INTRODUCTION
Within the adult population, 67% of individuals will experience shoulder pain at some point throughout their lifetime.1 There are numerous factors related to the etiology of shoulder pain and it has been hypothesized that the presence of scapular dyskinesis (SD) is a contributing factor to shoulder pathology.2,3 Scapular dyskinesis has been defined as alterations in scapular positioning at rest as well as during dynamic movement. Common variations in scapular movement4,5 include increased scapular superior translation along with reduced scapular posterior tilt, upward rotation, and internal rotation.6 Give the theorized relationship between SD and certain shoulder pathologies there have been several methods proposed to evaluate these alterations in scapular positions and movements.
McClure et al.7 developed a commonly used method of identifying SD, the scapular dyskinesis test (SDT), to identify the presence of SD and classify individuals into three levels: normal motion, subtle dyskinesis, and obvious dyskinesis. This is one of several methods commonly used during an evaluation related to shoulder pathology presented in Supplement A Though the SDT has been proven to be a reliable and valid method of identifying SD6,7 not all clinicians are trained to use this tool and current literature describes a wide variation of assessment methodology.6 Along with this lack of homogeneity in assessment of SD, there is a lack of evidence to support the idea that identification and correction of SD may help to prevent or treat shoulder pathology. Even with this lack of evidence, identifying SD is a common screening tool for both symptomatic and asymptomatic individuals. The evaluation is especially common in predicting or preventing injury in overhead athletes, however there is conflicting evidence regarding the link between SD and injury in this population exists.8,9 Clinicians often direct their treatment toward correcting the SD which could be normal movement variability.10,11
Because the identification of SD is a common part of a patient evaluation, it is often used to guide clinical decision making; however, there is considerable debate around linking the presence of SD to certain shoulder pathologies. Some studies have shown no difference in the prevalence of SD between symptomatic and asymptomatic populations.12 This raises the question of utility when screening for SD in patients seeking treatment for shoulder pain as well as for the asymptomatic population.
The purpose of this systematic review of the current literature to investigate the prevalence of SD among both symptomatic and asymptomatic populations. Understanding the relationship between SD and the presence or absence of symptoms may help to direct conversations regarding the clinical utility of SD. The authors hypothesized that SD is a common finding that has been medicalized (clinical findings suggested to require treatment but is ultimately a normal finding).
MATERIALS AND METHODS
Guidelines
This systematic review utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines during the search and reporting phase of the research process. The PRISMA statement includes a 27-item checklist designed to improve reporting of systematic reviews and meta-analyses.13
Literature search
An online literature search was conducted utilizing PubMed, EMBASE, Cochrane and CINAHL from the dates of their origin until July 2021. The search strategy was created and performed by a biomedical librarian. An example of the search strategy used for the PubMed database is provided (Supplement B) and similar strategies were utilized for the remaining databases. The study was registered using the International Prospective Register of Systematic Reviews (PROSPERO) in May of 2020 with a corresponding reference number: CDR42020187045.
Study selection
All titles were independently appraised by two authors (TB) and (AW) after the initial online literature search for studies to be retained. The abstracts of these titles were read to determine if the studies met the inclusion criteria. Studies with abstracts that met the inclusion criteria were accessed in their full-text format and then read to determine their eligibility for the review. The same two authors performed the study selection process for this review with a third author (PS) available to handle disagreements. The inclusion criteria for studies to be retained in the present review consisted of: (a) individuals being assessed as having SD, including reliability and validity studies (b) subjects aged 18 or older; (c) sport and non-sport participants; (d) no date restriction; I symptomatic, asymptomatic, or both populations; (f) all study designs except case reports. Studies were excluded if: (a) they were not published in the English language; (b) they were a case report design; (c) the presence of SD was part of the studies inclusion criteria; (d) data were not present distinguishing the number of subjects with or without SD; I they did not define participants as having or not having SD.
Data extraction
The data and results from the studies that were retained as part of the review were extracted using a format to identify study type, population, methods for evaluating SD, and the prevalence of SD. Data were extracted, reviewed, and analyzed by the primary author (PS) and verified by a research assistant (ZS). Discrepancies in data collection were resolved through discussion.
