INTRODUCTION
ACL injuries are one of the most troublesome and debilitating injuries in professional soccer often resulting in career threatening consequences. In European professional soccer an ACL injury occurs at a rate of 0.066 per 1000 hours of training or match play.1,2 This equates to 0.4 ACL injuries per team per season which means there will be on average one per team every two seasons.1 The average length of time a player is side-lined is 241 (± 63) days highlighting the severity of this injury.3 Only 55% of athletes post ACL surgery to return competitive sport4 and in soccer following ACL surgery only 65% of players were still be competing at the same level three years post-surgery.1 In professional soccer ACL reinjury rates are also high at 17.8%3 with pressure to return players back into competition as quickly as possible.5 Webster et al,6 have reported this may be because of practitioners continuing to use time-based criteria instead of criteria-based outcomes as only 23% of athletes have completed objective functional criteria prior to return to sport (RTS). van Melick et al.7 has recommended the use of strength tests, hops tests, and on-field sports specific assessments during ACL rehabilitation before a RTS is permitted. Further work by Kyritsis et al,8 highlighted athletes were at four times greater risk of sustaining an ACL graft rupture when they fail to meet six well defined criteria (IKD testing at 60, 180 and 300°/s, single leg (SL) hop, SL triple hop, SL crossover hop, and on-field sports-specific assessments) than those who have passed RTS criteria.
The first phases of a RTS program include the diagnosis and planning Phase, the acute management and contralateral limb loading Phase and finally the Phase for restoration of normal movement and early loading. Following these three phases is the gym Phase 4. Gym Phase 4 starts the rehabilitation process of the forementioned injury specific criteria including strength,9,10 capacity,11–13 and movement quality.14,15 In gym Phase 5 the athlete is objectively evaluated for a) capacity11–13; b) strength9,10; c) isokinetic dynamometry (IKD)16–18; d) hopping using a hop test battery19–21; e) force plate jumps22–25; and f) supine isometric hamstring RFD qualities26 to ensure a safe transition into grass Phase 1.
On entering grass Phase 1 an athlete begins to retrain their on-field sport specific criteria utilizing the ‘control-chaos continuum.’27 This starts with high control and low variability exercises as an athlete completes simple ball exercises and low intensity running (<65% maximum speed) to regain confidence and aerobic fitness. Further power qualities are also evaluated in grass Phase 1 (SL triple hop,19–21 SL medial hop19,21 and SL countermovement jump)22–24 to ensure that a >90% limb symmetry index (LSI) and pre-injury scores had been achieved. In grass Phase 2, running speeds (<85% maximum speed) and the intensity of sports specific actions are increased as controlled chaos and multidirectional actions were used. Underpinning grass Phase 2 was also the restoration of all explosive qualities (SL drop jump,25 IKD peak torque at 0.18ms28 and supine isometric hamstring RFD at 100ms)26 to ensure a >90% LSI and pre-injury scores had been achieved before entering grass Phase 3. Grass Phase 3 consists of high chaos and high variability through positional specific exercises where a maximum speed and intensity was employed. Exposing an athlete to exercises of a similar physical, technical and cognitive demand to team training was the aim which provided the necessary base for grass Phase 4. During grass Phase 4 the athlete is reintroduced to team training and return to match play. The purpose of this case report was to outline a RTP for a professional soccer player who successfully restored specific injury criteria (strength, capacity and movement quality), physical capabilities (plyometric and explosive qualities). and on-field sport specific criteria utilizing the ‘control-chaos continuum.’
The Rehabilitation to Performance Pathway
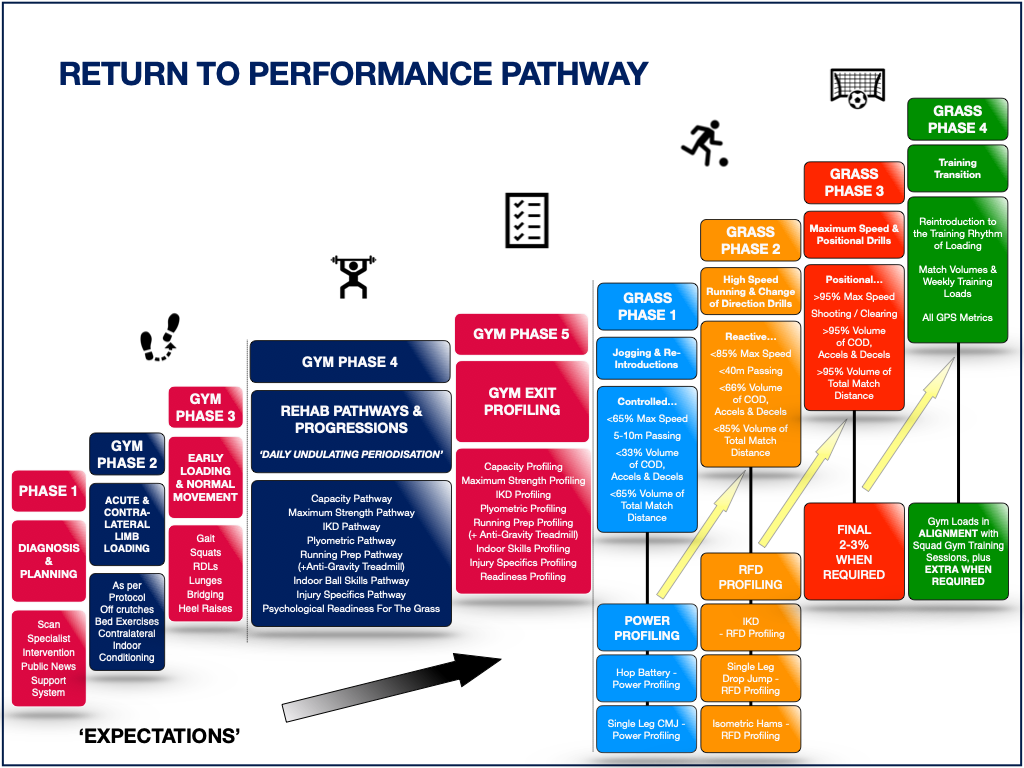
The RTP pathway (Figure 1) provides a clear plan and a progressive pathway for injured players, members of the multidisciplinary team (MDT) and coaches to follow. The philosophy has nine distinct Phases: 1-5 are predominately gym based, Phases 6-8 blend grass and gym rehabilitation, and Phase 9 is the training transition Phase. The injured player and members of the MDT go through the pathway in a step-by-step manner to provide a safe and successful RTP after injury.

In Phase 1 the initial injury has taken place. Examinations, scans and consultations are provided as required. An accurate and early diagnosis is fundamental, and the RTP plan is clearly communicated to the player. In gym Phase 2 the injured player starts acute management and can continue contralateral limb exercising when able. Treatment is given daily as the acuteness of the injury subsides. In gym Phase 3 (Figure 1) the injured player regains normal movement patterns through gait retraining and starts to initiate early injury loading with basic exercises such as double leg (DL) squats, lunges, bridge patterns and also heel raises exercises for the calf complex. Achieving fundamental exercise patterns without the injury reacting which is determined by an increase in pain levels (increase greater than >1 on a numerical rating scale)29 and effusion levels (an increase measured using the stroke test grading system)30,31 is paramount to start the rehabilitation pathways in gym Phase 4. Appropriate pacing and honest communication during the first three phases help to manage and synchronize expectations of the player, coaches, and members of the MDT.
