INTRODUCTION
It has been reported that 19% - 79% of runners experience running-related injuries, and up to 40 million Americans experience running injuries each year.1 Although running has many benefits, such as reduced risks for cardiovascular disease and cancer mortality,2 it is associated with various musculoskeletal injuries, including medial tibial stress syndrome, Achilles tendinopathy, plantar fasciitis, and patellofemoral pain.3 The risk factors associated with sustaining running-related injuries include abnormal running mechanics, prior running injury, higher weekly mileage, and increased frequency of running.1,4 Given that running in faulty forms are associated with musculoskeletal injuries,1 implementation of running gait analysis in orthopedic/sports physical therapy settings has been suggested to help identify abnormal mechanics in runners and combat the occurrence of these injuries.
Two-dimensional (2D) motion analysis is an affordable, time-efficient method for analyzing running mechanics in runners.5–7 For runners, 2D motion analysis is comparable to 3D motion analysis in quantifying sagittal plane kinematics of the hip, knee, and ankle during running.6 2D analysis has also been shown to provide reliable results for assessing running gait kinematics.1,8–10 Identification of gait events and common kinematic variables, including rearfoot position, foot-strike pattern, tibial inclination angle, knee flexion angle, knee separation, and forward trunk lean, were found to be highly reproducible.1 Excellent intra- and inter-tester reliability was demonstrated with contralateral pelvic drop and hip adduction angles in the frontal plane,10 as well as with sagittal plane measures, regardless of clinician experience.9 A recent systematic review concluded that 2D video analysis is a reliable method for assessing foot strike pattern and quantifying step rate.8 The information obtained from these 2D running gait analyses can be utilized by clinicians to inform their plan of care with the goal of improving a patient’s running mechanics to decrease their risk of injury.5
Despite the benefits of using 2D motion analysis, current use of video-based motion analysis among orthopedic physical therapists is not prevalent: less than 50% of orthopedic physical therapists use it in their routine caseload.11 Therefore, there is a need to investigate the process and effects of implementing 2D running gait analysis in clinical physical therapy settings. Therefore, the purpose of this study was to investigate clinician-perceived effectiveness, adherence, and barriers of using a 2D running gait analysis protocol for patients with running-related injuries. An additional aim of this study was to evaluate the value of implementing 2D running gait analysis by examining the associations between the plan of care, usefulness of routine use, clinicians’ satisfaction, patient-perceived benefit, time spent on the 2D motion analysis, and/or clinician perceived usefulness for making treatment plan decisions.
METHODS
2D Motion Analysis Methods
The physical therapists that participated in this study were instructed to use the specific setup and procedures below. CoachNow (Shotzoom Software LLC, Tempe, Arizona, https://coachnow.io), a free, 2D motion analysis smartphone application that supports video recording and analysis with slow motion playback and dynamic annotation was used to analyze the videos collected from a smartphone. A similar smartphone application (Coach’s Eye), which has been retired, has been shown to be a valid and reliable tool for analyzing various running gait kinematics.12 Specifically, Mousavi and colleagues showed excellent intra- and inter-rater reliability with the use of Coach’s Eye during treadmill running (ICCs ranged from 0.87-0.99). When compared to 3D motion analysis, they reported fair to excellent validity for measuring hip, knee, ankle, and foot kinematics, with ICCs ranging from 0.51 to 0.79.12 The sagittal view was taken with the camera placed two meters from the side of the treadmill, while the posterior view was taken with the camera 1.5 meters from the back of the treadmill.12 For both views, the camera was one meter off the ground, horizontally secured into the tripod, and orthogonally positioned relative to the plane of interest in order to reduce skewing of angles during analysis.