Methodological Quality Assessment Tool
The Joanna Briggs Institute (JBI) checklist for prevalence studies was used to evaluate methodological quality within the individual studies.14 There are nine items related to methodological quality included in the checklist which can be answered as yes, no, unclear, or not applicable. Following the scoring of each item, those individuals scoring the study are asked to provide an overall appraisal to include, exclude, or seek further information regarding if the article should be retained. The decision to include or exclude each article is then made by the reviewer(s) based on the completed checklist and consensus. Two authors, (DH) and (AM), performed the methodological quality assessment independently with discrepancies handled by the primary author if necessary. Prior to methodological quality assessment those involved in worked through scoring several unrelated prevalence studies in order to align definitions and interpretations of the various elements present in the JBI tool.
Data Synthesis and Analysis
Data were extracted and pooled to include the incidence of scapular dyskinesis, as defined by the authors, among those individuals that were symptomatic and those that were asymptomatic. The results were reported on percentage of incidence differentiating between classification of individuals with SD and shoulders with SD among each identified population. Data on relevant subcategories were identified and individually accounted for with separate analyses. Data from the identified studies did not allow for a quantitative analysis given the heterogeneity of several variables.
RESULTS
Search Results
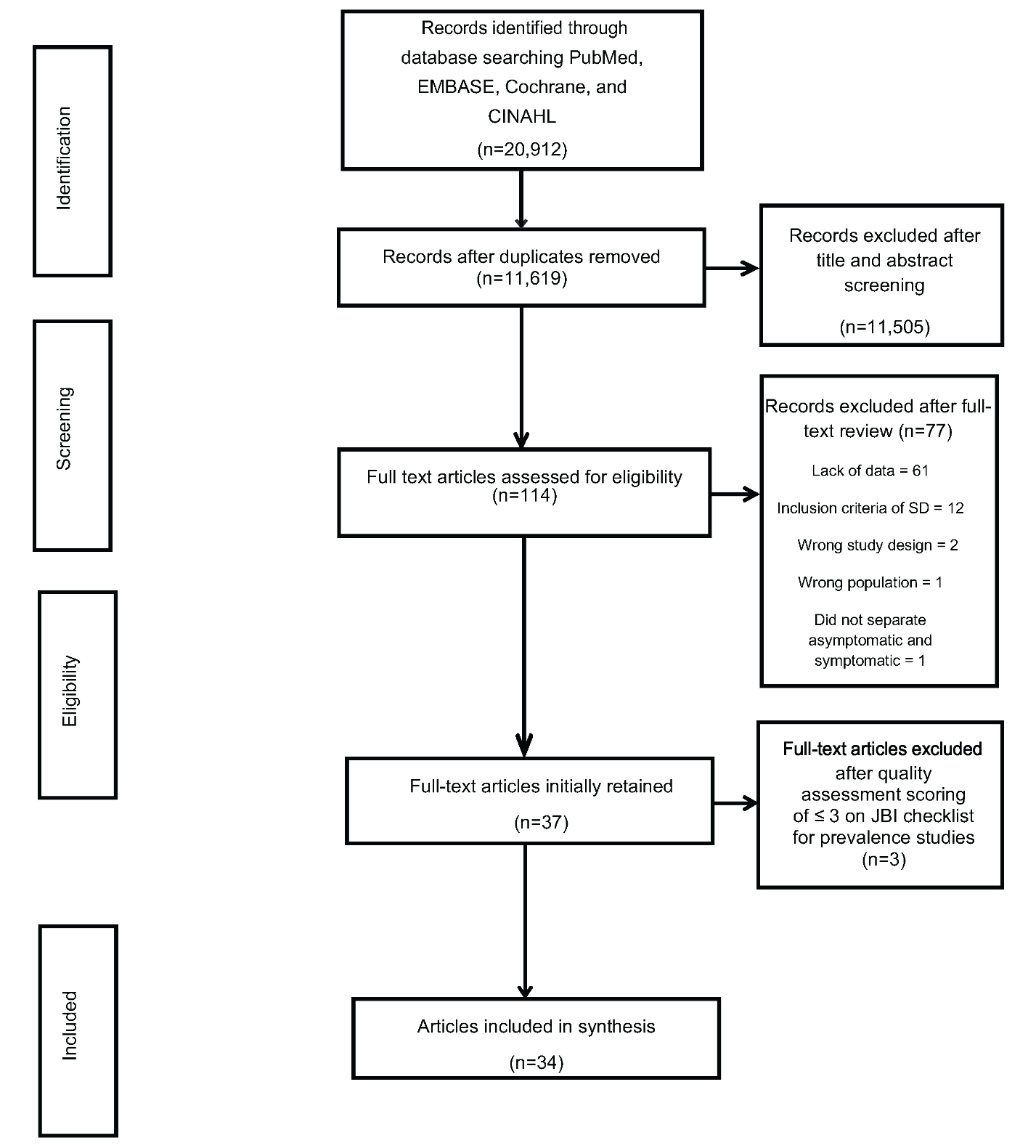
The initial search resulted in 11,619 after duplicates were removed. Following title and abstract screening 11,505 were removed. Full text articles were retrieved for the remaining 114 studies of which 77 were removed due to not meeting the inclusion criteria. The remaining 37 studies were retained for quality assessment Figure 1.
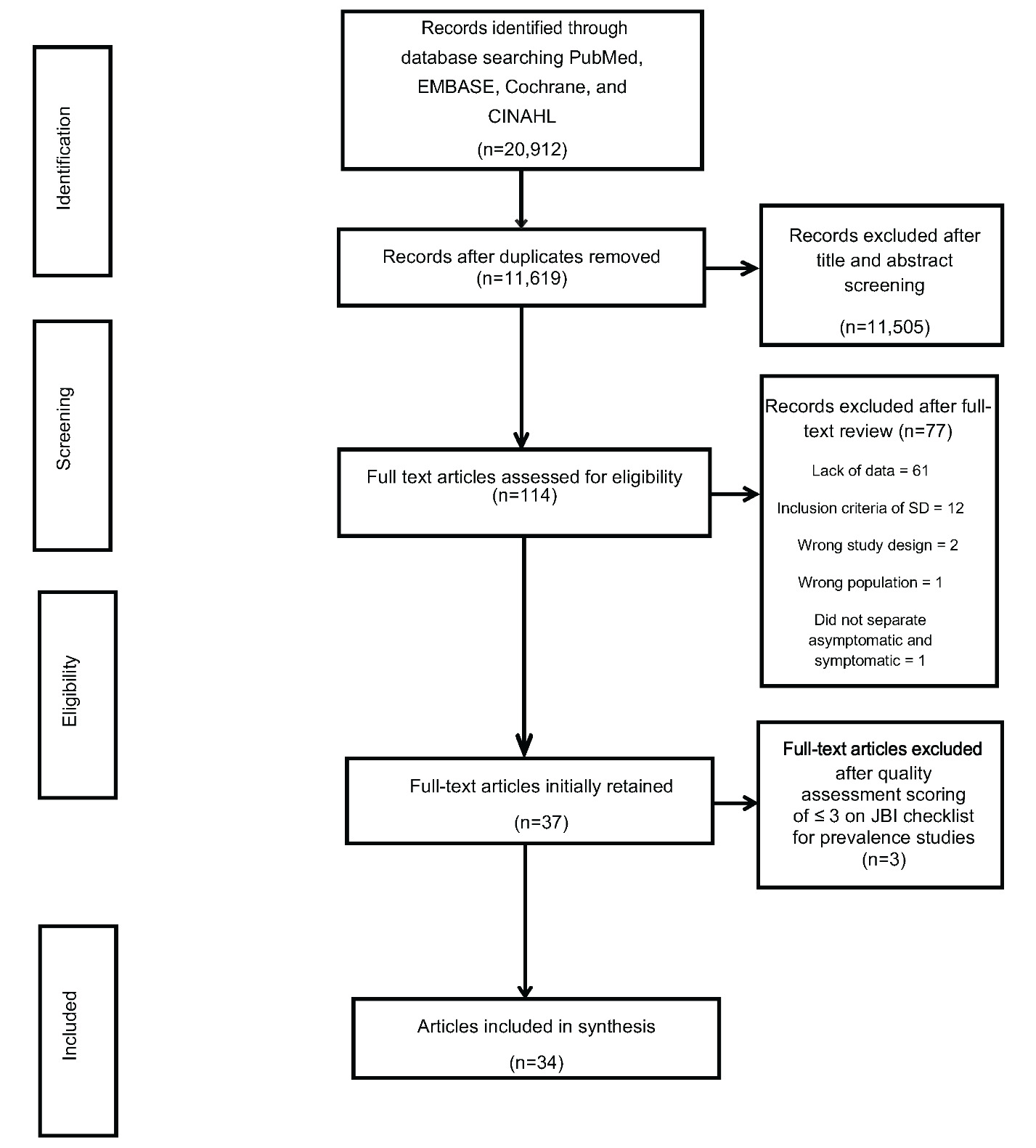
