
INTRODUCTION
Assessing the length of the rectus femoris muscle is a standard part of a lower extremity examination for physical therapists. The rectus femoris is the only two-joint muscle of the quadriceps group, and like many of the other lower extremity two-joint muscles, it can lose muscle length. A shortened rectus femoris muscle is associated with a number of different lower extremity problems including adolescent apophysitis of the tibial tubercle (Osgood-Schlatter’s disease),1–7 rectus femoris muscle strain,8–10 calcific tendinitis of the rectus femoris muscle,11 osteoarthritis of the knee,12–14 as well as anterior knee pain.15–17 Thus, an assessment of rectus femoris length is an important part of a physical therapy examination.
The most commonly described method used to assess rectus femoris muscle length is the Thomas test.18 Only a few researchers have examined the reliability of the Thomas test to assess the length of the rectus femoris muscle. Eng et al. reported “almost perfect” reliability (ICC = 0.94) test-retest reliability for quadriceps femoris muscle angle, but they failed to describe their method of how they measured quadriceps femoris angle or to report what kind of reliability tests were performed, either intra or inter-rater observer agreement.19 Horneij et al. assessed rectus femoris muscle length on 44 nurses or aides with and without back pain using a modified Thomas test, however they only rated rectus femoris muscle length using a nominal measurement scale as either “tight” or “excessive” muscle length.20 In another study, Harvey et al. assessed the length of all of the thigh two-joint muscles, however, the flexibility data was pooled so there is no way to determine observer agreement of any of the specific muscle tests.21 Peeler and Anderson, in an observer agreement study examining the Modified Thomas Test, assessed rectus femoris length measures taken by three athletic trainers and found moderate to fair test-retest intra-rater (ICC = 0.67) and inter-rater (ICC = 0.50) reliability.22 The “moderate” reliability findings may, in part, be due to the difficulty in properly performing the Modified Thomas test. Peeler and Anderson report that the Thomas test can be challenging for clinicians to perform.22 Cady et al assessed rectus femoris length using the Thomas test in 20 healthy men using digital photographs, among six raters, but they did not record goniometric measures and only used a nominal rating of pass or fail.23 Thus, from one suitable study, the reliability of the Modified Thomas test to assess rectus femoris muscle length, was “high” for inter-rater reliability with a Chronbach’s alpha of 0.80.23 A drawback in this study was that used nominal data, which increased their likelihood of agreement.
A current method that is easier for patients to assume and for therapists to perform, that does not stress the lower back or hips is Ely’s test. Ely’s test, used to assess rectus femoris muscle length, is a method that does not include holding the contralateral hip in full flexion, thus making it easier to perform. Peeler and Anderson assessed Ely’s test for inter and intra-rater reliability using measurements taken by three athletic trainers on 54 participants with no history of trauma.24 Their results showed moderate reliability with ICC values of 0.69 for intra-rater reliability and 0.66 for inter-rater reliability.24 However, they only used active, not passive knee flexion, when assessing rectus femoris muscle.24 Olivencia et al. also assessed rectus femoris muscle length using Ely’s test and found good inter-rater reliability (ICC = .90) and good intra-rater reliability (ICC = 0.91).25 But, they also only used active knee flexion to assess rectus femoris muscle length.25 According to Kendall muscle length testing is performed using passive not active movement that increases the distance from the origin and insertion which elongates the muscle in the opposite direction of the muscles action.18 Additionally, a muscle crossing two-joints like the hamstrings, are incapable of shortening sufficiently to produce complete range of knee flexion with the hip extended.18 Thus, the “true” or actual amount of rectus femoris muscle length, and thus the reliability which was recorded in these studies, using Ely’s test is questionable.
Another method similar to Ely’s test was previously described in the literature by Witvrouw et al.26 Witvrouw et al assessed rectus femoris muscle length in athletes with anterior knee pain.26 They described a method where the athlete assumes a prone position placing the contralateral (not measured) hip in a position of 90° of hip flexion to stabilize the pelvis and then flexing the ipsilateral (measured) knee assessing rectus femoris length.26 This position fo assessing rectus femoris muscle length is often easier for patients to assume and easier for therapists to perform the test. An advantage of this test method over Ely’s is that it allows for better pelvic stabilization by preventing unwanted pelvic movement. The new test examined in this study mimics the Thomas test position to some extent by flexing the contralateral hip when lying prone. It may also be desirable in those who are very flexible. When using Ely’s test with flexible patients, full knee flexion can be halted because the heel reaches the buttocks and prevents any further knee flexion. This new test rarely has that problem and can often discriminate left to right rectus femoris muscle length imbalances in flexible patients.
The purpose of this study was to determine observer agreement using a new test for assessment of rectus femoris length. A second purpose was to determine if those with anterior knee pain have different rectus femoris muscle length than those without anterior knee pain.
