INTRODUCTION
Movement is essential to human life. It is a vital aspect to the overall health and well-being of every human. Good movement quality has been defined as the performance of fundamental movements in a properly balanced and well-coordinated manner.1 On the contrary, poor movement quality has been defined as the inability to complete fundamental movements in accordance with accepted theoretical norms.1 These theoretical norms for movement have been developed by screening and scoring humans.
The original Functional Movement Screen™ (FMS™) has primarily been completed on the athletic population. If athletes or active adults want to potentially reduce a risk factor for injury and potentially improve their performance, then they need to be aware of how they are fundamentally moving. The FMS™ allows athletes, coaches, and clinicians to be aware of the movement strategies, and discern if alterations are needed before providing or progressing an appropriate exercise prescription. This awareness allows the athlete, coach, or clinician to modify exercise prescriptions based on the athlete’s needs. The recommended goal of the FMS™ is to obtain a score of 32 indicating movement competency; however, high level athletes can still score a 1 (indicating inability to perform) or a 2 (alteration/compensation during completion of movement) or demonstrate asymmetrical movements and remain successful. The FMS™ was developed as a screening tool to see if an athlete or active adult has pain or asymmetrical movement patterns. The screen was meant to help decide if the athlete should be protected, corrected, or developed.2
The FMS™ has been utilized by movement professionals to screen an individual’s functional and fundamental movement patterns to produce a quantifiable measure of their movement quality (0, 1, 2, or 3).1 The FMS has helped identify movement quality dysfunction in athletes or active adults that may be at risk of, but not currently experiencing, signs or symptoms of a musculoskeletal injury.3 Although the FMS™ is not intended to make a diagnosis, it has been used to identify and improve movement quality in individuals that are screened.4 The FMS™ has seven separate movement patterns that were specifically designed to place an individual in positions where movement deficits are noticeable if appropriate stability and mobility are not used.5 The seven movement patterns include: the deep squat, the hurdle step, the inline lunge, shoulder mobility, active straight-leg raise, the trunk stability pushup, and rotary stability. A scale from 0-3 has been used to score the seven movement patterns. A 0 indicates the individual has pain during any part of the movement, a 1 indicates the individual cannot perform the movement pattern even with compensations, a 2 indicates the individual can perform the movement but utilizes poor mechanics and compensatory patterns to accomplish the movement, and a 3 indicates that the individual can perform the movement without any compensations according to the established criteria.4
The FMS™ is clinically relevant to athletes and active adults because the scoring allows clinicians to progress the individual appropriately and safely with exercise prescription. If the athlete or active adult scores a 0 on a movement pattern, then they are to be referred to a qualified healthcare provider for further assessment due to the presence of pain. If the athlete or active adult scores a 1 on a movement pattern, then they are to be coached or provided with corrective exercises to improve the movement quality, which may potentially reduce a risk factor for future injury. If the athlete or active adult scores a 2 or 3, then their movement patterns mayb be considered acceptable and there is no need for corrective exercises to be administered.
Past studies on the original FMS™ have found that there was good to excellent interrater and intrarater reliability between the raters. Gribble et al.6 found evidence that was moderate to strong supporting intrarater reliability. Gulgin and Hoogenboom7 found acceptable reliability among four raters (three novices and one expert) that were all certified in FMS™. Leeder et al.8 found good to excellent reliability of the FMS™ when the raters were untrained and were only given instructions on how to score the recorded individuals via a DVD. Teyhen et al.9 had novice examiners go through 20 hours of training regarding the FMS who then demonstrated good to excellent interrater reliability. Shultz et al.10 demonstrated poor interrater reliability with five raters that were trained in FMS™ and one rater that was self-trained. Many other studies continue to demonstrate good to excellent interrater reliability,11–13 however, no study has looked at the new criteria for the FMS™ with the addition of the ankle clearing test and the updated scoring criteria for the rotary stability test.
The FMS™ was updated for two reasons: (1) the ankle clearing test was added because it was difficult to globally screen for ankle mobility deficits and pain, which caused clinicians to miss ankle dorsiflexion restrictions14,15 and (2) the rotary stability test was modified because the original test only discovered about 15% of rotary asymmetries, where the updated test is able to discover about 37% of rotary asymmetries.16 The updated FMS™ appears to improve the validity of the screen as compared to the original FMS™ by screening specifically for dorsiflexion restrictions in the ankle and by discovering rotary asymmetries, which may potentially help an athlete or active adult improve their performance and reduce a risk factor for injury.
