INTRODUCTION
Preprofessional and professional dancers have a 90% lifetime incidence of developing musculoskeletal (MSK) disorders, including injuries and pain.1 Dancers will sustain an average of one to two injuries per season.2–6 Dance related MSK disorders affect dancers’ physical and mental health, sometimes even threatening their careers.7,8 Hamilton et al. have found that the most injured are the preprofessional dancers who end their career prematurely.8 MSK disorders can also have serious consequences for the school or company where the dancers train.4 A dancer’s absence will affect the training of the other dancers and put financial pressure on their company.7 MSK disorders also carry a heavy personal and societal economic burden, as 60% of injured dancers will require a costly imaging examination or referral for their psychological health.1,3 MSK disorders can occur as a result of trauma or overuse of the MSK system. Overuse injuries account for 66-79% of all MSK disorders.2,3,6,9 Among dancers, overuse injuries are often related to a repeated faulty movement pattern or an excessive mechanical load that increases over time with the progression of their career.9 This highlights the importance of identifying best practices to either prevent or treat MSK disorders.
Even though dance is considered an art form, dancers are often regarded as athletes due to the high physical demand of their practice and therefore benefit from training to prevent injury.10 Many authors have supported the idea that conservative interventions such as strengthening and conditioning programs are one way of improving the dancers’ fitness and decreasing injury risk factors.11–15
Regarding treatment, conservative modalities specific to dancers have emerged in recent years. These types of interventions include physical therapy (e.g., manual therapy, strength and conditioning programs), massage therapy as well as interventions provided by other health care professionals.
However, scientific evidence on the effects and efficacy of conservative interventions to prevent and treat MSK disorders has never been synthesized, and the level of proof for these interventions has not been reported. Considering the high level of injuries among dancers and the unique physical demands of this art form, there is an urgent need for practitioners to identify effective conservative treatments to prevent or treat MSK disorders in dancers.
The aim of this systematic review was to locate, appraise and synthesize the available information on conservative interventions currently used for treating and preventing MSK disorders and their effect on pain and function in preprofessional and professional dancers.
METHODS
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was registered on the international prospective register of systematic reviews (PROSPERO CRD42021258563).
Search strategy
The following bibliographic databases were searched from inception to August 21st, 2022: Cinahl, Medline, ERIC, Sportdiscus, Psychology and behavioral science collection. A combination of keywords associated to the population (dance, preprofessional, professional) and outcomes (pain, function, performance) were used in the search. The full search strategy is presented in Appendix 1. No language restrictions were applied to the search. Grey literature was searched on the websites of Healthy Dancer Canada and the International Association for Dance Medicine and Science. The reference lists of eligible articles found in the main search were also screened for additional articles.
Eligibility criteria
The literature review included prospective and retrospective cohort studies as well as randomized controlled trials (RCTs) investigating the effect of at least one conservative intervention on professional and preprofessional dancers. Both injured and uninjured dancers at the time of intervention were included for treatment or prevention of MSK disorders. Case series and case reports were excluded.
Studies involving preprofessional and professional dancers, including ballet, classical, contemporary, hip hop, modern, ballet jazz and/or jazz dancers were included, as long as they represented 75% or more of the sample. Gymnasts, circus artists, tumblers, cheerleaders, and dancers whose main style was not ballet, jazz or contemporary (e.g., folk, irish, spanish, native and traditional dancers) were excluded from this review. These other sports and dance styles were excluded because the physical demands are very different from ballet, jazz or contemporary dance.
Regarding treatments, studies were included if they evaluated non-invasive interventions that aimed to prevent or treat a MSK condition (exercise/stretching, physical therapy, manual therapy, taping, electrotherapy, dry needling, acupuncture, osteopathy, chiropractor, massage therapy, kinesiology, proprioception, motor imagery, and nutrition). Studies investigating surgical procedures, pharmacological treatments, homeopathy or self-treatment were excluded.
Given the limited literature available on the effects of conservative treatment in dancers, no specific comparators were identified. Therefore, studies with conservative treatments versus no treatment, sham treatment or placebo or other types of interventions, including non-conservative treatments were included. Studies including co-interventions were included if they were applied equally to both the intervention and control group.