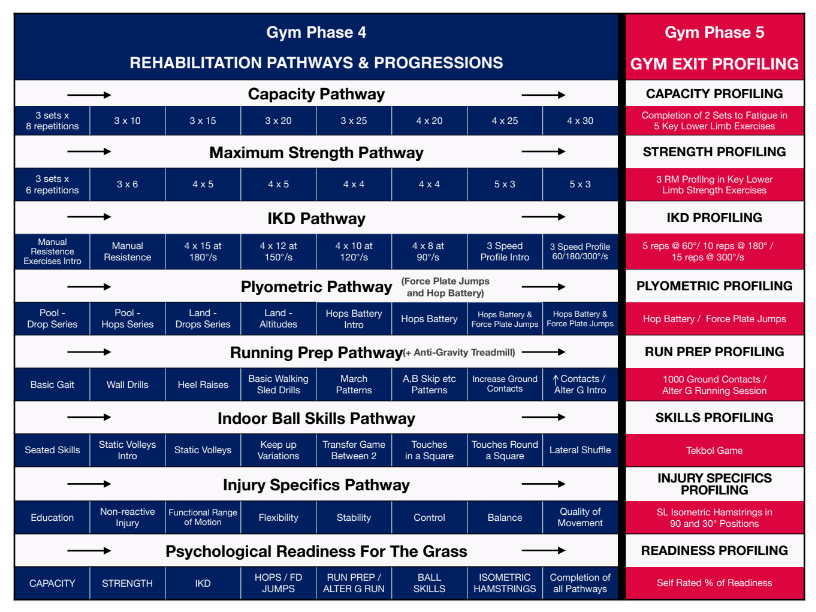
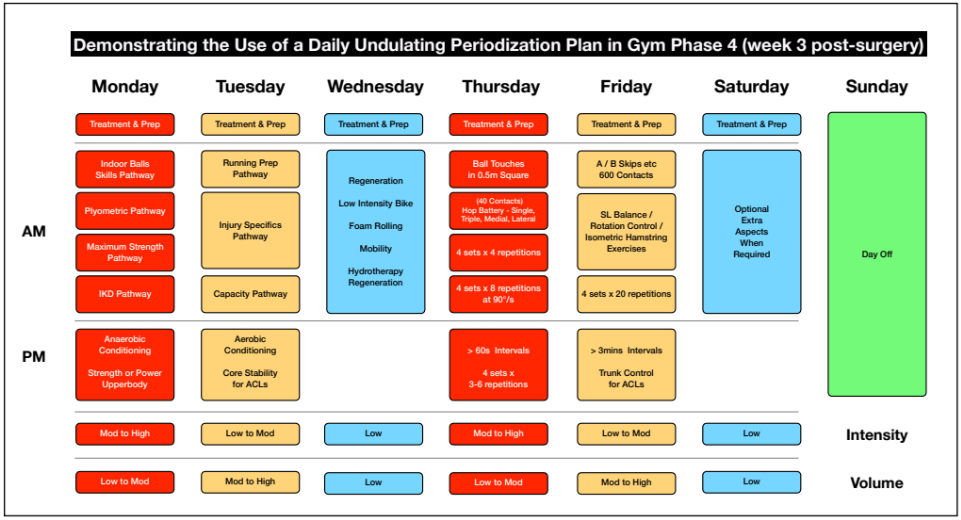
Gym Phase 4 is a key phase of the process when the player and injured structures start to recondition through the eight rehabilitation pathways and the step-by-step progressions (Figure 2). These rehabilitations pathways are programmed utilizing a daily undulating periodization (DUP) method as this allows for daily variations in intensity and volume32,33 (Figure 3).

The pathways all work on the theme of graded exposure and by varying the rehabilitation stimuli daily it is more conducive to neuromuscular adaptations than concurrent training.34,35 Each of the rehabilitation pathways targets a different physical quality and by alternating these through DUP superior adaptations can be achieved (Figure 3).32,33 Developing each of these eight rehabilitation pathways in gym Phase 4 provides three distinct advantages to the injured player: progressive exposure and adaptation of the tissue, variability through the eight distinct pathways, and confidence and trust in the injury.

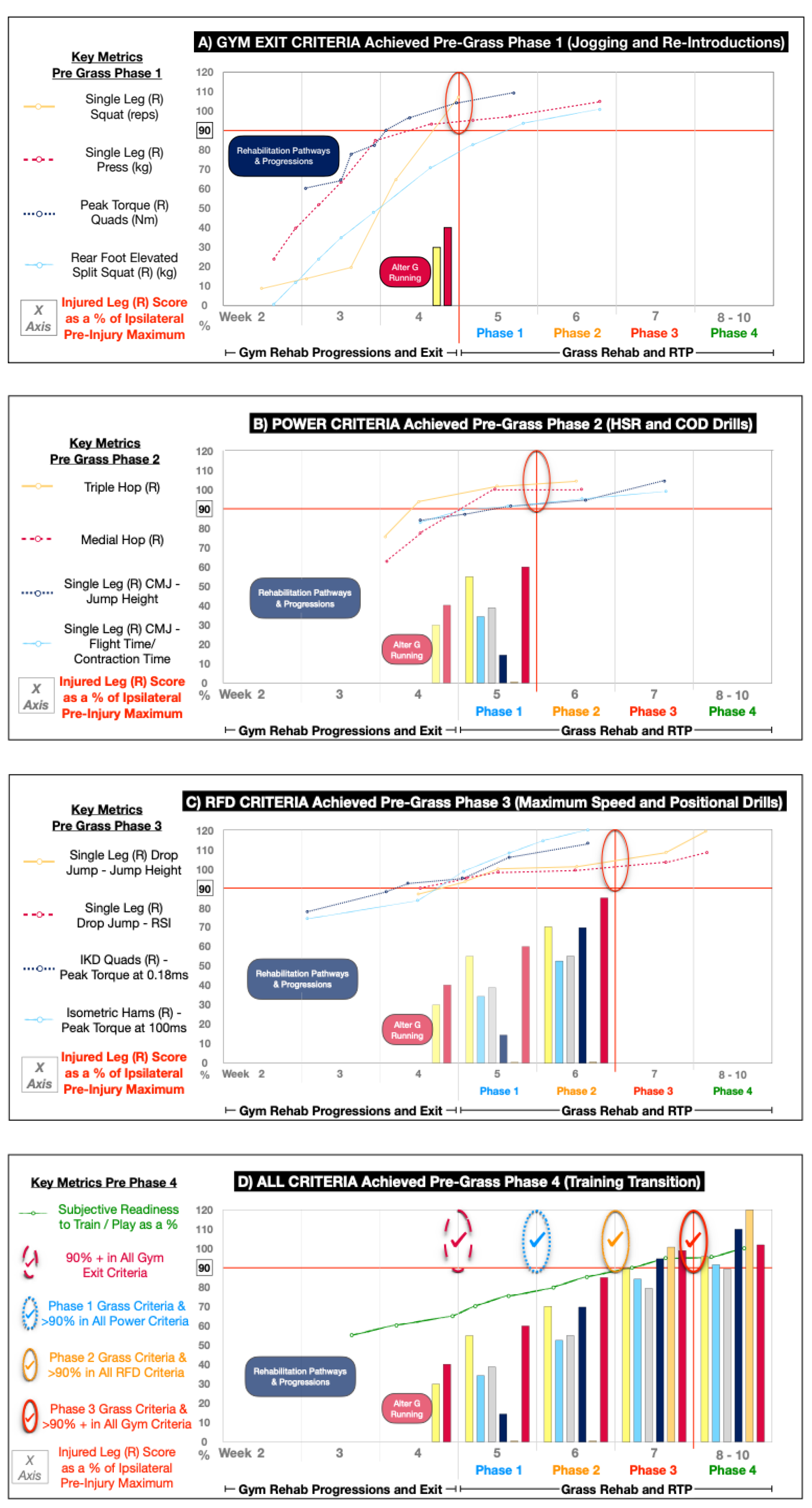
The rehabilitation theme of DUP is continued in gym Phase 5 which consists of the gym exit profiling where five of the rehabilitation pathways are objectively profiled (Figure 2). The plyometric pathway (hop battery and force plate [dual force plate system at 1000Hz, PASPORT force plate, model number: PS 2141; Pasco Roseville, CA, USA and integrated force plate form customized software package, NMP ForceDecks.] jump profiling) and injury specifics pathway (SL supine isometric hamstring RFD qualities) are practiced, and data is observed but are more formally assessed utilizing the force plates during the grass rehabilitation phases. The injury specifics pathway is used to address any outlying metrics that are not covered in the other pathways and deemed to be relevant for that specific injury or player. In this case, the measurement of the players SL supine isometric hamstring RFD qualities due to this being an ACL with a hamstring graft were considered important to assess.10,36 The five pathways are rarely completed all in one day as they stress different physical qualities such as strength (maximum strength profiling9,10 and IKD, [BIODEX, Biodex system 3, Biodex Medical System Corp., NY, USA.] profiling) endurance (capacity profiling) and movement quality (running preparation profiling and indoor ball skills profiling). Despite the development from the outset of plyometric and explosive qualities in gym Phase 4 the completion of the power hop battery,19–21 countermovement jump profiling22–24 and RFD (SL drop jump,25 IKD quadriceps peak torque at 0.18ms28 and isometric hamstring RFD at 100ms)26 profiling occur in a sequential fashion later in the pathway. Plyometric profiling being completed during the grass Phase 1 (Figure 5B) and explosive qualities like RFD profiling during grass Phase 2 (Figure 5C).