Following quality assessment 34 articles were ultimately retained for analysis. Study characteristics for each of the 34 studies consisting that examined 2,365 individuals can be seen in Table 1. Retained studies were categorized into either symptomatic or asymptomatic within either an athletic population or a general orthopedic population.
The general orthopedic population among the retained studies included study participants where the upper extremity was of interest, primarily the shoulder. However, there were a small number of individuals that had neck pain where SD was also evaluated, which is more clearly identified in the results section.
Methodological Quality
Of the 37 articles assessed three15–17 were excluded and 3412,18–50 were included for synthesis (Table 2).
The excluded articles all had a score ≤ 3 on the JBI tool. The reasoning for exclusion of articles was to remove poor quality studies due to low quality or high risk of bias. Otherwise, there would be little value in scoring quality if high- and low-quality studies are all given the same “voice”. Additionally, the JBI tool is specifically designed to give the raters the choice of including or excluding the scored study based on their interpretation of the scoring. Of the included studies, 1812,21–27,32,37–41,44,45,49,50 addressed the target population appropriately with the sample frame and had adequate sample sizes. However, only 13 studies12,19,23,24,26,28,31,32,41,42,47,49,50 reported both the study subjects and setting in detail. Additionally, 11 studies19,20,22–24,26,27,38,45,47,50 measured the condition in a standard reliable way, 15 studies12,19,22,23,26,30,32,34–36,40–42,48,50 used valid methods to identify the condition, and 8 studies21,22,32,37,39,41,48,50 included information on response rate as most studies were one-time measures. The JBI tool, like other quality and risk of bias assessment tools, does not advocate for a summative score as the constructs being scored are not similar. Therefore, in order to be as transparent as possible, we listed each item in the table along with their score, as well as provided a summary of those studies and which were the most common items not reported as you mention above.