Two main outcomes were selected in this systematic review: pain and function. Pain outcomes included pain intensity and quality. Included function outcomes were related to range of motion (ROM) or position, flexibility, balance, strength and conditioning (e.g., strength, power, muscular or aerobic performance); movement performance (e.g., task completion, movement quality); motor control (e.g., muscle activation); and time that participants had to refrain from dancing or change their technique.
Study selection
The literature search results were uploaded to the Zotero software and duplicates were removed. Teams of two reviewers determined the eligibility of each article by reading the titles and abstracts. Every abstract that appeared to match the eligibility criteria was assessed using the full text. The final selection of articles included in this systematic review was made using the full text. For all three phases, disagreements were resolved by consensus. If a consensus could not be reached, a third reviewer (JBP) was involved.
Data extraction
Two teams, composed of two reviewers each, then independently extracted the information for each study included using a standardized data extraction table. The following information was extracted: design of the study, population, sex, sample size, intervention details, outcome measures used, relevant results of the study and risk of bias score. Authors were contacted if necessary.
Risk of bias assessment
The articles included were reviewed for risk of bias using the Downs and Black checklist by two independent groups of reviewers.16 This checklist allows the assessment of both RCTs and non-RCTs, and comprises 10 items evaluating reporting of data, three items evaluating external validity, 13 items regarding internal validity and one item evaluating power. Each item is rated 0 (no or unable to determine) or 1 (yes), with the exception of the fifth item on the description of confounders that is rated 2 (yes), 1 (partially) or 0 (no). This tool showed good test-retest and inter-rater reliability with high quality index and internal consistency.16 A total score was calculated by summing all items, and quality was interpreted as excellent (26-28), good (20-25), fair (15-19) or poor (≤14).17
