
INTRODUCTION
Ankle sprains are among the most common injuries in the general population and are the most frequently reported injuries by competitive athletes.1–3 The prevalence of lateral ankle sprains (LASs), coupled with high rates of reinjury, persistent symptoms, and self-reported reduced ankle function, makes LASs and their sequelae a public health concern.4 Residual symptoms from an initial LAS are identified as chronic ankle instability (CAI). Doherty et al5 conducted a prospective study on patients with first-time ankle sprains who sought treatment at the emergency department in a hospital and found that 40% had developed CAI at the 12-month follow-up. CAI describes a combination of mechanical and functional instability with the following residual ankle sprain symptoms6,7: pain, swelling, weakness, instability, and repeated episodes of ‘‘giving way’’.8 These potential long-term consequences highlight the need for suitable treatments for these conditions.
Balance training has been reported to be an effective modality for the rehabilitation and prevention of recurrent sprains in individuals with CAI. In their systematic review and meta-analysis, Schiftan et al.9 concluded that balance training effectively reduces the risk of ankle sprain in sports participants with a history of ankle sprains. Balance training generally involves maintaining a standing posture on an unstable surface. Training on unstable surfaces has been suggested to be a valuable aid for ankle sensory-motor rehabilitation.10,11 Previous studies suggested that training on stable ground may correspond with enhanced static postural control, whereas instability training may improve dynamic postural control.12,13
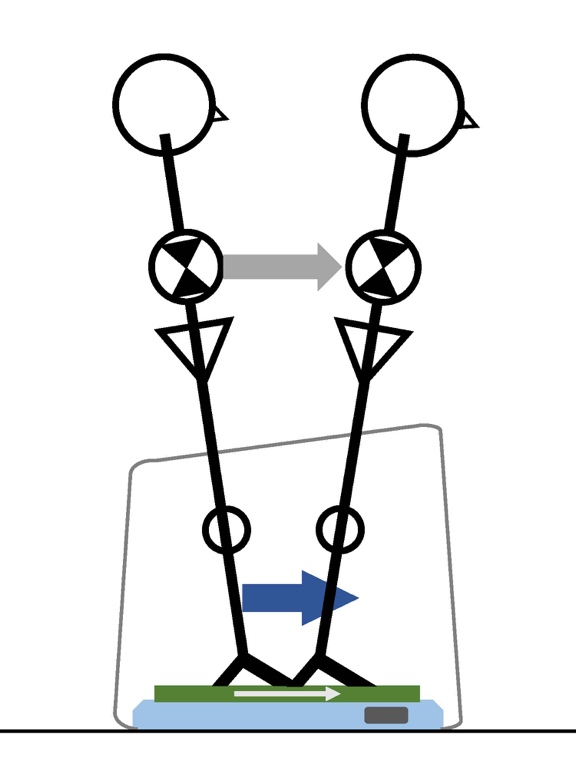
A real-time postural feedback system called the “balance adjustment system BASYS (MPF-5050B; Tec Gihan Co., Ltd., Kyoto, Japan)” was developed to establish a novel rehabilitation strategy for addressing postural control. The device adjusts between voluntary movements and reflects adjustments in an individual’s standing posture adjustment. In other words, the device helps the individual make the necessary physical adjustments to their posture, while also allowing their body to make automatic reflex adjustments as needed. By doing so, the device can assist the individual in maintaining a healthy and stable standing posture. Additionally, the BASYS can implicitly modulate an individual’s body sway, decreasing (in-phase mode) or increasing (anti-phase mode) it in real-time. Especially the in-phase mode differs from traditional balance training and constitutes an entirely new interventional stimulation method (Figure 1). Traditional balance training on unstable surfaces improves postural control by imposing sway on the patient. However, the in-phase mode of the BASYS supports standing postural adjustment and reduces sway by moving the plate in the same direction as the individual’s sway. These stimulations could be more effective than traditional balance training in treating the balance deficits that have been reported in patients with CAI and postural control disorder.