For a player to start the grass Phase 1 it is paramount to have adequately fulfilled the running preparation pathway and achieved >90% LSI and pre-injury scores on the non-negotiable prerequisites in gym Phase 5 (Figure 4A). These specifically involve the capacity profiling (SL squat,11 calf raise gastrocnemius bias and soleus bias,12 hamstring bridge in 90° and 30°),13 the maximum strength profiling (SL leg press, rear foot elevated split squat, [RFESS] trapbar deadlift and barbell floor thrust)9,10 and IKD profiling (quadriceps and hamstrings concentric tests) involving five reps at 60°/s and 15 reps at 300°/s.37–39
After successfully exiting gym Phase 5 the player starts grass Phase 1, “jogging and reintroductions”. During this phase the player is gradually exposed to their individualized match day total distances, typically running at speeds <65% of their maximum speed. It is a first step with high control and low variability as it aims to reintroduce the player to low intensity ball drills and regain aerobic fitness through 100m pitch runs27 and Hoff dribble circuits.40 Despite grass Phase 1 having an outdoor theme there are still necessary indoor gym parameters that need to be achieved to progress: >90% LSI and pre-injury scores in their power profiling (SL triple hop,19–21 SL medial hop,19,21 SL countermovement jump height and flight time:contraction time) (Figure 5B).22–24
During grass Phase 2, high speed running (HSR) and change of direction drills (COD) are developed with a gym focus on RFD. All grass intensities are below 85% of their maximum (speed and volume parameters) while the final RFD characteristics are achieved in the gym. During grass Phase 2 achieving >90% LSI and pre-injury scores in their RFD profiling (SL drop jump height and reactive strength index [RSI],25 IKD quadriceps peak torque at 0.18ms28 and isometric hamstrings RFD at 100ms)26 along with their grass metrics is the prerequisite to progress. In grass Phase 3 the player is exposed to their maximum speeds, intensities, and specific positional demands as the exercises are chaotic and highly variable.27 Intensities above 85% place an exponential load on the tissues39 and it is vital all strength, power and RFD profiling has been completed to >90% LSI and pre-injury scores to ensure safety before they enter the grass Phase 3 (Figure 5C).
Throughout grass Phase 3 the player completes positional drills and achieves maximum speeds in preparation for grass Phase 4 where they will transition into team training and match play. It should not be forgotten that despite gym metrics been achieved regularly exposing the player to the appropriate strength, power and RFD stimuli may reduce their risk of reinjury and improve their athletic performance. Once in grass Phase 4 the player trains in a normal pattern with the rest of the team as they increase their match exposure in a pragmatic fashion depending on their length of injury.
CASE PRESENTATION
A 26-year-old male professional soccer player with no previous history of injuries sustained a traumatic right knee injury. The player had a history of having played 300 professional matches as a midfielder / forward. He was a predominately right footed player and had an average playing mass of 78kg and height of 176cms.
Mid-way through the first half of a competitive match he received shoulder contact from an opposing player during a deceleration action. This contributed to a change in the following two to three steps of his normal deceleration pattern forcing his right knee into the classic dynamic valgus position of abduction, flexion, and internal rotation.41 The knee was in the ‘position of no return’ leading to an instant rupture of the ACL.42,43
After being removed from the field of play the initial examination showed reduced range of knee flexion 80° and an unwillingness to actively or passive extend the knee into hyperextension. The ACL was absent on Lachman testing and the player was experiencing high levels of pain 7-8/10 on a numerical rating scale.29 Within 48 hours a magnetic resonance imaging scan (MRI) was performed which confirmed a full thickness rupture of the ACL and partial thickness tears of the posterior horn to the medial and lateral menisci. The PCL and collateral ligaments were intact and there was no chondral damage.
Within seven days the player was assessed by an orthopaedic surgeon and the decision was made to have a surgical intervention. The plan was clearly outlined to the player: it would take a minimum of nine months to return to competitive sport and there was a 30-40% chance the medial meniscus repair might fail and require a further surgical intervention at some stage.44,45 The surgical opinion was that initially repairing the medial meniscus would reduce the tension on the harvested ACL graft in the early phases of the rehabilitation process.46–48 The player underwent a successful 90-minute operation during which the surgeon harvested a four-strand autologous hamstring semitendinosus and gracilis graft from the contralateral limb (left leg).49 This was inserted into the right knee as the new ACL. The player underwent meniscal repair of the posterior horn sections of both the medial and lateral menisci.
The player initially completed eight months of ACL rehabilitation. In accordance with Buckthorpe and Della Villa´s work14 this consisted of three distinct stages of ACL rehabilitation. Stage 1 was the early stage (Figure 1, gym Phases 2 and 3) where focus was placed on the player reducing pain and swelling and recovering normal gait and activities of daily living. Following this, the player went into the mid-stage (Figure 1, gym Phases 4 and 5) to regain muscular strength, power, and movement quality before entering the final sports specific stage to redevelop the underling explosive qualities and necessary soccer qualities to perform with the team.7,8,10,27 At the eight-month stage (Figure 1, grass Phase 2) despite the player completing HSR and COD drills on the grass the player felt a sharp pain in the medial aspect of the right knee during some routine hopping exercises. An MRI revealed he had re-torn the surgically repaired posterior horn of the medial meniscus. This distinct possibility had been outlined from day 1 so despite initial disappointment and frustration it was not a shock to the player or his support team. The player underwent the necessary medial meniscectomy of the posterior horn, and the following outlines the 10-week rehabilitation the athlete engaged in after the meniscectomy, in order to return to competitive soccer.