Strategy for data synthesis
Data was aggregated and a narrative critical analysis was conducted. Descriptive data were used to characterize the study population. A narrative report on the findings was completed to provide avenues for future research and practice. A meta-analysis was not attempted.
RESULTS
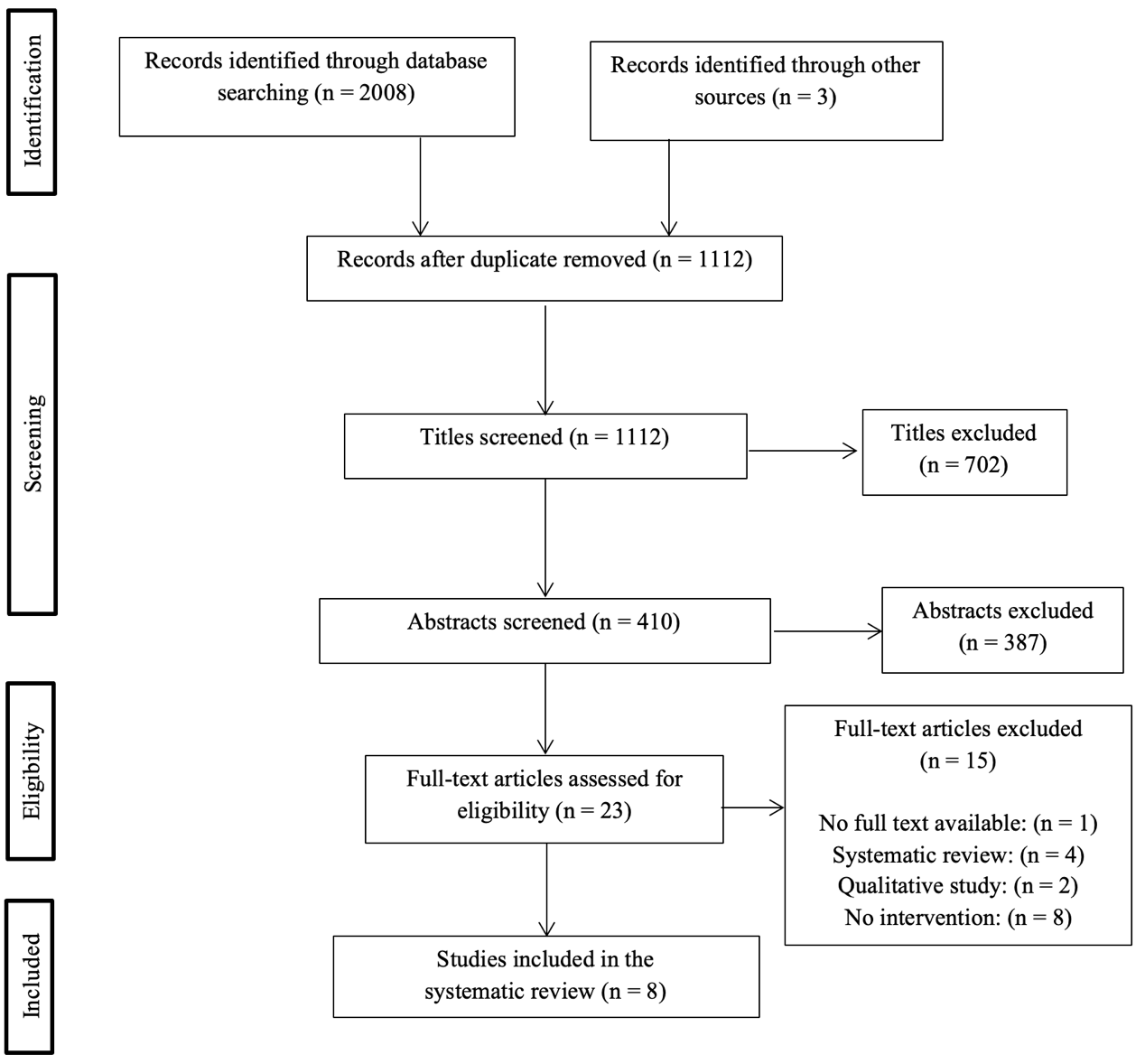
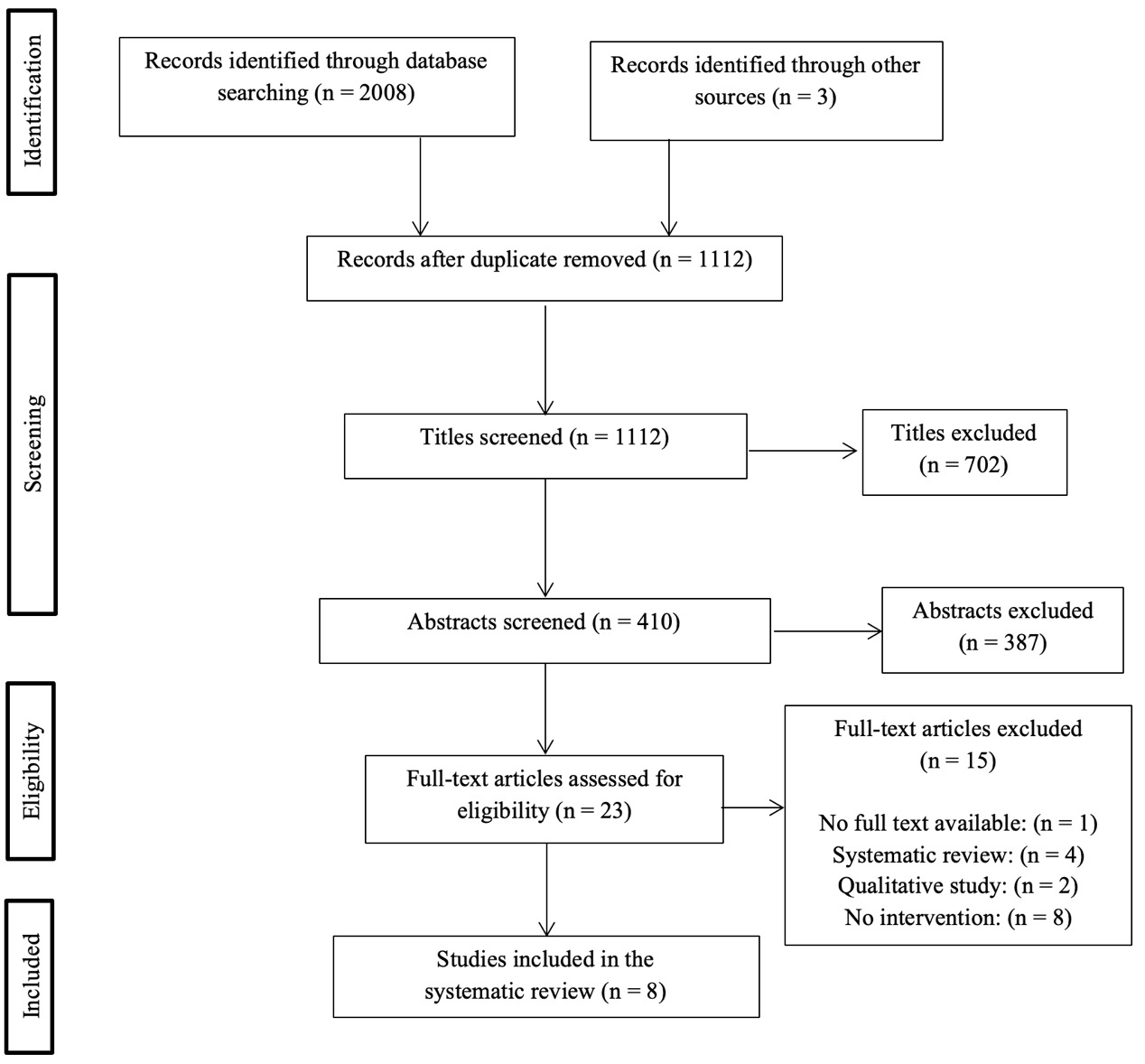
A total of 2,011 titles were identified following the database search (Figure 1). Once duplicates were removed, 1,112 titles remained. Of those, 1,089 were excluded based on inclusion and exclusion criteria using the titles and abstracts. The full text of 23 articles were obtained and assessed, and 15 were excluded, yielding eight studies that were included in this systematic review.
Risk of bias
According to the risk of bias assessment, two studies were scored as poor,10,18 four were evaluated as fair19–22 and two were rated as good.11,12 Table 1 presents evaluations for each study’s risk of bias using the Downs and Black checklist.
The risk of bias was derived from several factors. Most studies did not clearly describe the distribution of the principal confounders and the adjustments that were made in the analysis to account for those confounders. No studies reported on the possible adverse events of their intervention. Moreover, five out of eight studies failed to describe whether the participants contacted at recruitment were representative of the population and likewise, if the participants included in the study represented the population. Many of the studies had a high risk of bias due to the lack of blinding of the intervention from the participants, health care workers, and staff. Few studies used randomization, which was also one of the main risks of bias. Finally, no studies described how their sample size was sufficient to detect a clinically important change.