To the authors’ knowledge, the BASYS has been used primarily in elderly individuals and patients with neurodegenerative diseases; however, it has not been studied in younger individuals or patients with CAI. So far, it has been used in clinical practice, but there has been no detailed investigation of the BASYS device. Therefore, this study aimed to evaluate how a two-week program using the in-phase mode of the BASYS affects postural control in participants with CAI. The authors’ hypothesized that the BASYS (in in-phase mode) might lead to improved postural control compared with training on a balance disc.
METHODS
PARTICIPANTS
Twenty participants with CAI were recruited from several intercollegiate sports teams. Selection criteria for patients with CAI14 included participants who reported a history of at least one substantial ankle sprain (the most recent injury must have occurred more than three months before study enrollment), two or more episodes of the ankle ‘‘giving way’’ in the six months before the study, and a score ≤25 on the Japanese version of the Cumberland ankle instability tool.15 In participants with bilateral ankle instability, the ankle with the lower score was selected. The exclusion criteria were as follows: a history of previous surgery involving the musculoskeletal structures of either lower extremity; fracture in either lower extremity requiring realignment; or acute musculoskeletal injury to the joints of the lower extremity in the three months before the study, affecting joint integrity and function, and resulting in at least one lost day of desired physical activity.14
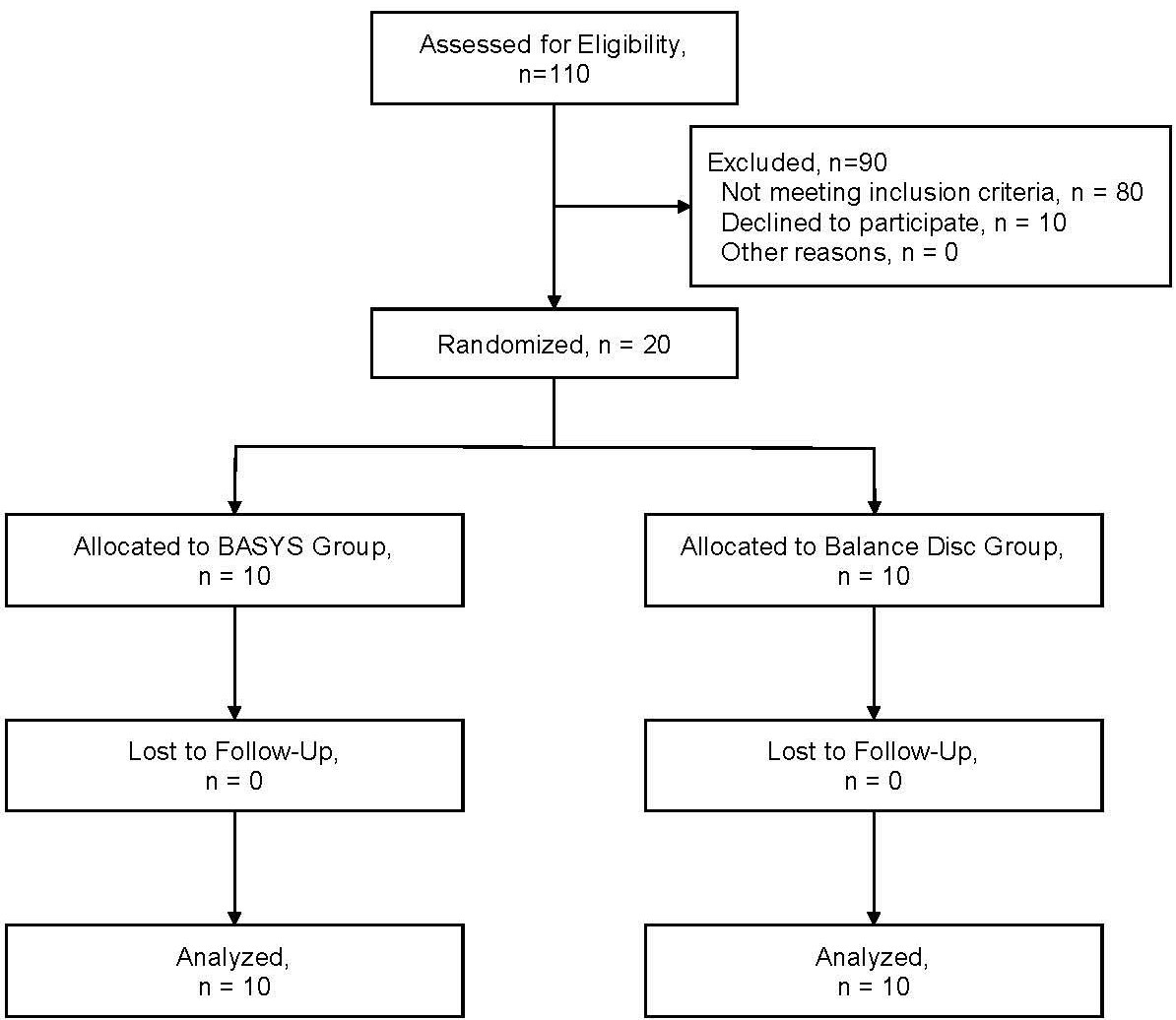
G*Power (Version 3.1.9.7) was used to determine the sample size. The calculation was based on the F test, with an alpha level of 0.05. The type II error rate was set at 80% power and the effect size of 0.3 of the primary outcome variable was taken from similar previous studies.10,11 The appropriate sample size for this study was determined to be 20 participants. The subjects gave informed consent to participate in the study. The participant flow chart as per the CONSORT statement is shown in Figure 2.

PROCEDURES