The authors hypothesized that this new method of assessing rectus femoris muscle length is reliable, and that those with anterior knee pain will demonstrate shorter rectus femoris muscle length than those who do not have anterior knee pain.
METHODS
Participant
Fourteen men and thirty-nine women (N = 53) participated in this study after volunteering through convenience sampling from Maryville University and the surrounding community looking for subjects with and without anterior knee pain. Anterior knee pain was defined as pain in an around the patella without having recent injury or surgery and whose pain level was below 5/10 on a numeric pain rating scale. Demographic data were gathered on all participants. Participants were included if they were between 18 to 65 years of age and could tolerate lying prone for at least 15 minutes. Exclusion criteria: if they could not speak or understand the English language, were mentally disabled, had undergone previous surgery on one or both knees, had recent injury or trauma to either knee within the prior six months (where their knee was assessed by a licensed health care provider), needed an assistive device for gait, had a history of structural problems of the ligaments of either knee (such as sprains due to any causative factor), or were pregnant. The study was approved by the IRB committee at Maryville University in St. Louis, MO.
A flip of a coin was used to determine which side to measure the left (heads) or right (tails) side, to avoid the issue of “double-dipping” the data.27,28 All participants completed a Lower Extremity Functional Scale (LEFS).29 A Numeric Pain Rating Scale (NPRS) was used to assess current, worst, and best pain.30 A high-low treatment table was used for participants to lie on while measurements were taken. A standard 12-inch plastic goniometer was used to measure hip flexion of 90° while in prone position prior to data collection.31
Participants reviewed and signed an informed consent form and were assigned a random participation number used throughout data collection. Eligibility to participate in the study was verified with an inclusion and exclusion, yes or no, questionnaire. The participants’ demographic information was gathered, and the participants were asked to fill out two self-reported measures. The first measure was related to functional ability using the LEFS. Then participants’ pain level was assessed for present anterior knee pain they were having at this time and for their worst pain level perceived in the prior six months on a 0 to 10 NPRS, with 0 = no pain and 10 at its worst. If both knees met inclusion and exclusion criterion, or if both knees had pain, a coin was flipped to determine which knee, left or right, would be measured.
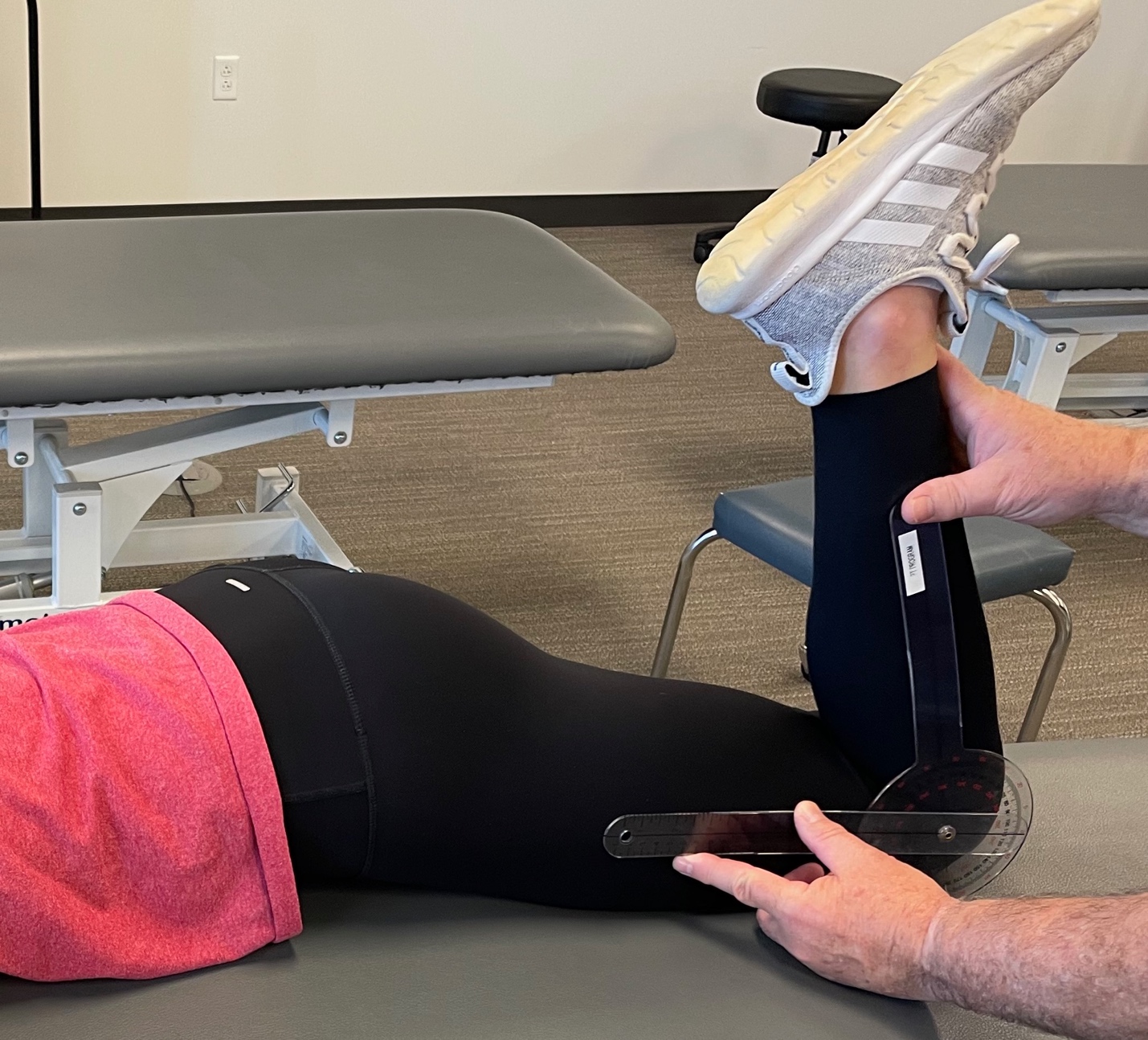
Rectus femoris muscle length (in the new measurement being studied) was measured using a new test, called the Falcon test, with the participants lying prone on a treatment table with the leg to be measured on the table while the other leg was placed off the side of the treatment table into a position of 90° of hip flexion with the foot placed on the ground (Figure 1) and the participant was told to maintain this position throughout the measuring process. One therapist measured the length of rectus femoris muscle by slowly passively bending the knee until a firm end-feel was first perceived. Another therapist, on the opposite side, measured the angle of passive knee flexion using a standard 12-inch plastic goniometer. (Figure 2) This process was completed three times, and the measurements were recorded by the measuring therapist. The mean of the three measurements were then used in statistical analysis.


