


INTRODUCTION
The lower trapezius (LT) muscle plays a critical role in stabilizing the scapula while it assists in the upward rotation of the scapula as part of a force couple. Of particular importance is the activity of the LT muscle which serves to maintain the width of the subacromial space during arm elevation through posterior tilting of the scapula.1,2 Conversely, altered activity ratio of the upper trapezius (UT) and LT muscle, such as hyperactivity of the UT muscle, can lead to scapular dyskinesis, which may be associated with symptomatic shoulders.1,2 For instance, patients with subacromial pain syndrome showed significantly higher ratios of UT to LT muscle activity in both the ascending and descending phase of arm elevation in the scapular plane, compared with asymptomatic individuals.3 A college baseball pitcher with shoulder symptoms after arthroscopic labral surgery abruptly increased the ratio of UT to LT muscle activity on the throwing arm during the weighted scapular dyskinesis test, compared with the non-throwing arm side.4
For healthy college and professional pitchers, the highest LT muscle activity has been reported during the acceleration and deceleration phases of the throwing motion.5 These findings can be associated with one of thrower’s adaptations where LT muscle activity was significantly greater on their dominant side than their nondominant side in both elevation and descent movements, and UT muscle activity was significantly less on their dominant side than their nondominant side.6 Consequently, the ratio of UT to LT muscle activity can be monitored not only for identification of a factor contributing to symptomatic shoulders, but also to provide objective guidance for shoulder exercise progression especially for overhead athletes.7,8
Several previous studies have investigated UT and LT muscle electromyography (EMG) activities in a variety of exercises and postural positions.9–15 Cools et al11 found of the 12 common shoulder rehabilitation exercises, prone shoulder abduction, side-lying forward flexion, and prone horizontal abduction with external rotation (ER), activated the LT muscle up to 80% maximal voluntary isometric contraction (MVIC) while minimizing UT muscle activity to less than 50% MVIC. The UT/LT ratio in the prone horizontal abduction (HABD) with ER exercise was also confirmed by a recent study, which was less than 0.4.9 Additional studies suggest that the prone horizontal abduction exercise at 120° of shoulder abduction effectively activates the LT muscle due to the alignment of the LT muscle fibers.16,17 However, clinicians need to be aware of prone horizontal abduction exercises with the shoulder abducted to 120° or even 90° may increase UT muscle activity to more than 70% MVIC when the scapula is retracted,18 which is not desired to improve scapular force coupling. In contrast, the prone horizontal abduction exercise can minimize UT muscle activity in the scapular plane without scapular retraction, leading to the UT/LT ratio less than 0.9.13 Thus, scapular position needs to be considered during prone abduction exercises to minimize UT muscle activity while emphasizing LT muscle activity.
Exercise intensity is another important consideration during shoulder exercises because it may affect glenohumeral external rotator muscle activity.19,20 LT activity has been correlated with external rotator muscle activity during both shoulder and scapular exercises while UT muscle activity has been correlated with middle deltoid (MD) muscle activity in the coronal plane.15,21,22 Furthermore, the hyperactivity of the MD can cause superior migration of the humeral head, leading to a decrease in subacromial space width especially during shoulder abduction.19,23 Therefore, exercise intensity must be controlled during the performance of shoulder rehabilitation exercise from the perspective of deltoid muscle activity especially for overhead athletes who need to improve scapular muscle balance ratios.5,13–15,17
Few studies have investigated LT muscle activity with respect to scapular protraction and retraction during side-lying shoulder abduction exercise, in which the patient is required to stabilize glenohumeral joint (GHJ) and the straight arm against gravity. Therefore, the purpose of this study was to investigate the electromyographic activity of the LT and other relevant muscles during scapular and shoulder activities in the side-lying position.
The authors of this study hypothesized that the side-lying position with the shoulder abducted to 90° with the scapula retracted would minimize MD activity, whereas the same arm position with scapular protraction would increase MD activity.
METHODS
Participants
Collegiate baseball players were recruited for the purpose of this study. This study obtained institutional review board approval prior to the start of study. All participants read and signed the informed consent confirming their voluntary participation. All subjects were asymptomatic, competitive baseball players without neurologic or physiologic deficits in the upper body according to the completion of a preliminary screening questionnaire. All tests were conducted in the Kinesiology Laboratory at San Jose State University.