This study was a randomized clinical trial that compared two types of balance training over two weeks by measuring static and dynamic balance. The study was approved by an institutional review board or similar committee. Participants with CAI were randomly assigned to one of two training groups: in-phase mode on the BASYS or Balance Disc (BD; cushion type, Kbands Training). A simple randomization procedure (sequentially numbered draws from containers) was used to allocate study participants. Participants were assessed at three instances: pretraining (Pre), post-training 1 (Post1; after the first training session), and post-training 2 (Post2; after the last training session). In this study, static and dynamic postural control were considered dependent variables, while the groups and time were the independent variables (Pre, Post1, and Post2). Assessment of both groups before and after the two-week intervention period consisted of the center of pressure (COP) measurements during single leg standing with closed eyes and Y-balance test reach scores (YBT; anterior [A], posteromedial [PM], and posterolateral [PL] directions).
STATIC POSTURAL CONTROL
To assess static postural control, all participants stood on an instrumented BASYS (MPF-5050B; Tec Gihan Co., Ltd., Kyoto, Japan) in a single-limb stance (CAI limb only) with their hands crossed in front of their chest and their eyes closed (Figure 3). They were given the following instructions: “Remain as motionless as possible for 30 sec, and if you move out of position, please return to the original position as soon as possible and continue the trial.” The test was performed for 30 sec, and the following outcomes were then calculated from the resulting COP data: total trajectory length and 95% ellipse area. The test was conducted three times, with a 60-sec rest provided between the trials. Data were filtered using a low-pass digital filter with a cut-off frequency of 10 Hz using the software included with the BASYS. The total trajectory length of the COP refers to the length of the path taken by the center of the foot’s pressure distribution, based on data recorded from changes in pressure applied to the foot. Additionally, the 95% ellipse area represents the area of an ellipse that approximates the trajectory of the COP. In this study, when the load balance on the sole of the foot is good, the total trajectory length is shorter, and the 95% ellipse area is smaller. Conversely, when the load balance is poor, the total trajectory length is longer, and the 95% ellipse area is larger. The averages of the values recorded in the trials were used for the analysis.