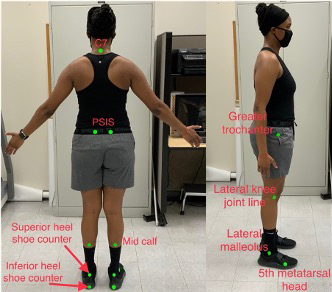
Standardized patient setup included patients being asked to wear running shorts, a tank top or sports bra for females and no shirt for males in order to facilitate optimal marker placement and observation of key landmarks. The markers used were round, 1-inch diameter, fluorescent 2D stickers placed at the C7 spinous process, posterior superior iliac spines, greater trochanters, lateral knee joint lines, knee joint center, lateral malleoli, midpoints of the calf, superior and inferior portions of the heel shoe counter, and the fifth metatarsal heads (Figure 1).

Patients were instructed to warm up on the treadmill at a self-selected speed for six to ten minutes at 0% incline.4 After the warm-up period, two 25-second videos were recorded in succession for each view.
Once recording was complete, each video was uploaded and analyzed with CoachNow. Analysis included viewing the footage in slow motion, pausing and using a scroll bar to identify precise gait events, and annotating still frame images to better visualize joint and body positions. Gait events to be identified were initial contact, defined as the first contact of the shoe on the treadmill belt, and midstance, defined as the instance the swing knee was adjacent to the stance knee.1 In addition, a running gait checklist that researchers adapted from the work of Pipkin et al.1 was provided to assess the alignment during the initial contact of the sagittal plane and midstance of the frontal and sagittal planes (Table 1 and Appendix 1).
RE-AIM Model for Assessing the Implementation of 2D Running Analysis
The process of implementing 2D running gait analysis into physical therapy clinics was assessed using the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) framework.13–17 The RE-AIM model provides a comprehensive evaluation framework to improve public health and community-based interventions by facilitating the translation of scientific advances into practice.18,19 Specifically, Reach is defined as the extent to which implementation reached the targeted population, measured by the percentage of outpatient orthopedic clinics deemed eligible compared to those approached that responded to the authors’ inquiry. Adoption is defined as the extent to which implementation is adopted in the clinical setting and by providers, measured by the percentage of orthopedic clinics willing to participate compared to those deemed eligible. Effectiveness is defined as the impact of an intervention on important outcomes by analyzing how often therapists used information gained from running analysis, and perceived utility of using the protocol. Implementation is defined as the extent to which the intervention is implemented as intended by analyzing therapists’ adherence to the protocol. Maintenance is defined as the sustainability of implementation over time by analyzing therapists’ persistence to using the protocol.
Surveys to Assess the RE-AIM model
To assess the five dimensions of RE-AIM, the researchers created four surveys (i.e., baseline survey, effectiveness survey, implementation survey, and maintenance survey) using Qualtrics XM (Qualtrics Software Company, Provo, Utah). All surveys were validated by a panel of five experts. Face and content validity of the surveys were determined by a panel of two physical therapy educators who specialize in orthopedics, two physical therapists with specialty certifications in running analysis, and one physical therapist who is a generalist. These experts provided a breadth of knowledge related to video gait analysis and the practicality of using video analysis in a clinic setting. They were asked to assess the overall face and content validity by examining the language used and relevance of each item in the questionnaire. Upon review of each survey question, each item was deemed valid by all experts, and no changes were made to the surveys.
The baseline survey gathered information about clinician specialization, such as being a clinic or regional director, prior running gait analysis training, current perceptions of running gait analysis to assist with treatment of patients, overall interest in the study, if they would be participating in the study, and reasons for non-participation. The baseline survey allowed the team to assess “Reach” and “Adoption” rates of implementation.
For the effectiveness survey, a 5-point Likert scale was used for the questions, where 1 represented a response of “not at all” and 5 a response of “very much”. Specifically, this survey asked for a rating of difficulty to conduct the protocol, if the protocol set up was reasonable, if the running gait checklist was useful for analyzing running gait patterns, if the protocol was worth routine use, if they felt the patients saw the benefit of using this analysis in their evaluation, and if implementing the protocol affected their overall satisfaction with treating running patients. Additional questions asked for a rating and an explanation for each answer. The questions included in this survey were as follows: “Is the methodology reasonable and appropriate? Is the protocol helpful in making decisions in treatment plans? Does the protocol influence your plan of care?”