Study characteristics
Table 2 presents a summary of the characteristics of the included studies. Study designs included two prospective cohort studies, one uncontrolled trial, one within subject quasi-experimental study, one randomized cross-over study, one within-subject experimental study, one pilot RCT and only one RCT.
Dance shoes
One crossover study examined two types of toe caps for pointe shoes in professional ballet dancers, who had an onset of hallux valgus or a sprained first metatarsal medial collateral ligament (N=10).19 The effects on pain intensity using the visual analog scale (VAS) and on the hallux deviation angle using X-rays were measured in a single session, where the dancers used two different toe caps. The study found that the customized toe cap caused less pain when dancing en pointe than the standard toe cap. The hallux deviation angle was lower with the customized toe cap compared to the standard toe cap.
Dry needling
One pilot study explored whether dry needling applied to trigger points on the triceps surae of dancers affects pain, ankle range of motion and ankle joint torque in plantar flexion at 60, 90 and 120 degrees/second.20 The researchers randomized dancers to a dry needling intervention (N=5) or a sham dry needling intervention (N=4). Dry needling was applied to trigger points on the triceps surae muscles of professional dancers. Dancers also received two 30-second stretches on a slanted board after the dry needling or sham dry needling intervention. No significant differences in pain (p≥0.246) or ROM (p≥0.093) were observed within and between groups. There was a decrease in temperature bilaterally, in the triceps surae trigger points, following the sham dry needling treatment (p=0.008) and in the right calf for the dry-needling group (p=0.048). Ankle torque at 60 degrees/second increased for the left calf in the dry needling group from pre- to post-treatment (p=0.027). Ankle torque at 90 and 120 degrees/second showed no significant difference pre- to post-treatment within or between each group (p≥0.108).