INTERVENTION
Gym Phases 1, 2 and 3 – ‘Expectations’
The aim of the first 3 phases (Figure 1) were to set the expectations and prepare the player for the loading and progressive gym Phase 4. Holistic care begins in all injuries during Phase 1 (diagnosis and planning). In this case the player underwent the necessary scans, consultations, and a surgical intervention to the posterior horn of the medial meniscus of his right knee. A routine surgical operation excised the small section of the posterior horn that was loose and simultaneously allowed for an arthroscopic examination of the previously reconstructed ACL and the lateral meniscus that were both reported to be healing well. Absolute clarity in communication between all members of the MDT during Phase 1 was paramount. The player and his support team inside and outside of the club along with the coaches were given clear understandable information about what had happened and the process ahead. Addressing and agreeing on the expectations of all the key people helps to start the process in a realistic and unison manner.
The acute and contralateral limb loading Phase (Figure 1 - Phase 2) lasted for the first seven days post-surgery. Wound management was prioritized along with daily use of the game ready (Model GRPro 2.1, Betchworth House 57-65 Station Road Redhill. RH1 1DL. UK.) to reduce post-surgical swelling and pain. Effleurage massage and range of motion exercises were used to restore mobility especially into knee flexion and extension and to reduce the formation of a capsular contraction.50,51 Controlled non-weight bearing exercises and the Compex muscle stimulator (electrical muscular stimulation was performed with model No SP 8.0, MI-scan, wireless, 120 mA, 400 us, 150 Hz. Guildford, Surrey, GU2 8XG, UK.) were used to address muscular atrophy and regain normal muscular recruitment patterns.52 Also in this Phase, contralateral limb exercise training53 and cardiovascular conditioning (seated battle ropes, boxing, upper body circuits, core and arm bike) sessions were completed to complement the nutritional advice given (provided by team nutritionist) and to maintain team involvement for the player wherever possible.54
This player exited gym Phase 2 at seven days post-surgery. For this, he exhibited full knee extension, flexion of >125°, the grading of a trace of joint effusion measured by the stroke test (Scale - Zero = No wave produced on downstroke. Trace = Small wave on medial side with downstroke. 1+ = Larger bulge on medial side with downstroke. 2+ = Effusion spontaneously returns to medial side after upstroke [no downstroke necessary]. 3+ = So much fluid that it is not possible to move the effusion out of the medial aspect of the knee)30,31 and a pain level never above 2/10 on a numerical rating scale.29–31 He had strictly adhered to the prescribed protocol, was competent in his non-weight bearing exercises and had subsiding pain and swelling levels. Patience within and respect during these first two phases allowed the player to appropriately start the gym Phase 3.
With a low pain score (<2/10 numerical rating scale) and trace joint effusion the player progressed into the gym Phase 3 to start early loading and regain normal movement patterns (Figure 1). Competency in the fundamental weight bearing exercises and gait variations was the primary goal of this phase. Firstly, he completed the key exercises like squats, lunge patterns, Roman deadlifts (RDL), heel raises, and gait exercises with reduced body weight in the pool and was then transitioned to the gym. Movement quality was deemed to be a key factor and assessed visually to ensure there was no loss of balance, contralateral hip drop, ipsilateral knee valgus or any excessive trunk movement.55,56 During gym Phase 3 the player was required to complete 3 sets x 8 repetitions with normal movement strategies and no post-session reaction to be able to start gym Phase 4. By day 10 the player had achieved these criteria and could start the rehabilitation pathways outlined in gym Phase 4 (Figure 2). Experience suggests premature entry into gym Phase 4 will lead to recurrent episodes of swelling, pain and compensatory movement strategies55,56 that reduce the players well-being and overall confidence.
Gym Phase 4 - Rehabilitation Pathways and Progressions
This phase started at the 10-day mark post-surgery and continued into week four when the player started to complete the necessary gym exit profiling tests in gym Phase 5. The aim of gym Phase 4 was to expose the injured lower extremity to different physical demands through the variety of rehabilitation pathways outlined in Figure 2. The pathways are clearly outlined in a progressive manner as the demands increase in a step-by-step fashion ensuring the player and the injury can safely perform the profiling tests in gym Phase 5.