The implementation survey contained questions that assessed the frequency in which the physical therapists performed the protocol and to what extent they accurately followed the protocol. These included a numerical value for number of times conducting the protocol in the last month and average time in minutes conducting each individual running gait analysis. A yes or no answer was used for questions asking if the amount of time spent performing the analysis was reasonable, if each runner warmed up for the appropriate time, if all videos were taken for at least 25 seconds, if the CoachNow application was used to analyze video footage for each runner, and if the running gait checklist was used to interpret the findings for each runner. Additional yes and no questions with an explanation box if the participant answered “no” were used for the following questions: “Was the protocol performed on all appropriate patients? Were the stickers used on each landmark for each runner? Were all videos taken from the specified setup criteria? Was CoachNow used as instructed? Was the running gait checklist used as instructed?”
The maintenance survey assessed how well the physical therapists maintained the use of the 2D running analysis protocol. Questions asked in this survey were: “Have you maintained use of the protocol? Have any adaptations been made to the protocol? Will you continue to use the protocol in the future? Do you have any further input or suggestions about the protocol?”
Procedure
The baseline survey was sent to 30 outpatient physical therapy clinics that are affiliated with the University of Nevada, Las Vegas, to assess interest and eligibility in study participation. To be eligible for the study, participating clinics did not have a current 2D running gait analysis protocol in place, had to have a licensed physical therapist and treadmill available within the facility, and had to be currently treating at least one patient with a running-related injury. Once the participating clinics were identified, researchers visited each clinic to train participating physical therapists in performing the 2D running gait analysis using aforementioned methods. The physical therapists were asked to perform this protocol at initial evaluations and re-evaluations on their appropriately designated patients, defined as any patient with a running-related injury that was willing and deemed safe by the evaluating therapist to perform treadmill running for gait analysis. The therapists were also advised to use their findings to help inform their treatment plan.
The effectiveness and implementation surveys were sent to all participating physical therapists after two months of participating in the study and contained questions pertaining to the protocol taught to therapists. The maintenance survey was completed four months after the effectiveness and implementation surveys were sent. All activities in this study were approved by the review board of University of Nevada, Las Vegas (IRB 1712677-5). Informed consent was obtained for all subjects and participating facilities.
Statistical Analysis
The data collected from the four surveys were de-identified for confidentiality. Reach and Adoption were evaluated using descriptive statistics through the baseline survey. Effectiveness and Implementation were assessed using descriptive statistics and qualitative analysis of information gathered from their respective surveys. Maintenance was evaluated using descriptive and qualitative statistics from the maintenance survey. For descriptive statistics, we reported available mean, standard deviation, frequency (percentage), and range. For quantitative analyses, Spearman’s rho correlation analysis (one-tailed, significance level=0.05) was also conducted, where correlation strength (r) was adapted based off general guidelines and defined as weak (r < 0.4), moderate (0.4 < r < 0.7), and strong (r > 0.7) for this study.20 Quantitative data was analyzed in SPSS statistical package (SPSS version 27.0, IBM Corp., NY, USA), while qualitative data was assessed using ATLAS.ti.
RESULTS
Reach and Adoption
Of the 30 clinics contacted, 15 clinics responded to the baseline survey. Twelve of these 15 clinics met the eligibility criteria for this study, giving a reach value of 80%. The remaining three clinics were not eligible to participate with two of them stating they did not have the correct patient population, and one reporting having an existing running gait analysis protocol in place. Of the 12 eligible clinics, 10 of them participated in the study, giving an adoption value of 83%. The two clinics that chose not to participate indicated time constraints and lack of cases to support effective use of the protocol as reasons for non-participation. Ultimately, 12 physical therapists from 10 different clinics participated in this study (Table 2). The age range of participating physical therapists was 28-57 years old, with a mean age of 41 years old. Eight of the 12 physical therapists were clinical or regional directors. Half of the therapists reported having prior standardized training with running gait analysis, while the other half had no prior training (Table 2).