_and_testi.jpeg)
DYNAMIC POSTURAL CONTROL
Dynamic postural control was tested using the YBT test apparatus (FunctionalMovement.com; Functional Movement Systems, Danville, VA). The YBT has been shown to be reliable (composite ICC = 0.89)16 in the measurement of individual reach directions: A, PM, and PL. The orientation of the reach direction was determined relative to the stance limb. Participants stood on the involved limb with the great toe behind the line on the platform located at the center of the three diverging lines. Measurements were taken as the participant pushed the target plate along the polyvinyl chloride pipe with the opposite leg. The participants were instructed to return to the starting position without losing balance after each trial. The test was conducted three times, with a 60-sec rest provided between the trials. The average values of the three trials were used for the analysis. The reached distances were normalized to the participant’s leg length, which was measured in centimeters from the anterior-superior iliac spine to the distal tip of the medial malleolus. The composite score (percentage) was calculated by taking the average of the three reached-distance average values divided by the participant’s limb length, multiplied by 100. The obtained value was used for statistical analysis.17
BALANCE TRAINING INTERVENTION
After baseline testing, the participants were randomly assigned to one of the two groups (BASYS or BD) in a 1:1 ratio. All participants then underwent a total of six supervised training sessions over a two-week period. Participants of both groups performed single-limb balance training sessions with their eyes open. During the task, they were instructed to cross their arms in front of their body and to look at the black curtain in front of them to avoid any visual effects.18 The black curtain was placed 70 cm in front of the participants. The training program consisted of one session of three 30-sec exercises with a 60-sec rest between the exercises. All exercises were carried out only on the unstable ankle and were performed barefoot. Participants in the BASYS group trained using the in-phase mode on the BASYS (Figure 3), whereas participants in the BD group trained with the DynaDisc on the floor. The BASYS used the anterior-posterior position of the COP in the standing position as a feedback signal to immediately move the floor surface in the front-back direction. The in-phase mode of the BASYS suppressed postural sway by moving the floor in the same direction as the sensed COP. The vibration of the BASYS floor movement could be set at 5%, 10%, or 15% of the sensed COP. In this study, COP was increased by 5% in each of the three exercises.
The training program (number of times, rest periods, number of sets, etc.) implemented in this study was based on the authors’ experience in clinical practice.
STATISTICAL ANALYSIS
Group demographics were compared using independent samples t-tests. A two-way repeated-measures analysis of variance was performed for all outcome variables to analyze the interaction among groups (BASYS, BD) and the time of assessment (Pre, Post1, and Post2). When the differences were established, a post hoc Bonferroni multiple comparisons test was used. The effect size (ES) was calculated for all pairwise comparisons according to the formula proposed by Glass et al.19 When a pairwise comparison was performed between the BASYS and BD groups, a pooled standard deviation for the calculations was used. The magnitude of the ES was interpreted using the scale devised by Cohen: small (<0.2), medium (0.5), and large (>0.8).20 All data are presented as means ± standard deviations. The α level was set at 0.05. Statistical analysis was performed using SPSS (version 26.0; IBM Corp, Armonk, NY).
RESULTS
Descriptive characteristics of the participants (11 females and 9 males; age, 20.9 ± 1.1 years; height, 165.2 ± 7.1 cm; mass, 62.3 ± 5.6 kg), after randomization into their corresponding training groups, are provided in Table 1. Independent t-tests indicated no group differences in age (p = 0.509), height (p = 0.198), or mass (p = 0.635) All randomized participants completed the entire study as allocated as shown in Figure 2, and none were harmed in the process. CAI participants were recruited from February 2021 to July 2021 and attended lab visits at the time of assessment and during the two-week intervention.
STATIC POSTURAL CONTROL
Results for static postural control are presented in Tables 2 and 3. There was a significant primary effect on time in the COP total trajectory length of the BASYS group (p = 0.035), but not for the 95% ellipse area (p = 0.126). The BASYS group total trajectory was significantly decreased for Post1 and Post2 values than the Pre value (Pre-Post1: p = 0.001, ES [95%CI] = 0.88 [-0.08,1.75]; Pre-Post2: p = 0.0001, ES [95%CI] = 1.02 [0.05,1.90]).
DYNAMIC POSTURAL CONTROL
Results for dynamic postural control are presented in Tables 4 and 5. Group differences (p > 0.05) and time-by-group interactions (p > 0.05) were not observed for either of the YBT reach distances.