During gym Phase 4 not all the rehabilitation pathways were worked on each day as a DUP theme was applied throughout the week (Figure 3). For this player a normal working week consisted of rehabilitation days on Monday and Tuesday with Wednesday set as regeneration day. Similarly, Thursday and Friday were rehabilitation days and often Saturday was free to work on any specific aspects as required. Sunday was traditionally set as a day off which was aligned with normal team training schedules. The aim of the undulated process was to expose the player to the most complex and neuromuscular challenging demands at the start of the session and the safer exercises towards the end of the session when arguably he was more fatigued.
Similarly, the player completed more neuromuscular challenging pathways (indoor ball skills pathways, plyometric pathway, maximum strength pathway, IKD pathways and anaerobic and upper body type conditioning) on Monday and Thursdays when the player was most fresh compared to lower intensity and higher volume type sessions on Tuesday and Fridays (running preparation pathway, injury specifics pathways, capacity pathway, aerobic conditioning and core exercises) when the player had worked the previous day (Figure 3).
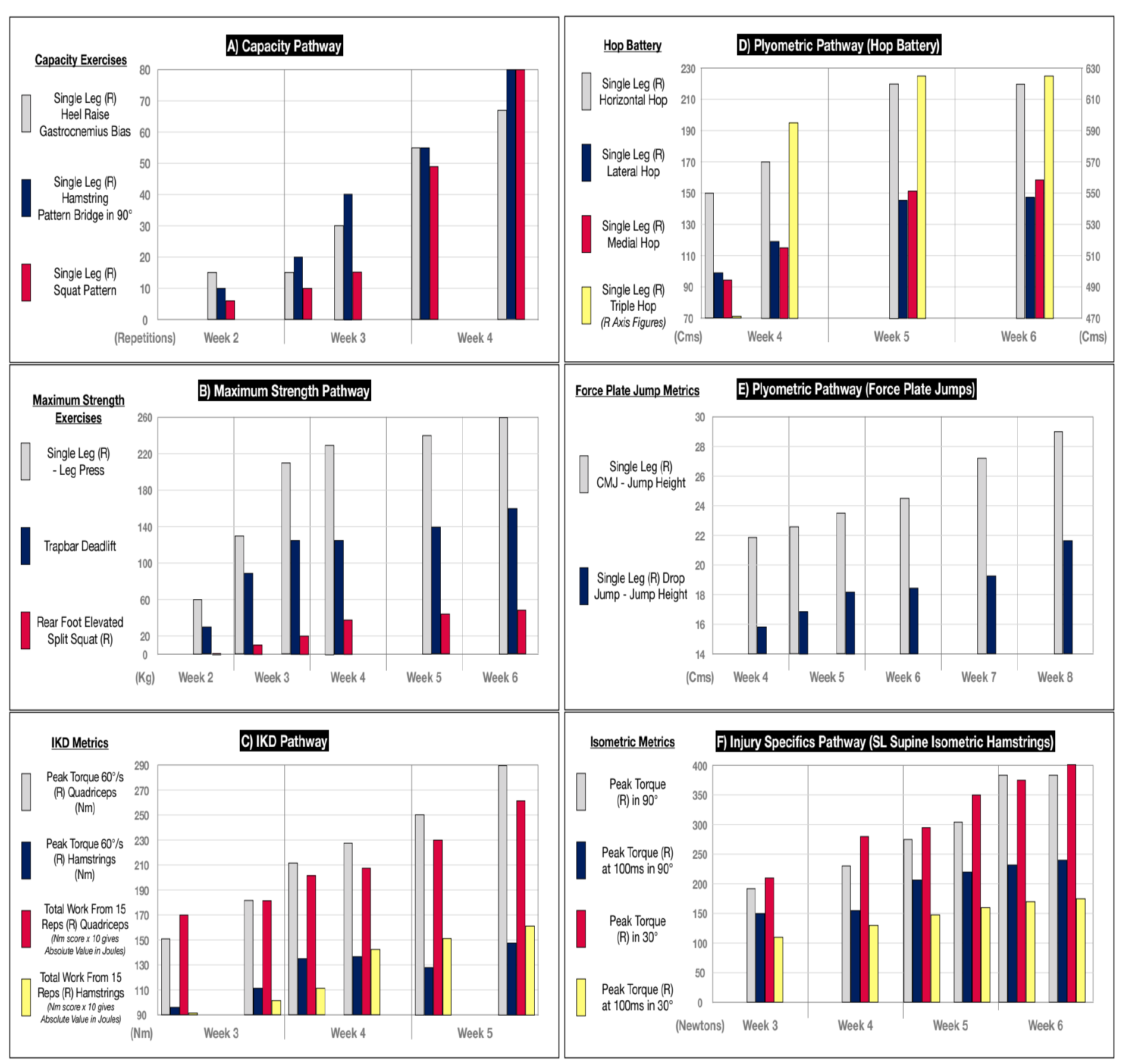
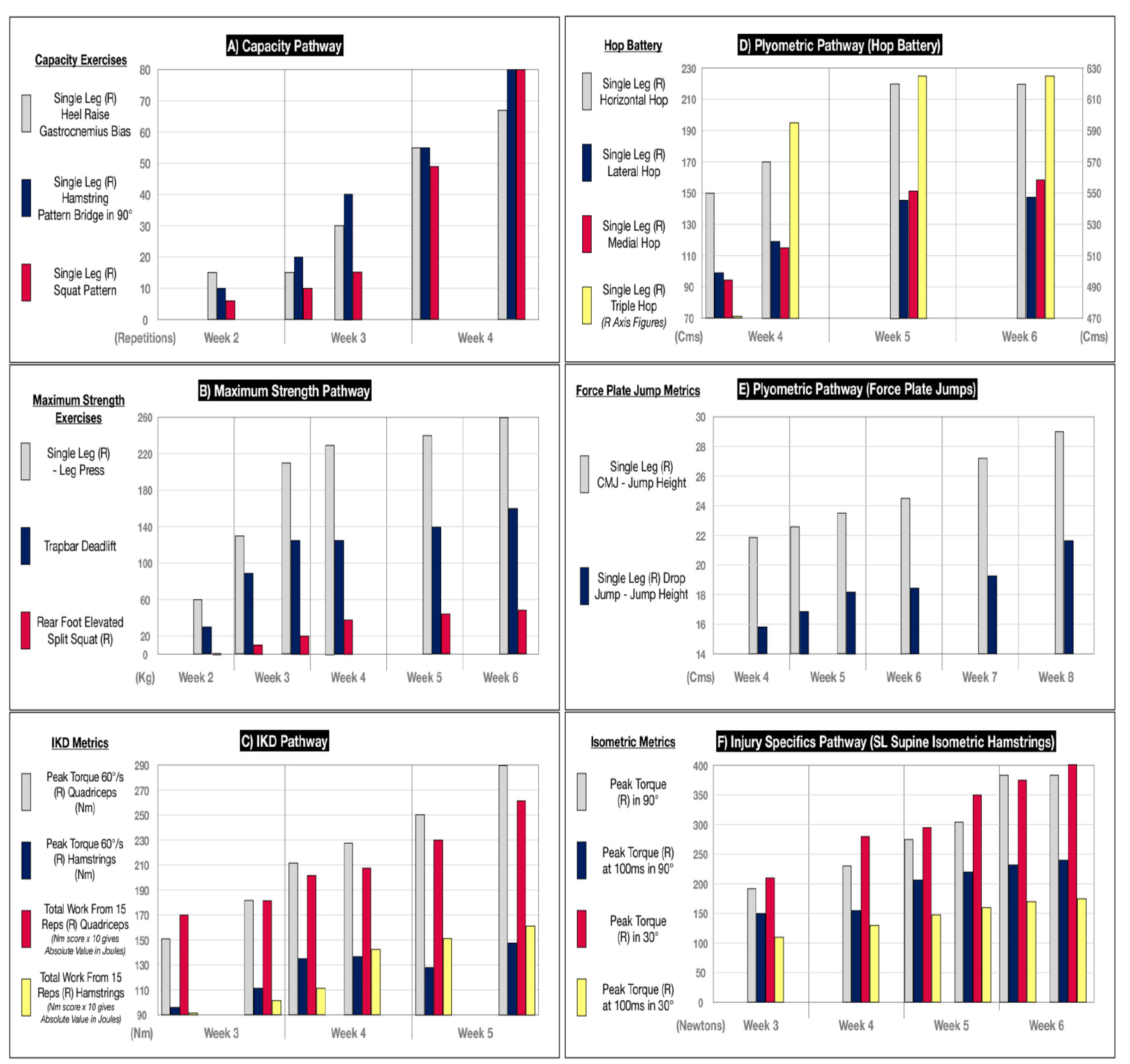
During gym Phase 4 there were eight key rehabilitation pathways to follow. The manner in which six of these progressed is highlighted in Figure 4. In the capacity pathway the player completed multiple exercises in his regular sessions but was critically assessed in five key SL exercises (squat,11 calf raise gastrocnemius bias and soleus bias12 and hamstring bridge in 90° and 30°).13 These are progressed from 3 sets of 8 repetitions to 2 sets to fatigue which was completed in the gym exit profiling in gym Phase 5. Gradually increasing the repetitions and sets developed a local muscular endurance and robustness in the joint to withstand the loads in preparation for the grass phases ahead.
Strength was addressed in the maximum strength and IKD pathways. With all strength progressions the repetitions were reduced as the load was increased. Again, the player had a variety of exercises for the posterior and anterior chain but was critically assessed in the SL leg press, RFESS, trapbar deadlift, and the barbell floor thrust.9,10 Accompanying this the IKD pathway was initiated on the treatment table with manual resistance as the therapist resisted knee flexion and extension through range. This was then progressed to the IKD machine where initially quicker speeds (low joint forces) were employed.57 These contraction speeds were gradually decreased from 180°/s to 60°/s as the player ended by completing the traditional 3-speed profiling (60,180 300°/s)16–18 at the end of gym Phase 4 ready for the gym exit profiling in gym Phase 5.
The players power and RFD qualities were also introduced early in gym Phase 4. They were initially started through the introduction of the plyometric pathway which involved the player completing a drop series of squats and lunges in the pool on Mondays and Thursdays (Figure 3). This was progressed to the land with simple landings from a step and box (altitude landings).58 As the plyometric pathway progressed the introduction of the hop battery which consisted of the SL horizontal hop, triple hop, medial and lateral hop for distance tests as described by Ebert et al,19 and force plate jump profiling which consisted of DL and SL countermovement jump, along with DL and SL drop jumps23,25 leading into week four which included some of the types of simple hopping techniques the player was doing. The use of the force plates enabled the analysis of the relative force, RFD and interlimb asymmetries for example, to be compared to preinjury standards.10,22,23,36 Despite ongoing improvement and monitoring these qualities cannot be completely restored without the necessary grass speed exposures later in the process.
Movement patterns through the running preparation pathway were also completed specifically on Tuesday and Fridays (Figure 3.) as the number of ground contacts increased from 100 in the first session to 600 by the end of gym Phase 4. Every time the foot hit the ground it was counted and calculated as a sum for the total session. This progressed from simple wall drills and sled walks to A skip (a skipping pattern in a linear direction emphasizing the hip drive phase of running) variations. By week 4 the player had increased the number of ground contacts so he was able to start gym Phase 5 where he would be expected to complete 800-1000 ground contacts in a session. This along with two running introduction sessions (60-75% progressing to 95% body weight) on the anti-gravity treadmill (Alter-G, Fremont, CA, USA.) further highlighted his readiness for the grass phases.