Procedures
EMG outputs of the lower trapezius (LT), upper trapezius (UT), infraspinatus (IS), posterior deltoid (PD), anterior deltoid (AD), and serratus anterior (SA) on the dominant side were collected. Bipolar surface silver (Ag) EMG electrodes with a bar length of 10mm, width of 1mm, and a distance of 1cm between active recording sites (Delsys Bagnoli-8, Delsys inc, Natick, MA) were used. Electrodes were placed on the center of the muscle belly in line with the muscle fibers for the specific manual muscle test (MMT). The electrode for the LT was placed obliquely between the intersection of the scapular spine and the scapular inferior angle outside the medial border at the level of seventh thoracic spine.24,25 For the IS muscle, the electrode was placed 4 cm inferior and parallel to the scapular spine over the infrascapular fossa.19 For the PD muscle, the electrode was placed in an oblique direction parallel to the muscle fibers of the deltoid muscles at the lateral border of the scapular spine19,24; while the electrode was placed halfway between the tip of acromion and the deltoid tubercle for the MD muscle.19 For the SA muscle, the electrode was placed below the axilla between the latissimus dorsi and pectoralis major at the level of the scapular inferior angle,24,25 while the electrode was placed halfway between the C7 spinous process and the acromion process for the UT muscle.24,25
Once the electrodes were secured, all the subjects performed a 4-second maximum voluntary isometric contraction (MVIC) after ramp-up contraction for each muscle using the MMT procedures for normalization of EMG data. The manual pressure was applied by the same examiner for all testing positions to determine each of the MVICs. For the MVICs of UT and MD muscles, the subjects resisted downward pressure applied on the arm with the shoulder abducted to 90° with the elbow flexed in the standing position.24,25 For the MVICs of LT and PD muscles, the subjects abducted their arm to 90° with the shoulder horizontally abducted in the prone position.24 The subjects resisted downward pressure applied on the distal portion of the forearm in the coronal plane while they lifted the arm barely off the table. For the MVIC of the IS muscle, the subjects resisted manual pressure applied toward internal rotation of the shoulder with the elbow flexed to 90° and the shoulder adducted with a towel held under the arm in the seated position.19 For the MVIC of the SA muscle the subjects protracted the scapula with the shoulder flexed to 90° and the elbow straight in the supine position while resisting manual pressure applied toward retraction of the scapula or down the arm, known as the “supine serratus punch.” The amount of maximum force (N) was determined with a handheld dynamometer (MicroFET, Hoggan Scientific, LLC, Salt Lake City, UT) for each subject prior to performance of the intervention exercises simultaneously when the examiner measured the MVICs of LT and IS muscle activity during the MMT.
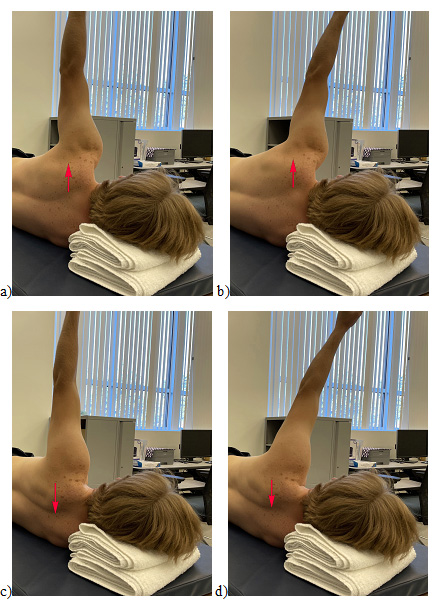
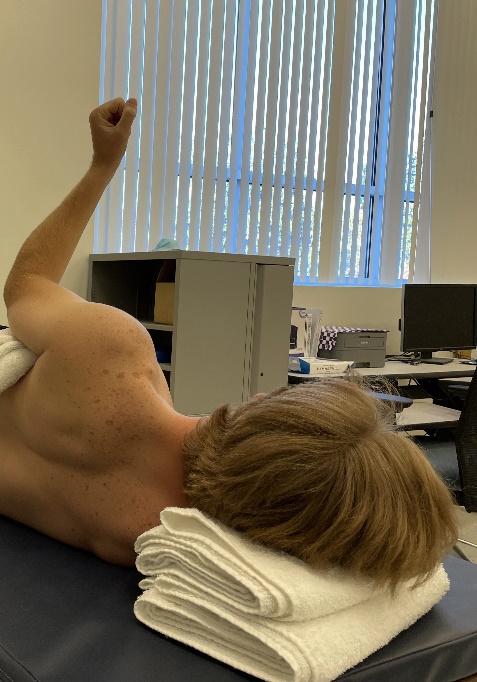
All the subjects performed isometric contraction exercises at 90° of shoulder abduction with the elbow straight in a side-lying position for EMG data collection with two different scapula positions: protraction (PRO) and retraction (RET), and two different HABD positions: 0° horizontally adducted from the coronal plane (NEUT) and 15° horizontally abducted from the coronal plane (HADD). The subjects were asked to extend the arm as much as possible for the PRO testing condition while for the RET testing condition the subjects were asked to pull their scapula down toward their spine. The subjects were asked to minimize any sway of the arm against gravity in the NEUT position, while for the HADD position, the subjects were asked to hold the arm 15° inward from the NEUT position (Figure 1). Finally, all subjects performed the supine serratus punch and side-lying external rotation (ER) of the GHJ in shoulder adduction with a towel under the arm at 90° of shoulder ER or with as much ER as possible (Figure 2).


