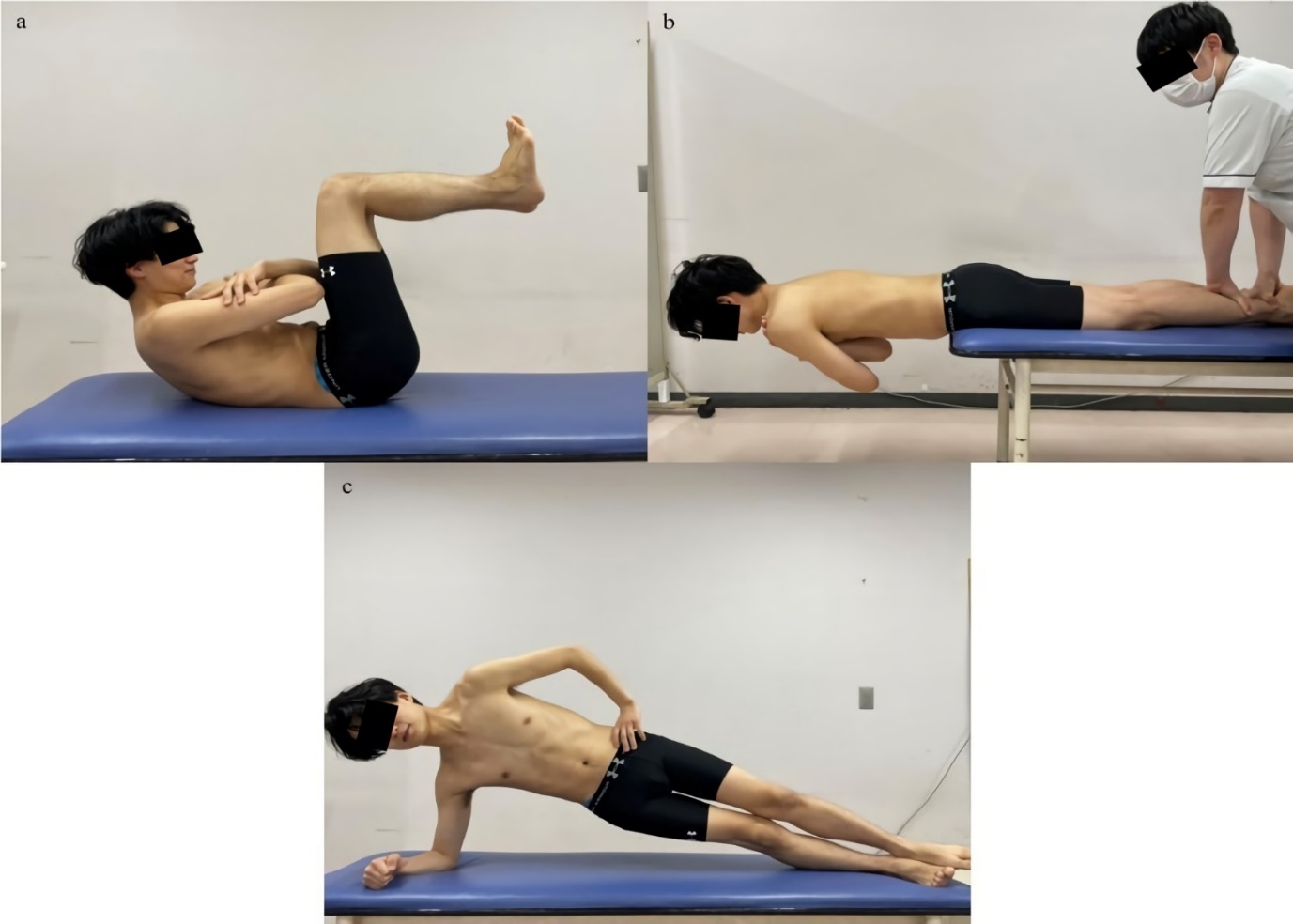
Trunk muscle endurance was measured using a stopwatch (ADME001; Seiko Watch Corporation, Tokyo, Japan) for flexion (Figure 3a), extension (Figure 3b), and throwing and nonthrowing lateral flexion (Figure 3c).20–22 The measurement of trunk muscle endurance used in this study is straightforward, and the reliability of the measurement is high.20,21 The trunk flexion muscle endurance was measured in the supine position with the hips and knees flexed at 90° and arms crossed over the chest. It was timed after the participant bent their trunk so that both elbows met the front of their thighs and when both elbows left the thighs. Trunk extension muscle endurance was assessed in the prone position with the pelvis aligned with the edge of the bed and arms crossed over the chest. The participants kept their trunk parallel to the floor and the time until failure to preserve this trunk position. The trunk lateral flexion muscle endurance was measured in the side-lying position, with the shoulder abducted at 90° and elbow flexed at 90°. Participants maintained a straight position, and the duration between failures to maintain these postures failures were recorded.