Gym Phase 4 encompassed the rehabilitation pathways and progressions and in this case lasted from 10 days into week 4. These step-by-step increases in each of the pathways emphasized the design of graded exposure and also the variability created through the different pathways. The player improved in his local muscular endurance (capacity pathway) and strength (maximum strength and IKD pathways). He also started to develop his power and RFD qualities (plyometric pathway). By adding the movement qualities that were practiced in his running preparation pathway and indoor balls skills pathway he was starting to develop a level of confidence in the gym. This self-confidence came from being pain free not only in these but in the wide variety of exercises and movements that gym Phase 4 included. Having successfully completed the gym Phase 4 rehabilitation pathways described (Figure 2) he was ready to enter the gym Phase 5 (gym exit profiling).
Gym Phase 5 - Gym Exit Profiling
The most common question a player asks at the start of the rehabilitation process is “when I can start running on the grass?” Gym Phase 5 has been specifically designed using objective tests to answer this question. The player had complete familiarity with the profiling modalities as they were gradually introduced throughout gym Phase 4. These standardized and repeatable profiling tests such as the hop test battery19–21 and force plate jumps22–25 were conducted regularly by all squad members as monitoring tests which added weight to their significance and relevance to performance. The common language they created was understood and well interpreted between the MDT, the player`s peers, and the coaches through ongoing education.
The structure of gym Phase 5 was conducted in complete alignment with the DUP of gym Phase 4. Gym Phase 5 was fundamentally an extension of gym Phase 4 with the exercises in the pathways being objectively profiled on the fourth and fifth day of week 4. On the fourth day the player completed the indoor ball skills profiling, plyometric profiling, the maximum strength and the IKD strength profiling. Despite a seemingly large volume of work, the indoor ball skills profiling (15 mins), the plyometric profiling (15 mins), the maximum strength profiling (30 mins) and the IKD profiling (15 mins) all took in total 75 minutes. Again, familiarity during gym Phase 4 to all these exercises reduced the players time to completion in one session.
The indoor balls skills pathway had seen the player progress through familiarization exercises with the ball which included exercises like the keep-up variations to lateral shuffles and volleys. The plyometric profiling (force plate jumps included the DL and SL countermovement and drop jumps with the hop battery including SL horizontal, triple, medial and lateral hop techniques) would not be equal to preinjury levels at this stage but it was important the player could perform all tests without pain or compensatory movement patterns. Compensations were judged in real time in the frontal plane by observing a vertical line through the trunk, one line through the exercising limb and one line horizontally through the pelvis. Despite being subjective, suboptimal mechanics seen through this method are easy to assess and can be used as simple steps to coach the player to better movement quality.15,59 In summary the movement quality, overall confidence, and ability to complete the plyometric variations at this stage was a prerequisite to exit gym Phase 5.
The maximum strength profiling (Figure 4B) saw the player achieve 230kg on a 3-repetition maximum9 SL leg press and 35kg each arm during a RFESS. Later that fourth morning the player completed the IKD profiling. At this stage the key criteria to achieve were >90% LSI and pre-injury scores in the peak torque at 60°/s (strength)37,38 and the total workload for 15 repetitions at 300°/s (endurance)16,60 for the quadriceps and hamstring muscles (Figure 4C). For the strength and endurance IKD tests, the quadriceps were 96% and 94% respectively when utilizing the pre-injury ipsilateral maximum scores for comparison.
On the final workout day of the week the player started by completing the running preparation profiling. Through a variety of drills such as A skips (a skipping pattern in a linear direction emphasizing the hip drive phase of running), B skips (a skipping pattern in a linear direction emphasizing the hip extension phase of running) and heel flicks for example, the player demonstrated the ability to complete 1000 ground contacts per limb in a movement session, a prerequisite for starting grass Phase 1. He also completed his final anti-gravity treadmill running session. The treadmill session followed on from the previous session that ended while running at 75% body weight. Two-minute running intervals at 12.6 km/hour (3.3ms-1 / 40% of maximum speed) with a stepwise increase from 80 to 95% body weight was successfully achieved.10 This was in exact alignment with the planned running intervals of the upcoming first session of grass Phase 1 in the following week. Later in the final day of the week the player completed low-level control and balance exercises as injury specific exercises. Movement quality while maintaining limb, pelvic and trunk alignment15,56,59 was the focus as SL rotational and balance type exercises were conducted.
To conclude gym Phase 5 the player completed the capacity profiling. This involved the player completing as many repetitions as possible on five key exercises. Throughout gym Phase 4 he had worked on numerous variations of these exercises like in all pathways but these five were specifically chosen to be profiled. From Figure 4A, the player exceeded >90% LSI and pre-injury ipsilateral maximum scores. Scores of 67 repetitions for the SL gastrocnemius heel raise, and 80 repetitions for the hamstring bridge in 90° and the SL squat exercise were achieved (Figure 4A). These tests along with hamstring bridges in 30° and SL soleus heel raise were used to measure the capacity of the lower limb musculature.11–13 Comparisons between limbs and exceeding >90% of his pre-injury ipsilateral maximum scores provided the player with the feeling of confidence to safely enter the grass Phase 1.

To exit gym Phase 5, it was important to utilize a holistic approach. Four key factors were interpreted together to make a safe and calculated decision that the player was ready to start grass Phase 1. Firstly, he had achieved >90% of his pre-injury ipsilateral maximum scores in his capacity, maximum strength and IKD profiling (Figure 5A). These key pathways were the cornerstone of his rehabilitation at this stage. Secondly it is widely acknowledged that the power (hop test battery - Figure 4D, and countermovement jump profiling - Figure 4E) and RFD (SL drop Jump,25 IKD quadriceps peak torque at 0.18ms28 and isometric hamstring RFD at 100ms)26 qualities will lag61 at this stage, but the player had started to go through the progressions and was comfortable with all exercises of the plyometric pathway (Figure 2). Thirdly, although not purely objective, the player had completed other pathways like the running preparation and indoor ball skills (Figure 2) which further highlighted his competency in a variety of movement patterns and also to tolerate load. Finally, and arguably the most critical factor was the psychological confidence the collective of all the pathways had provided the player. At this stage expecting the player to feel ready to resume playing is unfeasible. However, verbalizing his confidence and readiness (>90% confidence) to start on the grass was imperative for him to commence grass Phase 1 at the start of week 5. This simple confidence scale (>90% confidence) was used at the end of each phase to ensure communication between the player and therapist ensuring the player felt psychologically ready to start the next phase.
Grass Phase 1 – Jogging and Reintroductions
The aim of grass Phase 1 in week five was twofold. Firstly, to reintroduce the player to ball activities and jogging on the grass whilst increasing his level of aerobic fitness27 and secondly to develop the necessary power qualities in the gym to start HSR and COD drills in grass Phase 2. In grass Phase 1 despite the player working on the grass, off-feet conditioning, and gym work continued in unison with very specific targets after the profiling completed in gym Phase 5. This player needed to accomplish the necessary power qualities assessed through the hop battery19–21 and SL countermovement jump profiling.22–24 Specifically achieving >90% LSI and pre-injury scores ipsilateral maximum scores in these key power tests was required to exit grass Phase 1 (Figure 5B).