After approximately five minutes of rest time, the process was repeated using the same methods and measurements were taken by another rater. The second-rater therapist was blinded to all of the goniometric recordings made by the first rater.
DATA ANALYSIS
Data analysis was performed using R, a Language and environment for statistical computing.32 Descriptive statistics, including means, standard deviations, skewness, and kurtosis of age, BMI, LEFS29 scores, and NPRS scores (now, best, and worst pain score), were calculated using R.32 Intraclass Correlation Coefficients (ICC) were calculated for inter- and intra-rater reliability of assessing rectus femoris length with the Falcon test using R32 for the entire sample (those with and without anterior knee pain) and also for just the sample with anterior knee pain. A shortened rectus femoris was examined to determine if this was related to those with anterior knee pain using the student’s t-test and also calculated the SEM and Minimal Detectable Change (MDC) using MDC = 2 * 1.41 * SEM for rectus femoris muscle length using the reliability data.25
Results
Age, height, and weight of participants are described in Table 1.
The mean amount of maximum knee flexion (e.g., rectus femoris muscle length) for the Falcon test was 134° (Table 2); knee flexion motion ranged between 100 to 158°.
Observer agreement of assessing rectus femoris length for the full sample (N=53) using the Falcon test to assess rectus femoris length showed “almost perfect” reliability for both intra and inter-rater testing: intra-rater reliability ICC = .99, [CI95: .98-.99] and inter-rater reliability; inter ICC = .96, [CI95: .92- .98].
Observer agreement for the sub-sample of only those with anterior knee pain (N=16) showed “almost perfect” reliability for intra-rater reliability (ICC 1,1 = .98); [CI95: 0.94-.99] and for inter-rater reliability (ICC 2,1 = 0.88); [CI95: 0.70 -.95]. The SEM = 1.3°; MDC=3.6°.
There was no statistically significant difference between measurements in those without and with anterior knee pain (t= 0.82, p = 0.41); [CI95: -7.8 -3.33].
DISCUSSION
Observer agreement using this new prone position rectus femoris length test named the Falcon test was found to be “almost perfect” with ICC’s above .95 for both inter- and intra-tester reliability. This method may improve upon the Modified Thomas test because with this position, having one leg off the treatment table, effectively stabilizes the pelvis without extra stabilization methods. Thus, unlike the Modified Thomas test, the therapist does not have to be concerned about maintaining the contralateral hip in full flexion to keep the lumbar spine flat on the treatment table. Also, this test position was much easier to assume, maintain, and get up from for all of the participants in this study. From experience using this test, this is also true for the patients with low back pain and hip pain, who often have considerable difficulty and pain trying to assume the Thomas test position.