It is important to understand whether the updated FMS™ is reliable because it could allow a variety of clinicians to confidently screen the quality of movement of athletes or active adults. If poor movement qualities are observed, then recommendations can be made to improve the movement pattern, potentially reducing a risk factor for future injury risk. Many authors have reported that having a total score of less than 14 on the FMS™ increases the individual’s risk of injury.17–25
Use of FMS™
Most of the research involved in the original FMS™ has been focused on athletes or fit individuals. There has been a lack of research completed on individuals that are older, are not involved in sports, and may have other health complications. Multiple studies have examined if the FMS™ can be used as a diagnostic tool and used as a tool to predict future injury. A study done by Kiesel et al.17 asked the question; “If injuries sustained in professional football could be predicted and prevented by a functional movement screen done in the preseason?” It was found that athletes with a score of 14 or less on the FMS™ had a higher risk for injury. Bardenett et al.,26 found that the screen was better off used as an “assessment of quality” rather than used for diagnostic purposes. Another study by Dorrel et al.27 found that the screen did not provide discriminatory predictive values for future musculoskeletal and overall injury. On the other hand, a study by Bushman et al.28 agreed with the study listed above by Kiesel et al.,17 which said that physically active men who scored lower on their FMS™ (<14) put them at higher risk for future injury. At this time, there is mixed evidence as to whether the FMS™ may or may not be a good predictive tool for future injuries.
Smith et al.29 examined interrater reliability and intrarater reliability for individuals who took a two-hour training course on the original FMS™ and then scored subjects across two assessment sessions. It was found that the interrater reliability was good for both session one and session two (ICC of 0.89 and 0.87, respectively). The intrarater reliability of each individual rater was examined across the sessions, resulting in good reliability as well (ICC range from 0.81-0.91). A systematic review of six studies on the reliability of the original FMS™ found the overall interrater and intrarater reliability to be ICC 0.81.18 Both studies involved researchers that varied in FMS™ experience or only received a short training period before rating the subjects. Past studies have suggested that the original FMS™ intrarater reliability was strong and appeared to strengthen when the individuals had experience using the FMS in addition to clinical experience.26 The purpose of this study was to determine if the updated FMS™ has acceptable interrater reliability, so that various practitioners can utilize it with their patients.
METHODS
Experimental Approach to the Problem
The study was designed to have four raters who had all received the same education, perform the FMS™ to determine interrater reliability. Participants were taken through the FMS™ with standard instructions per FMS™ guidelines. Each rater observed and scored 45 participants based on the scoring criteria created by the FMS™. The study was approved by the Institutional Review Board (IRB) at the University of North Dakota.
Subjects
Participants were recruited from a student cohort in a physical therapy department. The inclusion criteria for this study were current physical therapy students with no reports of a recent injury (recent defined as less than or equal to four weeks prior). The exclusion criteria were any recent injury, an injury that contraindicated complete weight-bearing activities, and a participant’s inability to attend the scheduled videotaping sessions. Recruitment was done through email in which the subjects received an explanation of the nature, purpose, and risks of the study and were asked to volunteer to assist in the research. Fifty-five volunteers were recruited, and out of the 55 volunteers contacted, 10 volunteers declined. Before the FMS™ was completed and videotaped, participants and raters signed an informed consent document approved by the Institutional Review Board at the University of North Dakota.
Raters
The four student raters were halfway through their second year in the Doctor of Physical Therapy Program at the University. All the raters had received the same amount of prior learning and education in the field of physical therapy. For the FMS™ screen specifically, each rater had received a brief one-hour presentation on how the FMS™ was conducted and used, four months prior to testing. Two weeks before testing, the raters were presented with a two-hour lecture on the FMS™ in a class. Each rater practiced completing and scoring the FMS™ three times, one week before videotaping the participants. Following the screening of the participants, the raters attended a 1.5-hour FMS™ review session given by a licensed physical therapist who was certified in the FMS™. The raters were not certified in FMS at any time during the study. To be certified in FMS™, it takes approximately eight hours to get through the content. The rater training for this study was based on current classes in the PT curriculum at the University and a review of material to allow for accuracy in scoring the participants.