Prevalence Results
The number of studies with available data for the asymptomatic and symptomatic populations and relevant subgroups are reported. Table 3 reflects studies with available subgroup data for asymptomatic and symptomatic populations. Data for asymptomatic individuals are reported in Table 4. Finally, symptomatic athletic population results are reported in Table 5 while the asymptomatic general population results ae reported in Table 6.
Although the inclusion criteria were intentionally broad in respect to diagnoses for the symptomatic population, all but three studies20,35,40 consisted of individuals with some form of shoulder pain including diagnoses such impingement, instability, rotator cuff tear, labral tear, and upper extremity pain, all of which are listed in Table 1. Two of the three studies35,40 consisted of mixed upper extremity diagnoses but the SD data was not parsed out by diagnosis. The authors were able to examine them based on the inclusion criteria. This was an attempt to be transparent in instances were other diagnosis outside of shoulder conditions may have been considered as we were examining those studies that identify SD but could have been in a population of individuals with cervical or upper extremity conditions. The remaining study20 included individuals with neck pain only with a total number of 19 subjects. Within the studies for the symptomatic athletic and general orthopedic population there were 81% and 57% individuals with SD, respectively, and a total of 60% among both groups. The two studies within symptomatic athletic population that looked at both shoulders individually demonstrated a total of 79% of individuals with SD considering at least one shoulder. Within the studies for the asymptomatic athletic and general population there were 42% and 59% individuals with SD, respectively, and a total of 48% among both. The four studies within asymptomatic general population that looked at both shoulders individually there was a total of 42% of individuals with SD.