All of the subjects were asked to perform the isometric exercises under two kinds of external loads: a 9.1 kg (20 lb) dumbbell and 40% of the corresponding MVIC discerned during the MMT. The amount of external weight (9.1 kg) was determined from clinical practices in which overhead athletes were often instructed to specifically activate the SA muscle in supine as if performing scapular punch exercise. The amount of external load (40% MMT) was selected based on the protocol of the previous studies.19–22 For 40% MMT, the subjects were asked to match the external load pressure given just above the posterior distal portion of the forearm as a manual isometric resistance. The direction of resistance application with the handheld dynamometer was in the direction of HADD. Each subject performed the isometric resistance exercises in random order for three trials in each of the four positions (NEUT-PRO, NEUT-RET, HADD-PRO, and HADD-RET). The subjects held each of the arm positions for 10 seconds in each of the two different external loads. Additionally, the subjects performed the supine serratus punch with the 9.1 kg dumbbell and side-lying ER exercise with 40% MMT for 10 seconds for three trials each. The subjects had a10-second rest period after each of the trials while a 30-second rest period was given between different arm positions to minimize the effect of fatigue. The thumb on the tested side was pointing toward the head for all the procedures.
Data Analysis
The EMG electrodes were pre-amplified (X 10) and routed through the EMG mainframe, which further amplified (X 100), and band-pass filtered (20–450 Hz) the signals. The EMG activities were then collected using a data collection program (MP 150 Data Acquisition System; Biopac System, Inc, Goleta, CA) with a sample rate of 1000 Hz; all data were recorded and stored in a computer for off-line analysis. The mean EMG activity of the middle two seconds of each four-second MVIC testing was calculated to determine the individual’s MVIC. For the exercises, the mean EMG activity of the middle five seconds of each 10-second intervention exercise was calculated. All data were calculated in root-mean-square (RMS) values, normalized to MVIC of the corresponding muscle, and presented as a percentage of MVIC (% MVIC). UT/LT ratios were calculated for each of the individual three trials in each of the eight exercise conditions.
A 2 x 2 x 2 (external loads x scapular positions x shoulder positions) repeated-measures analysis of variance (ANOVA) was used to identify any difference in the mean values of normalized EMG muscle activity. This three-way counterbalanced repeated-measures ANOVA analysis was also used to identify a difference in the mean ratios of UT to LT normalized EMG muscle activity. In addition, a one-way repeated measures ANOVA was used to identify a difference in the mean values of IS normalized EMG muscle activity across two different GHJ positions (NEUT, HADD) in the scapular retraction position (RET), and ER in response to isometric contraction with 40% MMT as well as the mean values of SA normalized EMG muscle activity between the supine and side-lying position with the 9.1 kg dumbbell in NEUT and HADD in the scapular protraction position (PRO). Where appropriate, a post hoc test with Tukey’s honestly significant difference (HSD) was used to measure any significant difference between the three different arm positions. The significance level was set at α = 0.05. Additionally, the effect size of omega square (ω2) was calculated to estimate the amount of variance.
RESULTS
Twenty collegiate baseball players, including 10 pitchers, belonging to the National Collegiate Athletic Association Division I conference (height: 185.3 ± 5.1 cm, mass: 90.7 ± 12.6 kg, age: 20.1 ± 1.8 years) participated in this study. The mean force values produced in the prone HABD at 90 ABD arm position and the seated ER at 0 ABD arm position were 119.8 [+/- 16.0] N or 12.2 (+/- 1.6) kg and 69.8 (+/- 11.2) N or 7.1 (+/- 1.1) kg, respectively. Subsequently, the mean value used for 40% MMT load that the subjects were asked to match was 47.9 N or 4.9 kg for the HADD resistance exercise regardless of the shoulder and scapular positions and 27.9 N or 2.8 kg for the IR resistance exercise.
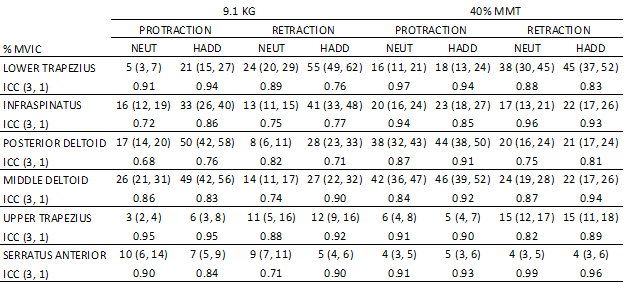
Mean values, 95% confidence intervals, and intraclass correlation coefficients (ICCs) (3, 1) for each of the six EMG activities (% MVIC) are presented in Table 1. The mean of the ICCs (3, 1) in the four different arm positions with the two different weight loads was 0.86.