The commonly used Modified Thomas test is not always easily performed. As many therapists know from experience, the sequencing of the many tasks involved with setting up a patient for the Modified Thomas Test can be difficult and often limit the ability of obtaining an accurate measurement of rectus femoris muscle length. For example, when flexing the ipsilateral knee, it is often difficult to prevent the contralateral hip from coming out of its fully flexed, knee to chest, position because of shortened hip flexor muscles. While trying to maintain the position of both hips and the ipsilateral knee, therapist then must measure the degree of knee flexion, while at the same time trying to maintain both hips positioning above the treatment table. Thus, in the clinic, for an accurate goniometric reading this test usually requires two therapists, one to stabilize and control unwanted pelvis or hip motion and the other to measure knee range of motion. Added to that, if the patient has more than a mild amount of pain, this can be very difficult for patients to assume as well as hold this position long enough to be measured. In a busy clinic this test is often difficult to accomplish.
This new test position is termed the Falcon test owing to its somewhat “bird” like pose of the patient when assuming this position, which needed a simple name so that therapist can easily describe to other colleagues the test position they used when assessing rectus femoris muscle length, rather than just calling the test the “prone, contralateral hip flexion to 90°, Ely’s test for rectus femoris muscle length”. The Falcon test may prove to be a better test than the Thomas test and Ely’s test because the pelvis can be stabilized better by flexing the contralateral hip to 90° and having the participant place their foot on the floor for stabilization. Placing the hip in full flexion, stabilizes the pelvis, preventing an unwanted increase in lumbar lordosis as well as any pelvic tilting, thus resulting in more reliable rectus femoris muscle length measurements. Thus, the Falcon test is just a Modified Thomas test turned “upside down”.
Using an Ely’s test to assess rectus femoris muscle length in some patients may be adequate for assessing rectus femoris muscle length. However, a common problem encountered with the Ely’s test is that when flexing the knee is that an end feel may not be achieved because range is limited by the heel contacting the buttock, creating a “ceiling effect”. This problem is found more often in females and in those with generalized hypermobility. A study by Sweeney et al. found that only six out of 67 female gymnast had rectus femoris limitation where they were not able to touch their heel to their buttocks with Ely’s test.33 Thus, although rectus femoris muscle length would not be considered short, the tests cannot distinguish if a muscle length difference may exist between the left and right sides. Side to side differences in rectus femoris muscle length do occur in patients, including patients after total knee arthroplasty, those with osteoarthritis of the patella and knee, patients with low back pain, and in athletes who sustain a rectus femoris muscle strain or injury. The Falcon tests allows a quick, easy assessment of rectus femoris muscle length in those with hypermobility, and after surgery or injury.
When comparing those with anterior knee pain to those without anterior knee pain there was not a significant difference in rectus femoris length between groups. However, this study was underpowered, likely by of those with anterior knee pain. Also, only one person in the group with anterior knee pain currently had considerable knee pain (6/10 NPRS) and the mean for the “worst pain” for the anterior knee pain group was only 2/10 on a NPRS while the mean current pain was 1/10. Thus, this sample may not have been representative of most who have anterior knee pain. Witvrouw et al. in a study of 430 athletes, showed that athletes with anterior knee pain had reduced rectus femoris muscle length when compared to those without anterior knee pain (124.6 versus 132.2 degrees).9 The inclusion criteria in the current study only included those with a 5/10 anterior knee pain or lower. Because the aim of the current study was to determine the intra and inter-tester reliability of the Falcon Test, patients with reported knee pain above 5/10 were not included to ensure that knee pain did not interfere with achieving an end range on the test, indicating a false positive for short rectus femoris muscle length.
LIMITATIONS
Although there were 53 participants in this study, most of the participants were female (N=39), also the average population age was younger (mean age = 22.7 years). Only 16 of the participants reported a history of anterior knee pain and of those most had only minor anterior knee pain (1/10). A limitation of the Falcon test as studied herein is that two therapists were used to assess rectus femoris muscle length, one to assess muscle end feel and maintain end range knee flexion, the other to measure the degree of knee flexion. Extreme care was taken to make sure that the second therapist did not observe the other therapist when measuring knee flexion. In hindsight, using a bubble goniometer or an electric goniometer would have eliminated the need for two therapists to measure rectus femoris muscle length. However, the position, not the measuring device, was the main focus in this study. A minor limitation to the Falcon test is that larger or pregnant patients may have difficulty lying prone.
CONCLUSIONS
A new test, named the Falcon test, showed “almost perfect” reliability for both intra and inter-rater agreement, indicating that this test can be used repeatably in clinical practice. The MDC for the Falcon test was found to be 3.6 degrees. No difference in rectus femoris muscle length measurements were found between those with anterior knee pain and those without anterior knee pain, however, the sample size was small.
Conflicts of interest
The authors report no conflicts of interests.