Motion analysis
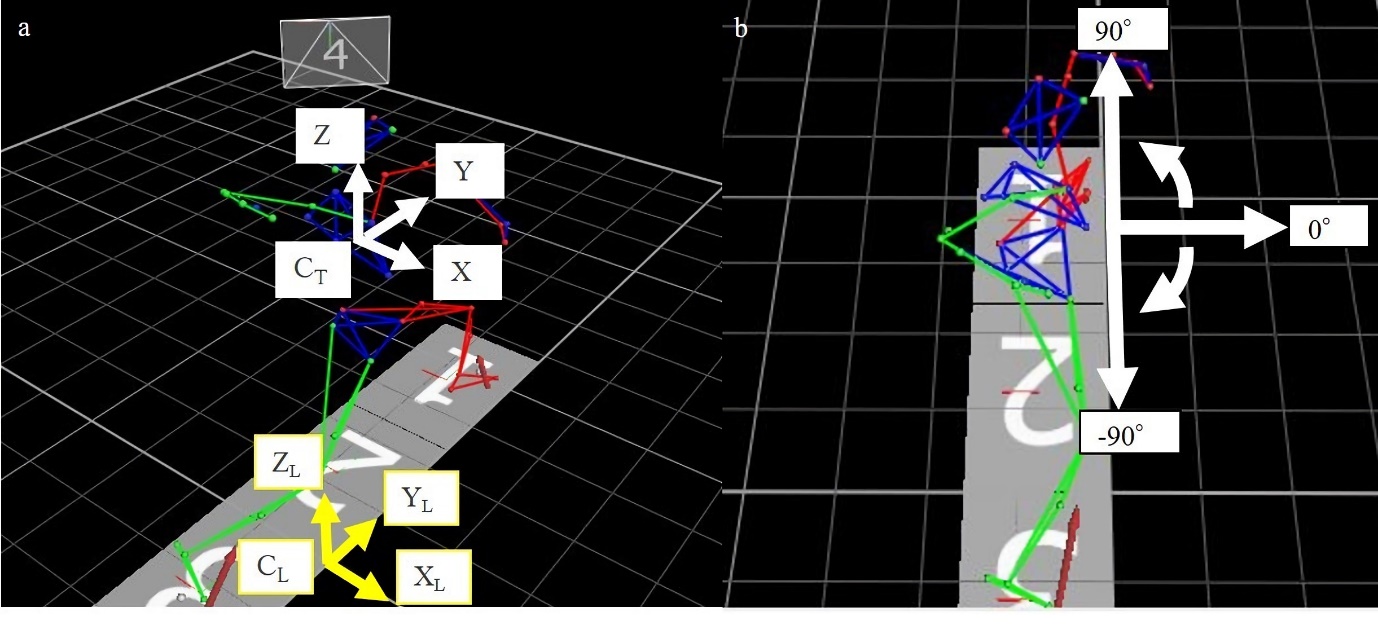
Throwing motions were measured using a three-dimensional motion analysis system (Vicon MX; Vicon Motion Systems Ltd., London, UK), which utilizes nine infrared strobe cameras and two force plates (BP400600-OP-2K-STT; Advanced Mechanical Technology, Inc., Watertown, MA, USA). Data were captured at 1000Hz, and force plate data were collected at 1000Hz. Thirty-nine reflective markers were fixed to anatomic landmarks according to the Plug-In Gait model (Vicon Motion Systems Ltd.) (spinous process of the 7th cervical vertebra, spinous process of the 10th thoracic vertebra, sternal notch, xiphoid process, right scapula, bilateral anterior/posterior head, acromioclavicular joint, lateral upper arm, lateral humeral epicondyle, lateral forearm, radial/ulnar styloid, second metacarpal head, anterior/posterior superior iliac spine, lateral thigh, lateral femoral condyle, lateral shank, lateral malleoli, second metatarsal head, and calcaneus). The thoracic angles (anterior/posterior tilt, throwing/nonthrowing side lateral tilt, and nonthrowing/throwing side rotation) and shoulder angles (horizontal adduction/abduction, abduction/adduction, and internal/external rotation) at stride foot contact during the early cocking phase (SFC) and at the maximum shoulder external rotation position during the late cocking phase (MER) were calculated based on the Vicon Plug-In Gait model.23 The SFC was defined as the instant when the vertical ground reaction force from the nonthrowing side foot exceeded 10 N, and the MER was determined using the joint angle data.24 Marker trajectory data were low-pass filtered using a fourth-order Butterworth filter with a cutoff frequency set at 13.4 Hz.25 The axes were defined as follows: the Y-axis extended toward the pitch, the X-axis extended from the first base toward the third base and was orthogonal to the Y-axis, and the Z-axis was perpendicular to both the Y- and X-axes. The thoracic angle was defined as the absolute angle of the thoracic segment to the laboratory axis (Figure 4). The shoulder adduction angle was defined as the angle between the thoracic segment and the upper arm segment.