Lower Trapezius
Comparison between 9.1 kg and 40% MMT
A significant 3-way interaction in the mean values of LT EMG activity between the two different external load exercises by the two scapular positions and two shoulder positions was found [F (1, 19) = 5.60, p = 0.029, ω2 = 0.18]. Specifically, the mean value was significantly greater with 40% MMT in PRO for NEUT than that of 9.1 kg (p < 0.001) (16 vs 5% MVIC, respectively), whereas no significant difference was observed between the two different external load exercises in PRO for HADD (p = 0.328). Likewise, the mean LT value was significantly greater with 40% MMT in RET for NEUT than that of 9.1 kg (p < 0.001) (38 vs 24% MVIC, respectively). Conversely, the mean value was significantly greater with 9.1 kg in RET for HADD than that of 40% MMT (p < 0.001) (55 vs 45% MVIC, respectively). (Figure 3)

Comparison between Retraction and Protraction
The mean values of LT EMG activity were significantly greater in RET with 9.1 kg than those of PRO for both NEUT and HADD (p < 0.001) (24 vs 5% MVIC for NEUT); (p < 0.001) (55 vs 21% MVIC for HADD). Likewise, the mean values were significantly greater in RET with 40% MMT than those of PRO for both NEUT and HADD (p< 0.001) (38 vs 16% MVIC for NEUT) (p < 0.001) (45 vs 18% MVIC for HADD). (Figure 3)
Comparison between NEUT and HADD positions
The mean values were significantly greater for HADD with 9.1 kg than those of NEUT in both PRO and RET (p < 0.001) (21 vs 5% MVIC for PRO) (p < 0.001) (55 vs 24% MVIC for RET). In contrast, no significant difference was observed between NEUT and HADD with 40% MMT in both PRO and RET (p = 0.532 and 0.063, respectively). (Figure 3)
Infraspinatus
Comparison between 9.1 kg and 40% MMT
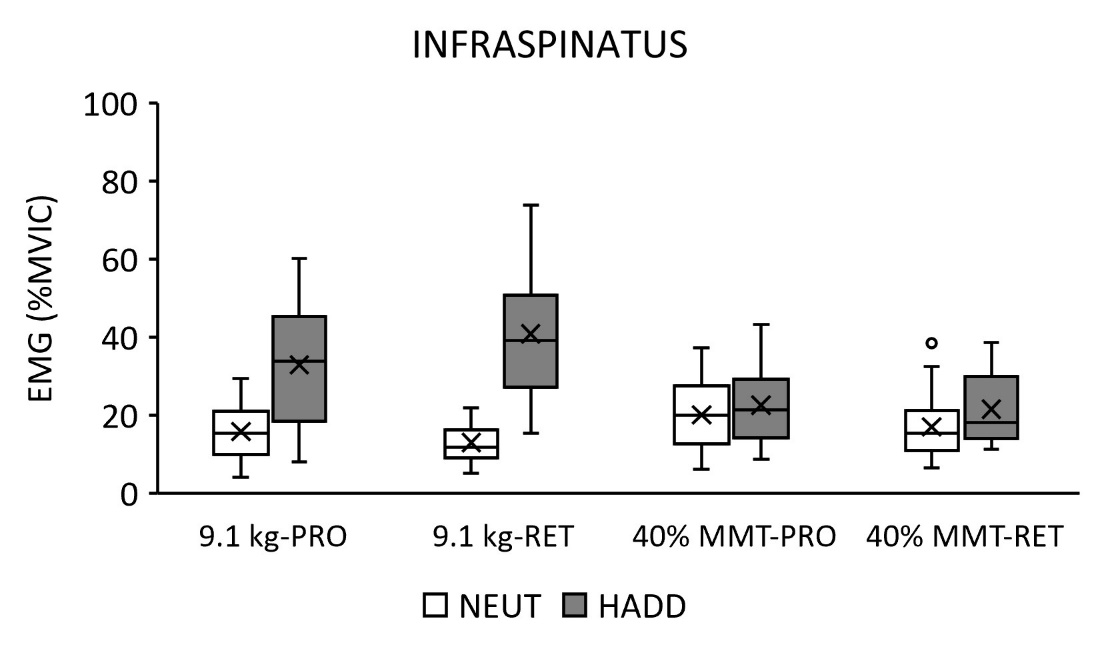
A significant 3-way interaction in the mean values of IS EMG activity was found between the two different external load exercises by the two scapular positions and two shoulder positions [F (1, 19) = 9.37, p = 0.006, ω2 = 0.29]. Specifically, the mean values were significantly greater with 9.1 kg for HADD than those of 40% MMT in both PRO and RET (p < 0.001) (33 vs 23% MVIC, respectively); (p < 0.001) (41 vs 22% MVIC, respectively), whereas no significant difference was observed between the two different external load exercises for NEUT in both PRO and RET (p = 0.07 and 0.10, respectively). (Figure 4)