DISCUSSION
The primary finding of this study was that two weeks of intervention with the in-phase mode of the BASYS improved static postural control in participants with CAI. Overall, these results support the use of balance training with the in-phase mode of the BASYS to address static postural control impairments in individuals with CAI. It was also hypothesized that dynamic postural control could be improved with intervention in the in-phase mode of the BASYS, however this hypothesis was not supported due to no changes in any post-intervention YBT reach distances variables.
The results showed that training using the in-phase mode of the BASYS decreased the total trajectory length of COP (p = 0.001, 0.0001) while there was no effect of training the BD for the same measure (p = 0.092, 0.676). Furthermore, the effect sizes from Pre to Post1 and Post2 were moderate to large for static postural control variables due to the intervention using the BASYS.
Static postural control was defined as the ability to balance on a stable surface without intentional movement by the participant, like a measure of postural sway on a force plate.21 The interventional stimulation in the in-phase mode of the BASYS can be performed with an extremely small movement in the front-back direction and with a small amplitude load while the ground surface remains horizontal for the participant’s COP. A single-legged stance on a firm surface evokes the lowest overall muscle activity levels for EMG.22 In addition, the use of a uniaxial balance board showed that, based on foot orientation, the agonist-antagonist co-activation can be controlled to some degree.22 Therefore, in this study, the intervention of stimulation by the BASYS in the in-phase mode may have contributed to the coordination of fine body movements of participants with CAI, reducing the postural control demands and improving the total trajectory length of COP.
Regarding dynamic postural control variables, no differences were found between the intervention in the in-phase mode of the BASYS and the intervention on unstable surfaces, indicating that the intervention utilized in this study did not improve dynamic postural control. The authors chose to incorporate isolated exercises, whereas a more comprehensive rehabilitation program addressing mechanical restrictions, plantar cutaneous deficits, strength, and static postural control may be more appropriate for improving reach distances and result in better functional outcomes.17 Further research in patient populations with CAI is necessary to evaluate the possible additional benefit of intervention in the in-phase mode of the BASYS.
Importantly, there was a significant decrease in the total trajectory length of static balance with intervention in the in-phase mode of the BASYS within a brief treatment period, from immediately after the intervention to two weeks after. This result was initially due to exercising in the in-phase mode on the BASYS, which may be considered for inclusion in a rehabilitation program for CAI. In previous studies, improvements were evident in postural control in four-week other intervention programs for participants with CAI.23–25 McKeon et al,26 who studied individuals with both new and recurrent ankle sprains, noted a substantial increase of up to approximately 70% in the probability of returning to play on day three following an injury. Roughly 90% of those injured returned to participate within one week.26 These results suggest that rehabilitation programs in the early period of CAI and ankle sprain should be conducted for improved outcomes.
Considering the results of the present study, future research should assess whether combining the in-phase mode of the BASYS and conventional methods can enhance improvements in dynamic postural control, providing a new direction for balance training following ankle injury.
This study has some limitations. The interpretation of the exercises was solely based on the postural control variables. To assess the intervention in the in-phase mode of the BASYS, it would be interesting to observe the effect on the evoked muscle activation levels or functional outcome measures. A BD was used for the control group in this study. Further research is needed to exclude cognitive bias. There is ample room for evaluation of the optimal training programs using the BASYS device.
CONCLUSION
This is the first study to assess the efficacy of the BASYS used in the in-phase mode as an intervention tool to address post-CAI postural control deficits. The total trajectory for COP decreased from Pre to Post1 and Post2 in the BASYS group. Furthermore, large to moderate effect sizes in terms of static postural variables were evident in the BASYS group. However, both groups did not demonstrate improved dynamic postural control outcomes. Therefore, whether the BASYS or BD groups have the greatest effect on improving dynamic postural control remains unknown. Evaluating how postural control in patients with CAI is affected by the in-phase mode of the BASYS may provide additional insight into how to restore normal function. Future research should examine if combining the in-phase mode of the BASYS with conventional techniques will boost improvements in dynamic postural control, offering a new approach for balance training after an ankle injury.
CONFLICTS OF INTEREST
The authors have no competing interests to disclose.
FUNDING
No funding was received in relation to this project.
ACKNOWLEDGMENTS
The authors thank all those who participated in the research.