Motor imagery
The non-randomized study by Gildea et al. investigated trunk stiffness and damping of the trunk during a forward or backward perturbation was applied to the trunk. They compared the natural postural response at the pre-treatment condition versus the postural response following a motor imagery intervention that aimed to elicit a fluid response in healthy dancers with (N=22) and without (N=8) a history of low back pain (LBP).23 The authors found no difference in stiffness between dancers with or without a history of LBP in the natural postural response pre-treatment condition, however there was a significant decrease observed in both groups following motor imagery. They also found that dancers without LBP had significantly higher trunk damping than dancers with a history of LBP (p=0.034) in the natural response condition. However, when using motor imagery to elicit a fluid reaction to the trunk perturbations, dancers with LBP had a similar level of trunk damping to dancers without LBP (p=0.226).
Conditioning/training programs
The conditioning and training programs used with dancers were investigated in five studies.10–12,18,21 The programs used were either the same for all dancers10–12,18 or tailored to an individual’s specific needs.21
Only one RCT was conducted on training programs to prevent injuries in dancers.11 Roussel et al. found no differences in aerobic capacity and explosive strength after a four-month conditioning program compared to the control group, which followed a health promotion program without any active exercises.11 It was nonetheless noted that the group that completed the conditioning program showed a decrease in their pain scores on the SF-36 and had fewer lower back pain complaints compared to the control group.11
All other studies were prospective and had no control group.10,12,18,21 Multiple outcomes were investigated, including aerobic endurance, strength, function, balance, stability and injury incidence.
Aerobic endurance was investigated using the Aerobic Power Index submaximal test in a study by Mistiaen et al. (N=40).12 They administered a weekly training program for six months that included aerobic endurance, local muscle strengthening and endurance, motor control, proprioception and coordination. A significant increase in aerobic capacity was found in the dancers who completed the training program. However, a similar program was used in the above-mentioned RCT by Roussel et al., and no differences were found between the experimental and control groups.
Strength was measured using the standing broad jump test12 and a subjective assessment of dancers.18 Following their training program, Mistiaen et al. found that the explosive strength of the dancers increased from pre- to post-treatment.12 However, no differences between the intervention and control groups were found when introducing a control group, as was done in the study by Roussel et al.11 Based on subjective data, Welsh et al. (N=8) found that dancers, who initially mentioned that their dancing was negatively affected by poor back strength, did not feel this way anymore following the strength training program.18
Function was evaluated using the Dance Functional Outcome Survey,10 and arabesque height was measured using the angle on a printed photograph.18 Long et al. administered a bi-weekly training program for a five-week period to professional contemporary ballet dancers (N=6).10 This training program included basic movement pattern exercises (bridges, planks, single leg deadlifts, lunges, squats, step ups and jumping). The movements became more specific to dance as the program progressed. They found that dancers had higher function following the program, as measured by the Dance Functional Outcome Survey.10 Welsh et al. compared mean arabesque height in dancers following a back strengthening program from pre- to post- treatment.18 They found an increase in arabesque height on photographs, although this difference was not supported by inferential statistical analysis.18
Balance was evaluated using the modified Star Excursion Balance Test in one within subject quasi-experimental study.10 Following the training program, balance increased in dancers from pre- to post-treatment.10 However, a within-group difference was found from the pre- to four-month follow-up for only one composite score of balance.10
Stability was evaluated only in one within subject quasi-experimental study, using the single-leg hop for distance for ankle and knee stability, as well as the Closed Kinetic Chain Upper Extremity Stability Test for upper extremity stability.10 Following the training program, the ankle and knee stability of the dancers increased from pre- to post-treatment, as well as from pre- to four-month follow-up.10 Similar results were obtained for upper extremity stability, although there was no within-group difference from pre- to four-month follow-up.10
Injury incidence was evaluated using the time-loss definition and assessed by an in-house physiotherapist. In a prospective cohort study, Allen et al. followed professional ballet dancers for three years (Year 1 N=52, Year 2 N=58, Year 3 N=53).21 The program for the first year was based solely on results from a pre-season screening using the Functional Movement Screen (FMSTM). The program for years two and three was based on both the FMSTM results and the dancer’s injuries, cause of injuries, and the final outcome of the previous injuries (still injured, recovered with compensations, or recovered). It was found that the injury rate dropped in the second and third year compared to the first year. The RCT by Roussel et al. also found a decrease in reported injuries following a conditioning program, although this was specific to low back injuries.11
DISCUSSION
The aim of this systematic review was to describe the different conservative interventions commonly used and their effect on MSK disorders in preprofessional and professional dancers. MSK disorders are a major concern for dancers, and this review identifies different conservative treatments that have been used, as well as the level of evidence supporting each intervention. The most commonly reported treatment was the training or conditioning program, whether it be general or individualized. The use of dry-needling, customized toe caps and motor imagery was also described in literature. The interpretation of these findings is however limited by the low number of studies as well as weak methodological designs and moderate to high risk of bias for the majority of the included studies.