Comparison between Retraction and Protraction
The mean value of IS EMG activity was significantly greater in RET with 9.1 kg for HADD than that of PRO (p < 0.001) (41 vs 33% MVIC, respectively), whereas no significant difference was observed between RET and PRO with 9.1 kg for NEUT (p = 0.22). No significant difference was observed between RET and PRO with 40% MMT for both NEUT and HADD (p = 0.64 and 0.16, respectively). (Figure 4)
Comparison between NEUT and HADD positions
The mean values were significantly greater for HADD with 9.1 kg than those of NEUT in both PRO and RET (p < 0.001) (33 vs 16% MVIC for PRO) (p < 0.001) (41 vs 13% MVIC for RET). Likewise, the mean value was significantly greater for HADD in RET with 40% MMT than that of NEUT (p = 0.033) (22 vs 17% MVIC), whereas no significant difference was observed between NEUT and HADD in PRO with 40% MMT (p = 0.243). (Figure 4)
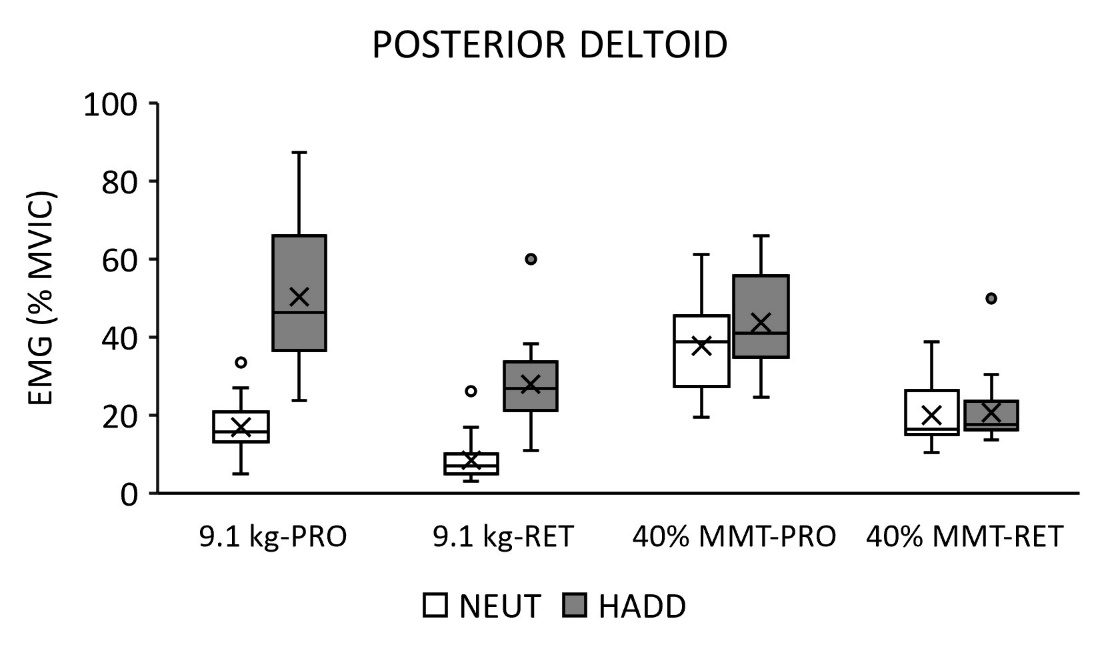
Posterior Deltoid
Comparison between 9.1 kg and 40% MMT
A significant 3-way interaction was found in the mean values of PD EMG activity between the two different external load exercises by the two scapular positions and two shoulder positions [F (1, 19) = 4.86, p = 0.006, ω2 = 0.16]. Specifically, the mean values were significantly greater with 40% MMT for NEUT than those of 9.1 kg in both PRO and RET (p < 0.001) (38 vs 17% MVIC for PRO, respectively) (p = 0.033) (20 vs 8% MVIC for RET, respectively). In contrast, the mean values were significantly greater with 9.1 kg for HADD than those of 40% MMT in both PRO and RET (p < 0.001) (50 vs 44% MVIC for PRO, respectively); (p = 0.019) (28 vs 21% MVI for RET, respectively). (Figure 5)

Comparison between Retraction and Protraction
The mean values of PD EMG activity were significantly greater in PRO with 9.1 kg than those of RET for both NEUT and HADD (p = 0.010) (17 vs 8% MVIC for NEUT, respectively); (p < 0.001) (50 vs 28% MVIC for HADD, respectively). Likewise, the mean values were significantly greater in PRO with 40% MMT than those of RET for both NEUT and HADD (P < 0.001) (38 vs 20% MVIC for NEUT, respectively) (p < 0.001) (44 vs 21% MVIC for HADD, respectively). (Figure 5)
Comparison between NEUT and HADD positions