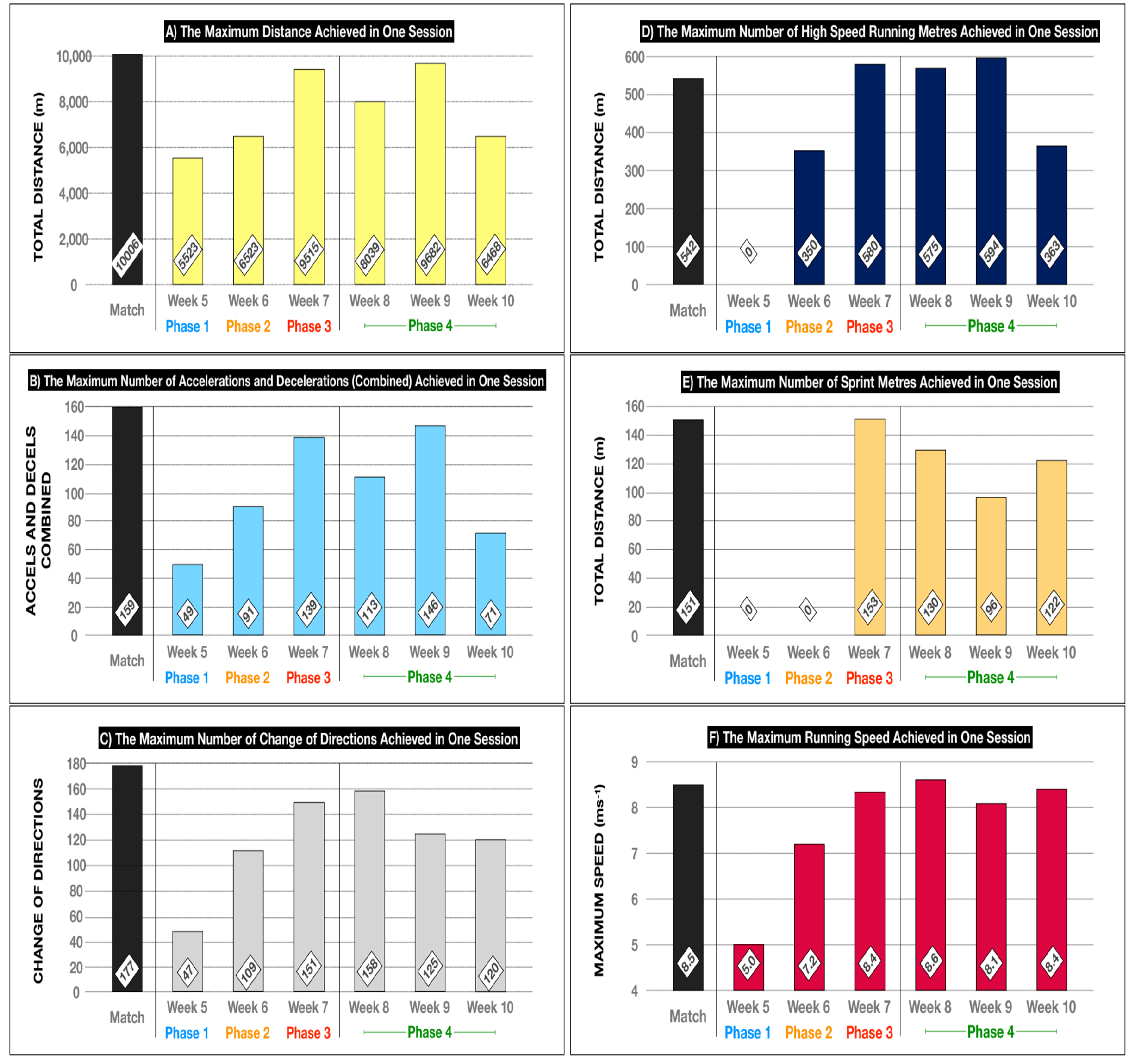
On the grass the player completed sessions that involved pitch length runs (1 pitch length 100m x 5 = 500m),10 and dribble circuits (Hoff dribble circuit 290m x 1 = 290m)40 at a low speed (<65% maximum speed <5.1 ms-1) to increase his aerobic fitness level. As the player progressed through grass Phase 1 the total distance he covered in each session improved by 1km each day to 6km from a starting point of 2km. Incrementally increasing the number of pitch runs and dribble circuits was conducting in a step by step process as this type of aerobic conditioning has proven to achieve a heart rate <85% maximum.10,62,63 Accompanying this he was reintroduced to simple passing (0-10m), ball manipulations and low-level patterning drills that were incremental advancements to the exercises he had completed during the indoor ball skills pathway. He had no exposure to HSR or high-level accelerations and decelerations (>2.5 ms-1) as the high control and low variability ball drills were confined to distances no greater than 4 meters. However, with the sensitivity of the global positioning system (GPS system - augmented 10 Hz Apex, Catapult Leeds, UK) he did record some low-level (<2.5 ms-1) COD (total in one session 47, 27% of match total volume, Figure 6C) and accelerations and decelerations (total in one session 49, 31% of match total volume, Figure 6B). All these short distance intensity type actions were controlled and included within the small area (4m maximum) patterning drills the player completed. Grass Phase 1 was conducted in week five post-surgery and contained in total of five grass sessions. Critically during Phase 1 aerobic conditioning was implemented in the form of 500m runs (1 pitch length 100m x 5) and Hoff dribble circuits.40 During this and simple passing drills the player regained some confidence in his body, had a reintroduction to ball drills and accumulated 18,800 meters at a low speed, with 5523m being the highest achieved in one session (Figure 6A).
_data_collected_in_six_key_metrics_used_to_gra.png)
To complement the running and ball work the player also prioritized power work in the gym during grass Phase 1. Crucial to this whole RTP philosophy was the blending of the grass and gym exercises both being addressed simultaneously to prepare the player for the next phase he would progress onto. At this point in grass Phase 1 he needed to complete the necessary power profiling (hop battery19–21 and SL countermovement jump testing)22–24 to ensure the player was adequately prepared and safe to start grass Phase 2. During the morning sessions specific cueing was utilized to direct the players intent in producing explosive movements. The player completed three power sessions (day 1, day 4 and day 6 in the week) which consisted of the profiling criteria and supplementary power-based exercises (squat jumps, lunge jumps, step jumps, and hurdle hop variations etc). The power profiling (part of the plyometric pathway) specifically focused on the hop test battery19–21 and the SL countermovement jump.22–24 The results of the hop test battery significantly improved with the key hops for this injury being the SL triple hop (625cms) and the SL medial hop (152cms) both exceeding >90% LSI and pre-injury ipsilateral maximum scores (102 and 101% respectively, Figure 5B). Similarly, the SL countermovement jump height (24.2 cms) and the flight time:contraction time ratio (0.58 ms-1) for this player had achieved pre-injury levels of 94 and 95% respectively (Figure 5B). To exit grass Phase 1 the player had completed the GPS criteria (5-10m passing, low intensity COD, accels and decels, aerobic runs with a maximum of 6km in one session, all metrics <65% in speed, intensity, and volume) and also the necessary power criteria (Figure 5B) which were the prerequisites to start grass Phase 2.
Grass Phase 2 – High-Speed Running and Change of Direction Drills
The aim of grass phase two was twofold. Firstly, it was on the grass to complete HSR (<85% of maximum speed), increase session volumes (<85% of match total volume in metres), complete reactive drills including CODs, accelerations and decelerations (<66% of match total volumes) and also to complete some longer kicking exercises (<40m) (Figure 1). All of these requirements were within the controlled chaos and multidirectional themes of the ´control-choas continuum´.27 The second aim was in the gym where the final RFD qualities (SL drop jump,25 IKD quadriceps peak torque at 0.18ms28 and isometric hamstring RFD at 100ms)26 were achieved again with a prerequisite to exit grass Phase 2 being set at >90% LSI and pre-injury ipsilateral maximum scores (Figure 5C).