The use of appropriate footwear is crucial for dancers. For example, the use of “dead” pointe shoes, i.e., pointe shoes that have lost structural integrity in the toe box or shank, was reported to affect muscle activation and biomechanics, which makes it more demanding for dancers to execute common movements, such as relevé or arabesque.24 In a randomized crossover study with a moderate risk of bias, the use of customized toe caps seemed to yield positive results for pain and the deviation angle of dancers with hallux valgus or first metatarsal hypermobility. However, costly customized toe caps are not commonly available to most dancers, and few dancers would have access to this kind of comprehensive assessment. Therefore, while interesting, this treatment would be difficult to implement in current clinical practice. Moreover, since the study included only a single session with pre- and post-treatment evaluations, long-term use should also be investigated. An analysis of costs and benefits could be conducted to evaluate the relevance of implementing this intervention in dance schools and companies.
The investigation of novel treatment strategies, such as dry-needling, customized toe caps and motor imagery, while interesting, showed a high risk of bias that impeded strong conclusions. Dry needling is a treatment technique that is usually delivered by a physical therapist, which has yielded promising results for decreasing pain, increasing range of motion and improving functional outcomes as well as strength in athletes.25–27 Indeed, in overhead throwing athletes with scapular dyskinesia, a RCT showed that the combination of dry-needling and manual therapy was more effective than manual therapy alone to reduce pain while playing and increase function during sport.25 Similarly, dry needling of trigger points in the gluteus medius and quadratus lumbarum combined to exercise therapy was more effective than exercise therapy alone to reduce pain and increase function in female athletes with patellofemoral pain.26 Another RCT found that, in elite soccer players, dry needling was more beneficial for hip flexors endurance and hip range of motion in the hip, after the treatment but also 4-weeks post-treatment compared to placebo laser.27 In the current systematic review, although there was a decrease in temperature, as measured by a thermometer, of the trigger points and an increase in plantar flexor torque at 60 degrees/second from pre- to post-treatment, the results from the pilot RCT by Janowski et al. had a high risk of bias. Some dancers were familiar with the twitch response that can be elicited through dry needling, and they could have thus guessed their allocation group. There were also two dancers who were not blinded in the sham group because they requested not to receive the dry needling intervention. Moreover, the sample was small and probably could not detect significant change. Considering the literature on dry needling and its positive effect on other athletes, this intervention should be further investigated in dancers.
While research on motor imagery in dancers is still emerging, the effect of this technique on performance is supported in different populations of athletes.28–30 In athletes, it has been mostly studied in terms of its effect on performance rather than prevention or treatment of injuries. In basketball players, it was found that motor imagery protocol was more effective to improve physical performance compared to a control and preintervention group.28 Its use has also been supported in non-athletes in the rehabilitation of knee injuries by a recent scoping review.31 Indeed, motor imagery interventions contributed to a better clinical outcome of function and pain.31 In dancers, motor imagery practice seems to improve performance of movements,32 and even mood.33 Moreover, dance teachers have been using images to convey the proper way of completing movements for decades.32 The study by Gildea et al. is of particular interest as it shows that dancers with a history of LBP and impairments in trunk stabilizer activation22,34 can use motor imagery to increase their damping abilities to the same level as dancers without a history of LBP. Motor imagery practice is especially interesting since it requires no costly equipment and could be implemented by either health care professionals or dance teachers. However, this study had a moderate risk of bias. Future studies should investigate the use of motor imagery in combination with other interventions to prevent or treat dancers with MSK conditions.