The mean values were significantly greater for HADD with 9.1 kg than those of NEUT for both PRO and RET (p < 0.001) (50 vs 17% MVIC for PRO); (p < 0.001) (28 vs 8% MVIC for RET). In contrast, no significant difference was observed between NEUT and HADD in 40% MMT for both PRO and RET (p = 0.068 and 0.822, respectively). (Figure 5)
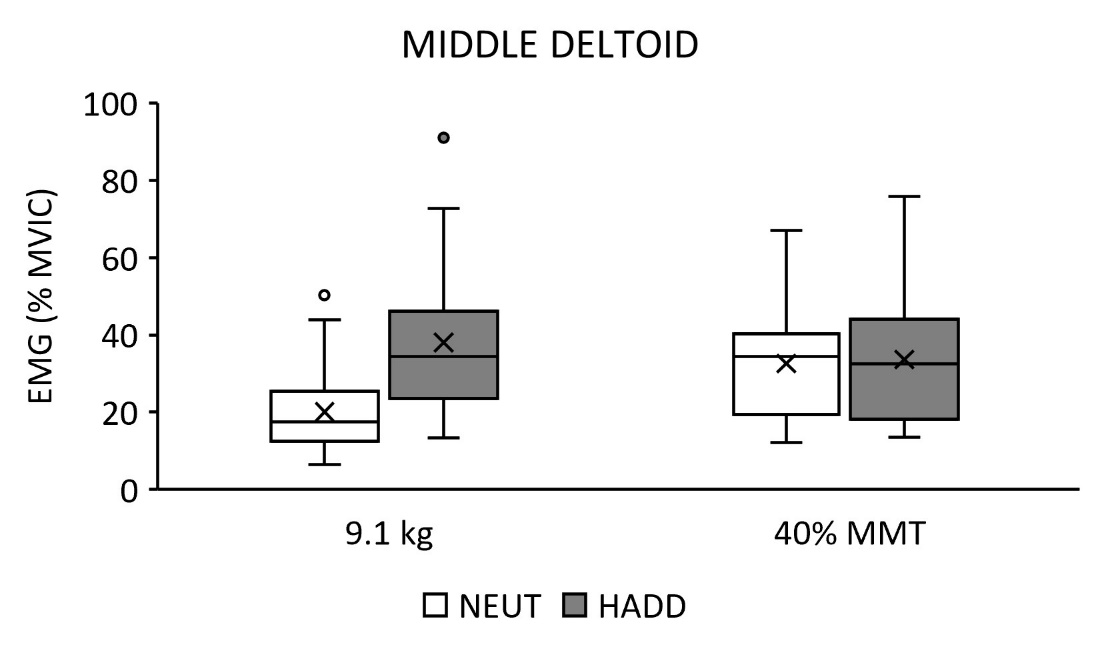
Middle Deltoid
Comparison between 9.1 kg and 40% MMT
No significant interaction in the mean values of MD EMG activity between the two different external load exercises by the two scapular positions and two shoulder positions was found (p = 0.378). However, there was a 2-way interaction in the mean values between the two different external load exercises by two shoulder positions [F (1, 19) = 62.8, p < 0.001, ω2 = 0.75]. Specifically, the marginal mean value was significantly greater with 40% MTT for NEUT than that of 9.1 kg regardless of the scapular positions (p < 0.001) (33 vs 20% MVIC for NEUT, respectively) whereas the marginal mean value was significantly greater with 9.1 kg for HADD than that of 40% MTT (p = 0.015) (38 vs 34% MVIC for HADD, respectively). The marginal mean value was significantly greater for HADD with 9.1 kg than that of NEUT regardless of the scapular positions (p < 0.001) (38 vs 20% MVIC, respectively) whereas no significant difference between the two exercises for HADD with 40% MMT (p = 0.069). (Figure 6a)


The glenohumeral joint was no (0°) horizontally adducted from the coronal plane (NEUT) and 15° horizontally abducted from the coronal plane (HADD) during side-lying isometric contraction while the scapula was protracted (PRO) and retracted (RET). Each of the electromyographic (EMG) activities was normalized to maximum voluntary isometric contraction (MVIC) of the corresponding muscle and presented as a percentage of MVIC (% MVIC) in the vertical axis.
Side-Lying External Rotation
Mean values, standard deviations, and the ICCs (3, 1) of each of the six muscle activities are presented during side-lying ER with the elbow flexed to 90° in Table 2. Specifically, the mean value of the IS muscle activity was significantly greater in side-lying ER with the elbow flexed to 90° with 40% MMT than that of both NEUT and HADD in the RET (Tukey’s HSD (DTukey) = 5.5%, p < 0.05) (44, 17, and 22% MVIC, respectively).