Common reasons for participation included gaining knowledge and improving clinical skills in order to provide better treatment to runner patients and contributing to research for the advancement of the physical therapy profession. Five therapists’ initial perception of running gait analysis was that “it can be useful if time permits and when used with the appropriate population”. Four therapists acknowledged that running gait analysis would be most beneficial when used by trained and well-versed clinicians in running mechanics and that running analysis should not be used in isolation, but rather as part of a full patient assessment. One therapist stated that running gait analysis was useful for breaking down phases of gait, identifying biomechanical faults and possible contributing factors towards injury, tracking progress, and when used in conjunction with patient education.
Effectiveness
Table 3 details the effectiveness survey results regarding how the 12 included physical therapists ranked each survey question. The four questions that received the highest rating were “Is the protocol easy to conduct?”, “Is the methodology reasonable and appropriate?” ,“Is the provided Running Gait Checklist useful for analyzing running gait patterns?”, and "Do the patients see the benefit of using this in their evaluation?", with a score ranging between 4.0 and 4.6. Two questions received somewhat ambivalent/neutral ratings, including “How useful was the protocol in helping you make decisions about your treatment plans?” and “Is the level of usefulness enough to make the protocol worthy of routine use?”, with a score of 3.2 and 3.0, respectively. The remaining three questions scored intermediately between 3.7 and 3.8, including “Are the setup criteria reasonable?”, “Does using 2D running gait analysis influence your plan of care for patients?”, and “How has implementation of the protocol affected your overall satisfaction with the treatment you provide your running patients?”. A significant moderate positive correlation was found between the rating of the protocol’s influence on plan of care and the rating of usefulness of routine use (r=.516, p=.043). The rating of clinicians’ satisfaction of implementing the 2D motion analysis in the provided treatment demonstrated positive moderate correlations with the rating of the protocol’s influence on plan of care (r=.509, p=.045), and with the rating of patient perceived benefit of using the protocol (r=.524, p=.040).
Implementation
During the first month of implementation, six therapists conducted a single running analysis, two therapists conducted two analyses, three therapists conducted three, and one therapist conducted four analyses, for a total of 23 analyses (mean = 2 analyses). All therapists reported performing the protocol on every appropriate runner with a running-related injury except for one therapist who was unable to conduct the protocol on one runner due to complications with setup in the clinic at the time. Therefore, therapists performed the protocol on 23 of the 24 appropriate runners, a rate of 96%. The average time therapists spent performing each protocol was 32 minutes (range = 10-75 minutes), with 50% of the therapists spending between 25-30 minutes on each running analysis. 75% of the therapists felt the time spent conducting each analysis was reasonable, including those who spent 45 and 75 minutes on each analysis. The remaining three therapists who felt the time spent was unreasonable reported conduction times ranging from 25-60 minutes. A significantly moderately positive correlation was found between average amount of time spent conducting protocol and the rating of clinician perceived usefulness for making treatment plan decisions (r=.663, p=.009).
As shown in Table 4, 83% of therapists reported placing markers on every designated landmark for each runner. Of the remaining two therapists, one reported placing markers for the frontal, but not sagittal view as their clinic setup did not allow them to obtain a sagittal view. Another therapist reported not needing markers at all. The majority of runners who had a running gait analysis performed, warmed up for the designated time of 6-10 minutes, an adherence rate of 96%. Therapists were asked whether all videos were taken from the specified distance, height and angles provided in the protocol, eight therapists (67%) answered yes. The four therapists who answered “no” gave responses related to setup and time efficiency as reasons for making modifications. Specific issues with setup involved clinic layout not allowing for a sagittal view, treadmill handlebars obstructing the sagittal view, and differences in magnification between devices. 92% of therapists reported recording all videos for at least 25 seconds, and 100% of therapists used either the Coach’s Eye application or CoachNow application to analyze video footage for each runner. Eleven of the 12 therapists used the applications as instructed while one therapist did not, and instead used the application’s line tool to draw a plumbline from which they could emphasize angles, alignment, and contact points. All therapists used the running gait checklist to interpret findings for each runner, with 11 of 12 therapists using the checklist in the manner that was instructed. One therapist reported skipping through some of the checklist for efficiency.