Statistical analysis
IBM SPSS Statistics, version 23 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Shapiro and Wilk’s W-statistic was used to screen all data for normality of distribution. The paired t-test or Wilcoxon signed-rank test was used to compare trunk muscle endurance before and after throwing, depending on whether normality was present or not. The changes in kinematics were analyzed in innings 7, 8, and 9, depending on normality, and the significance level was adjusted by Bonferroni analysis for multiple comparisons. Statistical significance was set at p < 0.05. Effect sizes and 95% (CI) between each measure were also calculated. Effect sizes (Cohen’s d) using the paired t-test were rated small (0.20≤d<0.50), moderate (0.50≤d<0.80), and large (d ≥ 0.80).26 Effect sizes (r) using the Wilcoxon signed-rank test were rated small (0.10 ≤ r < 0.30), moderate (0.30 ≤ r < 0.50), and large (r ≥ 0.50).26
RESULTS
Twelve athletes participated in this study (mean age, 22.8 ± 2.9 years; mean body mass, 67.5 ± 8.7 kg; mean height, 170.4 ± 5.4 cm; mean experience, 13.6 ± 1.9 years) (Table 1).
Changes in the trunk muscle endurance before and after repetitive throwing are shown in Table 2. Endurance of the trunk flexors [p = 0.001, d = 1.10 (95% CI: 3.8,10.6)], extensors [p = 0.002, d = 1.30 (95% CI: 3.7,12.8)], lateral flexors on the throwing side [p < 0.001, d = 1.11 (95% CI: 6.0,11.7)], and lateral flexors on the nonthrowing side [p < 0.001, d = 1.76 (95% CI: 7.1,15.7)] was significantly decreased after repetitive throwing.
Table 3 shows thoracic spine and shoulder kinematics at SFC and MER in the first, seventh, eighth, and ninth innings. The thoracic rotation angle at the SFC in the eighth inning was significantly lower than that in the first inning [p = 0.013, d = 0.20 (95% CI: 0.4,3.0)]. The shoulder horizontal adduction angle at MER in the seventh [p = 0.013, d = 0.38 (95% CI: 0.7,4.7)] and ninth [p = 0.004, d = 0.42 (95% CI: 1.1,4.6)] innings was significantly lower than that in the first inning. No differences were found in other variables.
DISCUSSION
Because shoulder injuries related to pitching occur in 13%–35% of baseball players,1–4 and the likelihood of performance recovery is low,5,6 the link between repetitive throwing and shoulder injury has recently come under scrutiny.3,9 There is a lack of consensus agreement on specific changes that repetitive throwing might cause in shoulder kinematics.11–13 While the most agree that good trunk function is essential in controlling shoulder kinematics, the changes in thoracic kinematics and trunk muscle strength related to repetitive pitching are unclear.15 The results of the current study reveal that the trunk muscle endurance diminished and thoracic rotation and shoulder horizontal plane kinematics were altered by repetitive throwing.
Despite studies on how shoulder and hip muscle function changes when throwing repeatedly,19,27 variations in trunk muscle function have not yet been examined. In this line, Mullaney et al.27 showed that shoulder internal rotation strength decreased after about 100 pitches, whereas Yanagisawa and Taniguchi19 showed that hip adduction and abduction strength decreased after 117 pitches. Although the body segments assessed varied, the current study conforms to previous reports.
Hirashima et al.28 examined the rectus abdominis and external oblique muscles activity during throwing using surface electromyography. They showed that the external oblique muscles on the nonthrowing side were active in inhibiting early thoracic rotation during the early cocking phase. In contrast, the external oblique muscles on the throwing side were active to direct the thorax toward the throwing direction during the late cocking phase. However, the rectus abdominis muscle was shown to be active immediately before ball release. The paraspinal muscles have been described as active from SFC to ball release for postural control of the trunk.29 Based on these observations, the authors of the current study hypothesized that abdominals and trunk extensors were engaged to control the thoracic movement during each phase of throwing and that repeated throwing reduced trunk muscle endurance.