Procedure
Two experts, both licensed physical therapists, one of whom was certified in FMS™, conducted the FMS™ screening for this study. No warmup was allowed for the subjects before the screening. Next, tibial tuberosity height (from the ground to the top center of the tibial tuberosity) and hand length (from the distal wrist crease to the end of the longest digit) were measured using the FMS™ equipment per standard FMS™ instructions. Tibial height and hand length measurements were used for each participant during the hurdle step, inline lunge, and shoulder mobility movement patterns. Each participant then underwent one FMS™ testing session while being recorded on video, which lasted approximately 15 minutes. For reliability purposes, word for word instructions were read to the participants on how to complete the seven movement patterns and four clearing tests of the FMS™ (Appendix A), in addition to demonstrations of each movement pattern. If the subject needed more clarification, instructions or demonstrations were repeated, but no further directions were given. Instructions were provided immediately before each individual movement. After demonstrative and verbal instructions were given, the participants were allowed three attempts to complete the movement pattern per FMS™ instructions, with the best score recorded. After each movement, the participant was asked if any pain was associated with the movement. During each movement, the participants were video recorded from both the sagittal and frontal planes in a closed environment. Once the video recordings were completed, the four raters then individually observed and scored the FMS™ on each recorded participant. The videos were stored securely labeled only with a number (i.e. - Participant 1). The four raters each completed the scoring from the video recordings in the same environment each time, and in the absence of any outside distractions.
Statistical Analyses
The scores for each participant were put into Statistical Package for Social Sciences (SPSS) and reliability analysis statistics were run for each movement. Descriptive statistics were calculated as mean values with standard deviation for normal interval data. Intraclass Correlation Coefficients (ICC’s) were calculated to determine the interrater reliability of each individual exercise component of the FMS™ and the participant’s overall FMS™ score. Interrater reliability was defined as poor for an ICC below 0.50, moderate for 0.50–0.75, good for 0.75-0.90, and excellent for 0.90 or higher.30
RESULTS
Forty-five individuals participated (male=14 and female=31). The overall ICC for the total score was 0.95 (95% CI: 0.93, 0.97), demonstrating excellent interrater reliability between raters (Table 1).
As far as new criteria on the FMS™ regarding the clearing tests, the ankle mobility clearing test for the right inline lunge was ICC 0.76 (good), while the left side was ICC 0.63 (moderate). These tests both show good and moderate interrater reliability, respectively, and are shown in Table 2. All other clearing tests suggest good to excellent interrater reliability.
Table 3 displays the raw scores of the individual movement patterns. Examination of the individual movement patterns of the FMS™ showed rotary stability as the most reliable ICC 0.96 (95% CI: 0.93, 0.97), whereas the least reliable was deep squat ICC = 0.78 (95% CI: 0.66–0.87). The deep squat was still considered to have good interrater reliability.