Maintenance
Of the 12 clinicians completing the study (Table 5), six therapists (50%) reported continuing to use the running gait analysis protocol, while six therapists (50%) answered “no” to continuing use. Comments from the group of clinicians answering “yes” about why they continued to use the protocol included two therapists reporting general interest in using the analysis to analyze patient’s running gait, two therapists reporting the protocol being useful for patient education, and one therapist feeling the protocol was quick to set up and easy to use. Reasons reported by the group answering “no” to continuing protocol use included five therapists reporting not having adequate case load to continue use, one therapist reporting time restraints, and one therapist reporting clinic set up not allowing adequate use of protocol. Overall, only one out of 12 therapists (8%) reported making adaptations to the protocol. The adaptation reported was “did not take every measurement to shorten the protocol to focus on specific patient goals”.
When asked “Will you continue to use the protocol in the future?”, seven therapists answered “Probably yes”, four answered “Might or might not”, and one answered “Probably not”. Additional comments related to the protocol were: 1) the protocol would be useful in a cash pay setting rather than a busy outpatient setting, 2) the protocol is useful if not limited by time restraints, 3) having more appropriate patient populations would allow for more use, and 4) using the stickers can be cumbersome to put on and have limitations in their use.
DISCUSSION
Previous research has shown that more than 50% of surveyed orthopedic physical therapists do not use video-based motion analysis in clinical practice.10,11 To understand the actual implementation of 2D running analysis and barriers of implementation in clinical physical therapy setting, we aimed to examine the clinician-perceived notions of implementing a running gait analysis protocol into their practice via a RE-AIM model.
The RE-AIM framework used in this study allowed us to understand the details of the implementation process. The “Reach” and “Adoption” rates in the beginning of this study were 80% and 83%, respectively, suggesting that we were able to reach and initiate the adoption of the 2D running gait analysis in the majority of outpatient orthopedic clinics. However, as 15 clinics did not respond to the proviced survey, the reach and adoption rates observed in this study may have been different if those clinics responded to the baseline survey.
With respect to the effectiveness of implementing the 2D running analyses, the majority of the clinicians that participated in this study valued having a protocol with a checklist in which they could quantitatively analyze their patient’s running gait pattern with a reported mean score of 4.6 on a five-point Likert scale. Additionally, most therapists reported that the protocol was easy to conduct, the methodology was reasonable and appropriate, and the patients saw the benefits of using the protocol in their evaluation. However, the questions about the level of usefulness for making the protocol worthy of routine use and for helping clinicians make decisions about the treatment plan received neutral rating (around 3.0). This may be attributed to time constraint and patient’s competing needs in an outpatient setting. Of the clinicians who chose to elaborate on why they felt that the protocol was or was not worthy of routine use, all of them stated that time was the significant factor in why it might not be. Interestingly, a moderately positive correlation was found between the amount of time spent conducting the protocol and clinician perceived usefulness in developing a treatment plan, suggesting that the increased amount of time taken to properly conduct the protocol could benefit therapists’ in developing individualized treatments for their patients. One possible strategy to alleviate the time required for administering the 2D motion analysis is to have other clinic personnel assist with the camera setup and marker placements to shorten the amount of time taken to perform the entire protocol.
One potential barrier to implementing this protocol expressed by clinicians was not having appropriate clinic setup to accommodate performing this protocol. One clinician stated that their clinic space did not allow for sagittal views, one reported having a treadmill with handlebars that obstructed the field of view, and one clinician stated that different [video recording] devices display different magnification settings, which may require clinicians to adjust the distance to the treadmill that videos are taken from in order to get all markers within view.