The majority of studies included in this review investigated conditioning or training programs. These interventions have been widely researched in other athletes and have proven to be effective to prevent certain injuries, especially among female athletes.35–37 Indeed, a systematic review found that neuromuscular training, including interventions such as strength, balance and proprioceptive exercises, was effective to prevent ankle injuries in female athletes.35 In another systematic review, it was found that strength, balance and plyometric exercises were effective to prevent anterior cruciate ligament injuries in male and female athletes.36 An additional systematic review on female athletes found that neuromuscular training including plyometric exercises was the most beneficial to prevent anterior cruciate ligament injuries.37 While these findings are important and relevant, dancers are a unique population as they are both artists and athletes. The studies included in this review combined multiple components in their programs. They were delivered between one and three times per week, for a period ranging from five weeks to three years.10–12,18,21 Uncontrolled prospective studies with varying risk of bias showed improvements in pain, aerobic capacity, explosive strength, balance and stability.10,12,18,21 It should however be noted that the only study with a robust design (RCT) and low risk of bias did not find any difference in aerobic capacity and explosive strength between groups, but found a decrease in pain and lower back injuries pre- to post-treatment.11 As no sample size calculation was provided in this study, it is not possible to exclude the fact that the non-significant differences observed between groups could be attributable to lack of statistical power. Therefore, additional RCTs with a sufficient sample size would be necessary to confirm the benefits observed in the included studies.
Future directions
In a sport with such specific demands and high expectations of performance, effective treatment that allows the artist to return to dancing is imperative. In the literature on the treatment and prevention of MSK disorders in athletes, multimodal interventions seem to be key in improvements of pain, function, and a prompt return to sport.
Future research on the treatment of MSK disorders in dancers should therefore include multimodal approaches, including training and conditioning programs integrated to novel components like motor imagery and dry-needling. Moreover, future research should focus on conservative interventions adapted to the athlete and type of dance, as well as to the athlete’s development during the rehabilitation or prevention program. More importantly, studies need to use a robust design and include control groups to ensure that the sole taking care of dancers or placebo effect does not interfere. In order to analyze the changes in the incidence of MSK disorders and injuries following conservative treatments, there is an urgent need to establish a clear and standardized definition for MSK disorders in dancers.
Limitations
This systematic review is inherently limited by the quantity and quality of the studies included. Since there were no exclusion criteria based on the risk of bias assessment, all studies were retained for the review regardless of their quality. Interpretation of results are limited as most studies did not include a control group or blind the dancers to their group allocation. Moreover, most studies also had a small sample size and no sample size calculation to justify such a limited number of participants.
The few studies included in this review had widely different populations in terms of professional or preprofessional status and dance style. Robust conclusions that would apply to the entire population of dancers that were studied is therefore difficult considering the different training, schedule, and mindset of these dancers.
CONCLUSION
Although this review highlights some promising treatment and prevention avenues for dancers, a strong interpretation of results was limited by the insufficient acknowledgement of confounders, concerns regarding external validity, insufficient power, as well as lack of randomization and blinding participants, health workers and staff. More high-quality studies are needed to reach any solid conclusions. Dance researchers should focus on the addition of control groups to their studies, as well as multimodal interventions. Indeed, the use of multimodal conditioning programs yielded significant early results on pain, function, and balance in uncontrolled prospective studies. This multimodal treatment should be investigated in RCTs. Moreover, researchers should explore the idea of individualized conditioning programs, tailored to the dancers’ limitations.
Acknowledgements
The authors would like to acknowledge the collaboration of Marie Chrysagis, Carolane Giroux, Janne Pintal, Audrey Thibert, Romy Lambert-Hevey, Liliane Dubé and Laurie Morelli-Valiquette for their assistance with the search strategy.
Conflicts of interest
The authors report no conflict of interest.