__and_intraclass_correlation_coeffi.png)
Supine Protraction
Mean values, standard deviations, and the ICCs (3, 1) of each of the six muscle activities are presented during supine PRO in Table 2. Specifically, the mean value of the SA muscle activity was significantly greater in supine PRO with 9.1 kg than that of both NEUT and HADD in the PRO (DTukey = 4.2%, p < 0.05) (39, 10, and 7% MVIC, respectively).
Mean values, standard deviations, and the ICCs (3, 1) of each of the six muscle activities are presented during supine PRO in Table 2. Specifically, the mean value of the SA muscle activity was significantly greater in supine PRO with 9.1 kg than that of both NEUT and HADD in PRO (DTukey = 4.2%, p < 0.05) (39, 10, and 7% MVIC, respectively).
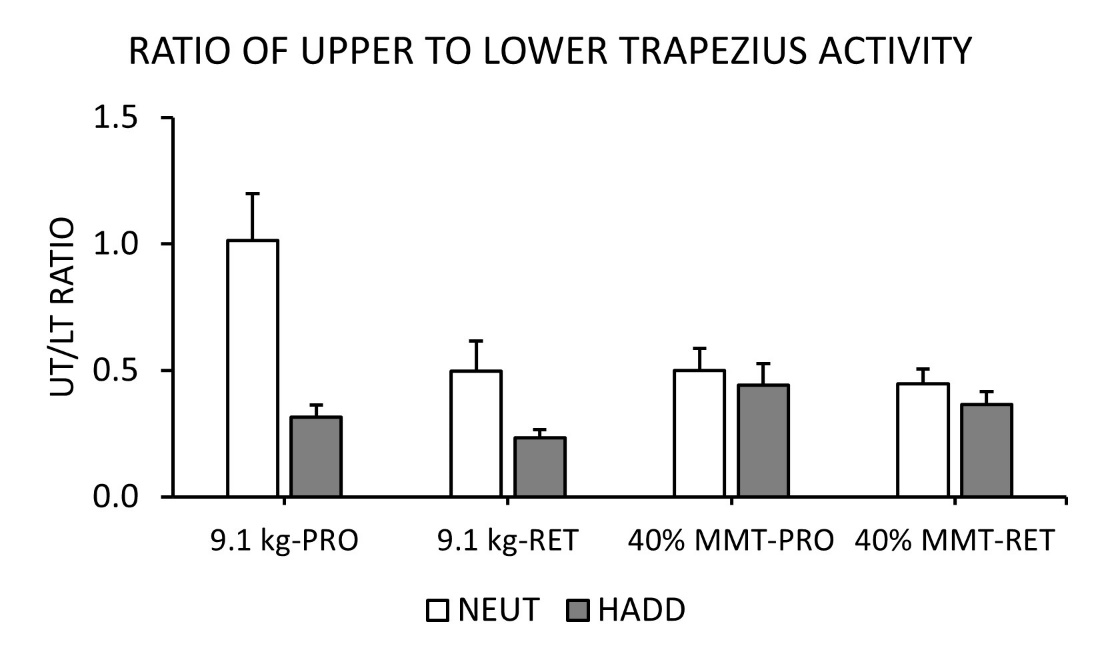
Ratio of Upper to Lower Trapezius
A significant 3-way interaction was found in the mean values of the UT/LT ratio between the two different external load exercises by the two scapular positions and two shoulder positions [F (1, 19) = 5.94, p = 0.025, ω2 = 0.14]. Specifically, the mean UT/LT ratio was significantly greater with 9.1 kg for NEUT than that of 40% MMT in PRO (p = 0.013) (1.01 vs 0.50, respectively) (p = 0.013). Also, the mean ratio was significantly greater in PRO with 9.1 kg for NEUT than that of RET (p < 0.001) (1.01 vs 0.50, respectively). Likewise, the mean UT/LT ratios were significantly greater for NEUT in 9.1 kg than those of HADD for both PRO and RET (p < 0.001) (1.01 vs 0.32 for PRO, respectively) (p < 0.04) (0.50 vs 0.23 for RET, respectively). (Figure 7)
_to_lower_trapezius_(ut)_muscle_activity.jpeg)
DISCUSSION
The results of this study supported the primary hypothesis in which the side-lying position with the shoulder abducted to 90° with the scapula retracted significantly minimized deltoid muscle activity (up to 27% MVIC), which in turn significantly increased LT activity with the shoulder horizontally abducted 15° from the coronal plane (55% MVIC with the 9.1 kg dumbbell). This side-lying arm position exercise minimized MD activity by almost half of the amount of MD activity performed in standing horizontal abduction exercise at 120° ABD with an elastic resistive band while it activated the LT more than that of the standing exercise.14 The LT plays a critical role in maintaining the posterior tilt and external rotation of the scapula during the late cocking phase of the throwing or serving motion.1,26 Conversely, excessive activity of the MD decreases the subacromial space width as a result of superiorly directed humeral head translation relative to the glenoid fossa.19,23 In summary, side-lying isometric shoulder abduction exercise with scapular retraction can substantially activate the LT muscle in the position of shoulder horizontal adduction while compensatory activity of the MD muscle can be minimized.