It is also important to acknowledge that some clinicians who might attempt to implement this protocol may not have access to video technology or access to the application used to analyze running gait in this study, which could limit their ability to conduct this analysis. Although all clinics were deemed eligible prior to implementation, change in clinic setup or in clinician video devices could have created barriers to using the running analysis. Having a consistent manner to record videos and perform analysis is essential, meaning clinicians will need to assess their own setups to decide if they are able to perform the analysis.
When asked if the protocol influenced their plan of care, clinicians most frequently stated that it helped to provide patient education and to design treatment plans based on their patient’s gait abnormalities. Importantly, associations were found between the protocol’s influence on plan of care and usefulness of routine use, and between clinicians’ satisfaction of implementing the 2D motion analysis and the protocol’s influence on plan of care/patient perceived benefit. Multiple clinicians also expressed the importance of this protocol being used in conjunction with other examination strategies, rather than using this protocol as a standalone assessment. Further research will need to be conducted to assess what strategies would best be incorporated with performing a running gait analysis. Since visual feedback is already a common use of video-based motion analysis among clinicians that use cameras to analyze their patient’s movement,11 the integration of patient education along with visual feedback when using this protocol has the potential to be a significant benefit of using this 2D running gait analysis.
Half of the clinicians involved in this study reported not continuing protocol use after the six-month maintenance survey. This rate is similar to that of a larger-scale survey study that assessed the prevalence of using 2D motion analysis in orthopedic physical therapy clinics.11 However, the majority of clinicians reported that they would or probably would use the protocol in the future. This shows that even though clinicians did not remain consistent after six months, they are open to using it again when needed. Clinicians expressed that the main hinderances to continued use are not having a sufficient patient caseload to continue use and time restraints due to their clinic setting. No clinicians reported discontinuing use of the protocol due to any specific protocol reasons or feeling that the protocol was not useful, leading the researchers of this study to believe that a much higher retention rate would have been plausible if clinicians worked with more patients that were runners or had more time to evaluate each patient. Also, only minimal reports of changes or suggestions were made by clinicians about the protocol, demonstrating that the protocol itself may not be the reason for the low retention rate.
Lastly, while many clinicians stated that the protocol was useful in designing their treatment plans, it is unclear if the change in treatment resulted in improved function as patient outcomes were not assessed. Nevertheless, these results suggest using this protocol in a clinical setting with an appropriate patient population, sufficient amount of time to evaluate each patient, and proper clinic set-up may provide clinicians an effective tool to help guide patient evaluations and design treatment plans.
The study has several limitations. First, given that this study was only conducted in the Las Vegas area, the findings may not be generalizable to other areas. Another limitation of the current study is that patient outcomes or perspectives were not assessed. This study focused solely on the clinicians’ views of implementing 2D running gait analysis, but evaluating patient outcomes could provide useful information and should be considered for future research. A third limitation in the current study was that many of the therapists had high caseloads. Time constraints and inadequate patient population were commonly reported barriers in this study; thus, the results could potentially be different if the study was done with different clinician populations.
CONCLUSION
The results of this study provide evidence that 2D running gait analysis is a potentially valuable intervention that can be utilized by outpatient physical therapy clinicians to assist with evaluating injured running patients and devising treatment plans. Clinicians that participated in this study expressed a perceived benefit of implementing a running gait analysis protocol with common themes of ease of use, being a useful adjunct to evaluating a patient, and increased satisfaction with treating injured runners. Potential barriers presented in this study included clinicians not having appropriate clinic setup, being restricted by time constraints, and not having adequate patient populations. The use of a 2D running gait analysis protocol in outpatient physical therapy settings may be improved by eliminating the barriers identified in this study.
Disclosures
The authors report no conflicts of interest.