Early thoracic rotation at the SFC is one of the thoracic kinematics during throwing that should be focused on since it is frequently linked to shoulder injury.16,17 Although trunk muscle endurance decreases occurred in this trial, the thoracic rotation angle to the nonthrowing side at the SFC did not increase. In healthy participants, the decrease in trunk muscle endurance might not necessarily lead to poor trunk motion, such as early thoracic rotation. However, the thoracic rotation angle at the SFC increased toward the throwing side in the eighth inning. The variations observed in this study do not have therapeutic relevance because no reports demonstrate a connection between the changes in thoracic kinematics exhibited herein and shoulder injury.
The shoulder horizontal adduction angle at MER dropped in the seventh and ninth innings. However, the effect size for the change in shoulder horizontal adduction angle with recurrent throwing was small in this study. Several studies have focused on how repetitive throwing affects the shoulder’s horizontal adduction angle. Chou et al.12 showed that 100 pitches increased the shoulder horizontal adduction angle at the MER in top-level high school baseball players. Conversely, Escamilla et al.13 showed that 105–135 repetitive throws did not change the shoulder horizontal adduction angle in Division I college baseball players. Considering factors that lead to a decrease in the shoulder horizontal adduction angle at MER, Mullaney et al.27 reported that the shoulder internal rotation strength decreased after 100 pitches. Additionally, Dale et al.18 showed that fatigue of the shoulder internal rotator muscles began even after 60 pitches. Throwing repeatedly is likely to reduce the shoulder internal rotation strength because the subscapularis, pectoralis major, and latissimus dorsi muscles are very active from the late cocking phase to the acceleration period.30 Jobe31 considered that a decrease in the function of the shoulder anterior components may contribute to a decrease in the shoulder horizontal adduction angle during the late cocking phase. Furthermore, of the subscapularis, pectoralis major, and latissimus dorsi muscles, the subscapularis and pectoralis major are thought to contribute to the maintaining of the glenohumeral joint horizontal adduction position.30 However, although there were no changes in thoracic kinematics affecting shoulder kinematics in this study, a deficit in muscle function of the anterior shoulder components, such as the subscapularis and pectoralis major muscles, may lead to a change in the shoulder horizontal plane kinematics at MER.
A decreased shoulder horizontal adduction angle at MER is closely associated with shoulder injuries and is a risk factor for posterior superior impingement syndrome.31,32 Posterior superior impingement syndrome is a phenomenon in which the rotator cuff is trapped between the humeral head and glenoid fossa during the late cocking phase.31,32 Mihata et al.33 reproduced the MER position in cadaveric shoulders and reported that the pressure between the greater tuberosity and glenoid increased as the shoulder horizontal adduction angle decreased. In this study, the shoulder horizontal adduction angle at MER decreased in the seventh and ninth innings, suggesting that pitching >100 pitches may contribute to increased mechanical stress within the shoulder.
This study has some limitations. First, the trunk muscle endurance was evaluated using a method that is easy to use in clinical and field situations. However, the technique used in this study could not deny subjectivity. In the future, we should employ a more accurate method of assessment. Second, the throwing motion function was only assessed during specific innings. Japanese starting pitchers often throw more than seven innings, but in the United States, they barely reach this number. Whether the throwing motion will change in less than seven innings needs to be determined. Therefore, assessing pitching data in every inning would be relevant, particularly in American baseball. Third, based on previous reports, the authors speculate that the decreased shoulder horizontal adduction angle at MER increases mechanical stress within the shoulder.31–33 This study only showed changes in shoulder motion with repetitive throwing in healthy participants, and whether a healthy athlete whose shoulder motion is altered by repetitive throwing will develop shoulder injuries in the future remains unknown. If the relationship between changes in shoulder motion with repeated throwing and the incidence of shoulder injury can be clarified, this may lead to preventive actions for future injuries.
CONCLUSION
The results of this study indicate that with 135 repeated throws trunk muscular endurance was reduced. In addition, thoracic rotation at SFC and shoulder horizontal plane at MER kinematics were altered by repetitive throwing.
Funding
This study was not funded.
Disclaimers
No potential conflict of interest was reported by the authors.
ACKNOWLEDGMENTS
The authors would like to thank all the individuals who participated in this study. The authors would like to thank Enago (www.enago.jp) for the manuscript review and editing support.