During grass Phase 2 (week 6) the player continued the theme of DUP. On day 1 and day 4, the player completed more intensity-based drills including short distance (0-20m), accelerations, decelerations and CODs. Conversely on day 2 and day 5, he completed a more extensive HSR theme at the start of the session and an accumulation of low intensity meters towards the end of the session. Daily warmups of either rotational and more flexed positions or more upright HSR mechanics reflected these grass themes to prepare the player appropriately. Towards the end of the grass Phase 2 in the day 4 session the player had completed in total 91 accelerations and decelerations (57% of match total volume - Figure 5B) and 109 COD (62% of match total volume - Figure 5C). On day 5 the player accumulated 350m of HSR (peak speed 7.2ms-1 = 85% of maximum speed – Figure 5F) in this extensive day and a total of 6523m in his largest volume session (Figure 5A). Concurrent to the physical work was the ball work where the player completed longer passing type exercises specifically on the intensive days (day 1 and day 4).
During grass Phase 2 in addition to the HSR and reactive drills the player also prioritized RFD work in the gym. RFD was deemed to be the last quality to be completed in the gym61 and a non-negotiable prerequisite to start the maximum speed work in grass Phase 3. The development of the player´s RFD had started beginning at 10 days post-surgery as the player engaged in the plyometric pathway (Figure 2). Also, by undertaking all of the rehabilitation pathways and achieving qualities like capacity, strength (Figure 4A) and power (Figure 4B) this could finally be accomplished. By replicating the periodization of the power work in grass Phase 1 the player completed pre-grass sessions on day 1, day 4 and day 6 in the week programmed around the theme of RFD. A variety of exercises such as hamstring isometrics, drop jumps and hurdle bounds were employed to increase limb stiffness and utilize the fast stretch shortening cycle (<250ms ground contact times).59,61 Minimal repetitions (2-4) and maximum intent was employed as the player´s RFD qualities were profiled in numerous ways. As Figure 5C highlights >90% LSI and pre-injury scores was specifically required in the SL drop jump (jump height and RSI),25 the RFD of the quadriceps peak torque on the IKD at 0.18ms (at 180°/s)28 and the isometric RFD in the hamstrings (3 x 3s isometric holds) on the force plates at 100ms (Figure 4F).26 By the end of week six the player had successfully completed grass Phase 2 as he had achieved the GPS criteria (Figure 1) and the necessary RFD criteria (Figure 5C) which were the prerequisites to start grass Phase 3.
Grass Phase 3 – Maximum Speed and Positional Drills
At seven weeks post-surgery, the player started grass Phase 3. The aim of this phase was to achieve maximum GPS metrics (Figure 1) and work on any rehabilitation residuals that he had not accomplished. On the grass the phase involved maximum speed work (>95% of maximum speed), increased session volumes (>95% of match total volume in metres), positional drills including CODs, accelerations and decelerations (>95% of match total volumes) and also to complete positional kicking in this case namely shooting drills (Figure 1). The second aim of grass Phase 3 was in the gym. If there are no major asymmetry to work on like in this case, then continuing to monitor essential variables is the focus such as RFD and maximum strength qualities for example.
Grass Phase 3 was periodized in a similar theme (intensive days on day 1 and day 4 and extensive plus volume (low intensity) days on day 2 and day 5) to grass Phases 1 and 2. This was in alignment with the team’s training schedule except the hardest day of the week in RTP was on day 5 as opposed to day 6 (match days) for the team. On the extensive days (day 2 and day 5) the player achieved a speed of 8.4 ms-1 (Figure 6F), 153m sprint meters (Figure 6E) and 580m of HSR (Figure 6D) which equated to 99%, 101% and 106% of his match metrics respectively. The second part of his day 5 session included conditioning (high volume at low intensity) as he accumulated a total session distance of 9515m (95% of match total metres). Conversely intensive metrics were similarly developed as he achieved in one session 139 accelerations and decelerations (Figure 6B) and 151 subsequent COD (Figure 6C) (87% and 85% respectively of match total volumes). Chaotic and highly variable movement patterns were individualized for the player through positional drills and shooting drills.27 Similarly controlled collision exercises with the physio and peers were designed to build confidence by replicating his injury mechanism and prepare him for team training in grass Phase 4.
Despite the player achieving >90% LSI and pre-injury ipsilateral maximum scores in the maximum strength (Figure 5A) and RFD profiling (Figure 5C) the player subjectively wanted to maintain these training habits and qualities. He valued their link to performance and his preparation sessions on day 1 and day 4 continued to favor a RFD theme. Conversely after his grass sessions on the day 2 and day 6 he completed a concise maximum strength exposure (3-4 sets x 3-4 repetitions). Accompanying these positives themes the player subjectively felt 90-95% ready to train (Figure 5D) which is also another key psychological prerequisite to be achieved prior to starting with the team in grass Phase 4.
Grass Phase 4 – Training Transition
To enter grass Phase 4 at eight weeks post-surgery the player had completed the three grass phases exposing him to the necessary GPS demands (Figure 1) and also accompanying gym profiling (Figure 5D). Clinically he presented with no pain or swelling in his knee. He had experienced no major setbacks during the 8 weeks post-surgery and self-rated his readiness to train at >90%. During grass Phase 4 he rejoined full team training, exposing him to full contact and the inevitable neurocognitive overload that team training brings. The training speeds, spaces and interaction with players and coaches’ instructions undoubtedly overloaded the player, so unnecessary increases in the physical demands were not priortized.27 In the gym the player continued a bi-weekly prophylactic strength exposure in the key exercises he perceived to be benefiting his knee (RFESS, SL leg press, glut-hamstring bench raises, Nordic hamstring exercises, and the IKD, at 3 sets x 5 repetitions at 60°/s).38 His preparation sessions consisted of RFD exercises to ensure the RFD in the concentric and eccentric phases were continuing to improve. Both the strength and RFD sessions contained some of the key profiling tests (for example, strength exercises RFESS, SL leg press and IKD at 60°/s and RFD exercises such as SL drop jump and supine isometric hamstrings) now being employed as simple monitoring exercises to check for any subsequent trending patterns. The detection of any possible drop offs could be addressed early with the appropriately prescribed prophylactic strength or RFD sessions pre or post training. After two weeks of full team training the player took part in a behind closed door friendly match where he successfully played 45 mins. This was followed, five days later, with another 45 minutes in a friendly match situation. These match minutes were further increased to 75 and 90 minutes before the player played in his first full league match. Similarly, he built up his competitive match minutes from 25 to 45 to 75 as he regained match fitness.
SUMMARY
The purpose of this case report was to outline a RTP for a professional soccer player who successfully restored specific injury criteria (strength, capacity and movement quality), their physical capabilities (plyometric and explosive qualities), and the retraining of their on-field sport specific criteria utilizing the ‘control-chaos continuum.’ The player went through the nine-phase RTP pathway linking the pathology, the development of physical qualities in the gym, and also sport specific qualities on the grass. The pathway utilizes clearly outlined exit criteria for each phase and demonstrates how each of the phases were progressed by graded exposure in the gym and on the grass utilizing the ‘control-chaos continuum’. Furthermore, the provided pathway presents how the players physical qualities were developed in a sequential fashion with capacity and strength developed first followed by plyometric and explosive qualities. The RTP pathway has clear phases, and exit criteria, a philosophy that is not limited by static time-based markers but instead uses objective and performance-related criteria. By achieving a LSI of >90% and pre-injury scores it allowed the player to complete the process as quickly as possible while ensuring he was safe to return to competition.
Conflicts of Interest
The authors report no conflicts of interest.