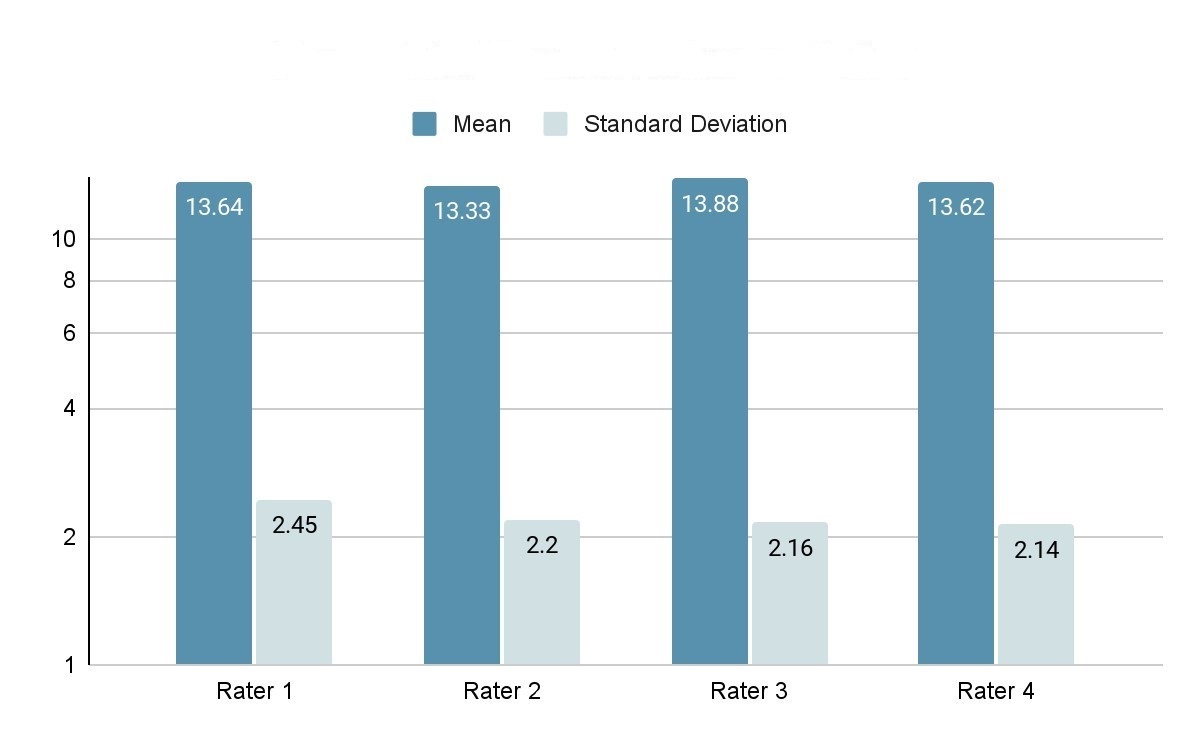
Mean total scores are shown in Figure 1. The results suggested that each rater’s score was highly correlated with one another. The ICC of the final score of each movement pattern was above 0.90, except for the deep squat. This is in the “excellent” category for interrater reliability.

DISCUSSION
The purpose of this study was to determine if the updated FMS ™has good to excellent interrater reliability, so that various practitioners can apply it to their patients. It is anticipated that the updated FMSv will have good to excellent interrater reliability and its application may reduce a risk factor for future injury and potentially improve performance of athletes and active adults. Previous literature has examined interrater reliability using videotaping and multiple raters, but these studies were prior to the additions and modifications to the FMS™ and warranted further study. To the best of the authors’ knowledge, this study is the first study to assess interrater reliability following the addition of the ankle clearing test and modifications to the rotary stability scoring criteria.
Past studies6–9,11–13 have all demonstrated good to excellent interrater reliability of the original FMS. In the current study, the updated FMSv continues to demonstrate good to excellent interrater reliability. The new criteria for the FMS™ were found to show good to excellent interrater reliability, except for the left ankle clearing mobility test, which had a moderate agreement among raters. These results suggest that the new criteria are reliable between raters. There was a large difference between the right and left ankle mobility clearing test (ICC = R: 0.76, L: 0.63), indicating that an outside variable may have caused this difference in reliability. This may be due to viewing difficulties when participants wore pants rather than shorts, when participants did not hold the position long enough to view the end position, and when participants let the heel lift off the ground. Future studies should be aware of these factors when completing the mobility clearing test on the ankle.
There were limitations related to rating the participants. The first limitation included a non-standard distance that the participant was from the video recording making some videos easier to see than others. The second limitation included the rater’s choice of an area that was non-distracting to observe and score the participants. This location was supposed to be used each time the rater observed and scored a participant; however, the only way that this was monitored was through verbal confirmation. Lastly, all the participants were in their 20s or 30s, healthy, active, and in graduate school. Future studies could examine various ages of participants and include participants that have comorbidities.
CONCLUSION
The results of this study indicate that four novice raters who were minimally but adequately (4.5 hours of training and three practice attempts) trained can reliably score individuals on the updated FMS™. A reliable screening tool allows physical therapists to observe and intervene with their patients, clients, or active adults quickly, so that they can be proactive and potentially reduce the likelihood of future injury and/or pain.
Disclosures
The authors of this study express that there are no conflicts of interest. The results shown are not endorsed or funded by the authors of the National Strength and Conditioning Association or any outside source.