The UT/LT ratios calculated in this study were significantly lower in the side-lying scapular retraction position with the dumbbell weight of 9.1 kg, compared to the scapular protraction position. These UT/LT ratios were similar to the ratios seen during performance of prone ER in 90° of shoulder abduction and side-lying ER with a weight of 1 kg in hand during isotonic exercise without the instruction for active scapular retraction.27 It was presumed that for the side-lying position the gravitational force assisted with the placement of the scapula toward the spine. The scapular position in turn minimized the activity of the rhomboid muscles, which could be co-contracted with the UT muscle when the scapula was retracted.10 Subsequently, the findings of this study show the side-lying abduction exercise can effectively minimize UT activity, regardless of shoulder positions (NEUT and HADD). Therefore, this exercise might help those who need to improve the optimal UT/LT ratio, such as patients with subacromial impingement syndrome.3,7
The amount of IS activity generated in the side-lying horizontal abduction exercise was less than half of the IS muscle activity generated in the side-lying ER exercise. The findings of this study were consistent with previous studies in which the IS was hardly activated during isolated horizontal abduction exercise in the position of shoulder abduction.15,21,22 Previous studies also have revealed that resistance of horizontal adduction at 90° of shoulder abduction significantly augmented IS activity when the subjects generated shoulder ER force.15,22 Taken together, IS activity decreases in horizontal abduction exercise without ER force generation.21
The amount of activity of the IS has been demonstrated to vary with the amount of MD activity during ER exercise of the GHJ at 0° ABD19,20 MD activity can be further decreased in the scapular plane, compared with the coronal plane during ER exercises.15,21,22 The side-lying abduction with the elbow straight position with the scapula retracted placed the humeral head in the GHJ steadily enough to minimize both MD and IS activities in the NEUT position. The horizontal adduction position at 15° from the sagittal plane with the dumbbell weight produced only a mild amount of MD activity. Consequently, the findings of this study indicate that such small degrees of horizontal adduction position may involve the IS in an attempt to stabilize the humeral head in the GHJ, leading to an increase in the muscle activity as much as side-lying ER exercise at 0° ABD.
The PD has been reported to contribute to ER force in shoulder abduction along with the external rotators of the GHJ.28 In addition, the PD can be positively associated with the LT in quadruped shoulder flexion,29 arm elevation in the scapular plane, (known as scaption),23 prone horizontal abduction,21 Shoulder ER at 90° of abduction with the elbow flexed to 90°, (known as 90/90 ER),14,15,21,29 and dynamic motion exercises, such as the lawn mower and robbery exercise.25,30 This study revealed that the amount of PD activity was reduced in the scapula retracted condition during the side-lying abduction exercises regardless of the different external loads, compared with the scapular protraction condition. Likewise, the PD barely contributed to ER force in the side-lying ER exercise, which may be accounted for by the muscle length-tension relationship.31 Therefore, both LT and IS activities can be independent of PD muscle activity in the side-lying abduction exercise with scapular retraction.
Limitations
This study determined the amount of exercise intensity based on MD activity ranging between low and moderate activity as indicated by DiGiovine et al.5 Although a significant difference was found in the marginal mean value of MD activity between the two exercise intensities: the external weight of 9.1 kg dumbbell and external force generated by 40% MMT (38% vs 34% MVIC), the exercise interventions demonstrated in this study were comparably controlled to identify LT activity modulations. This study solely included collegiate baseball players with asymptomatic shoulders and all analyses were performed only on the dominant side. Thus, the implication of the findings to individuals with differing age, levels of performance, presence of shoulder symptoms, non-dominant side, and the dumbbell weight used in this study may have limitations.
CONCLUSION
This study investigated the amount of scapular, deltoid, and rotator cuff muscle activity during two isometric exercise positions with altered scapular positions and differing external loads. The findings of this study suggest that the amount of LT activity can be modulated by changes in scapulothoracic and glenohumeral positioning. This study also revealed that IS activity was augmented with the scapula retracted in the side-lying abduction exercise by the external load of a dumbbell, compared with resistance of HADD. Changes in the UT/LT ratio based on scapular position and exercise characteristics were observed. Further studies are warranted to investigate the effect of scapular positions on the activity of the LT, IS, UT, and deltoid muscles in side-lying exercises for use in injury prevention programs, especially for those overhead athletes who need to improve scapular muscle balance ratios.
Conflicts of Interest
The authors have no conflicts of interest to declare that are relevant to the content of this study.
Acknowledgement
The authors thank Wesley Clawson and Karter Lang, MA, ATC for their assistance with data collection during this study.