DISCUSSION
The purpose of this systematic review was to examine the available literature in order to report the prevalence of SD among both the symptomatic and asymptomatic population. The results of this systematic review indicate that there is an overall presence of SD of 60% among symptomatic individuals. Among the asymptomatic population there is an overall presence of SD of 48% among those studies that identify individuals with SD. The low number of studies that identified individuals with SD per shoulder makes it difficult to determine true differences between those with and without symptoms. Despite the overall prevalence of SD being higher among those with symptoms compared to those without, there is still a considerable number of those that present with SD (nearly half of those studied) that are asymptomatic which questions the relevance of this finding. Furthermore, the total number of symptomatic individuals, 650, within studies investigating SD was just over half the number of those studies investigating SD among asymptomatic individuals, 1,048. This was reported for transparency in how the data were presented.
When considering the population of those with general shoulder pain there were a total of 582 individuals within the studies examined in this review. Among this population there was a higher percentage of individuals with SD (57%) compared to those without (43%). However, whether SD is contributing to the symptoms experienced by this populations remains unclear. If SD is a contributing factor to the symptoms among the general orthopedic population with shoulder pain, then how is the high prevalence (57%) of SD among the general population studied without symptoms explained?
There is considerable discussion in the literature regarding the presence of SD among overhead athletes with or without symptoms, as well as the presence of SD being a potential risk factor for sustaining injury in the future.8,9,31,32,37 The current findings from the current study support the high incidence of SD among athletes with shoulder symptoms. However, it is important to note that only three studies with a total of 68 individuals investigated the presence of SD within the symptomatic athlete population while 16 studies with a total of 657 individuals investigating the presence of SD in the asymptomatic athletic population were included. Given the larger number of asymptomatic athletes who were described as having SD (from 20%-92%) it is clear that a large number of athletes present with SD and have no symptoms. This may indicate that it is a possibility that SD may be a normal adaptation for those participating in overhead sports.
Additionally, the timing of measuring SD is not consistently reported among the studies that contain overhead athletes and may add further evidence that SD is a normal adaptation within this population. Two studies31,32 measured SD of asymptomatic competitive swimmers at various points of an individual training session. Both studies found that as training progressed, the number of individuals presenting with SD increased with a large number of participants presenting with SD at the end of the training session (82%31 and 85%32). At first glance the initial perception may be that these results are suggestive of weakness or some compensatory mechanism that requires attention, however, it is possible that there is a normal adaptation related to the overall shoulder complex that causes this change to occur, particularly since these athletes were all competing at a high level without symptoms. This would not be unlike what is known regarding the increase in external rotation range of motion at the glenohumeral joint within a single game and over the course of the season in a baseball pitcher.51 Within baseball pitchers this adaptation is not only normal, but necessary to perform at a high level.
Limitations
There are several limitations to this systematic review. The first limitation is that only included studies published in the English language were included which may have excluded published studies on this topic. Additionally, a very strict inclusion and exclusion criteria was applied in order to identify those studies that would provide the appropriate data for the purpose of this study. Lastly, there is a lack of consistency among how SD is measured across studies as well as populations, so it was not possible to perform a meta-analysis.
CONCLUSION
Within the symptomatic population, athletes have a higher percentage SD than the general orthopedic population. However, there are a considerable number of individuals with symptoms that do not present with SD. Perhaps more revealing is the number of asymptomatic individuals that present with SD, suggesting that SD may be a relatively normal finding among nearly half of the asymptomatic population studied within the literature. Until longitudinal studies are completed that monitor the predictive value of SD over time amongst asymptomatic populations, the relevance of this finding will remain uncertain.
Acknowledgements
Melinda Johnson, Reference/Academic Support Services Librarian, Nova Southeastern University and Zachary Smith
Conflict of interest declaration
The authors declare no conflict of interest.