



INTRODUCTION
According to the National Golf Foundation (NGF), golf is increasing in popularity now being played in 209 of 249 countries, including six continents, with 24.8 million golfers in the U.S. in 2020.1–3 This was a 2% increase (500,000 golfers) over 2019, which is the most significant net increase in 17 years.1 One possibility for the recent rise in the number of golfers may be due to the recent COVID-19 pandemic, allowing more time to be outside and start a new hobby. This number increased to 37.5 million in 2021 which can be further broken down to 25.1 million on course and 12.4 million participating in off course activities,2 including the driving range, TopGolf, mini golf, etc. Women golfers were also a part of the 2020 surge, jumping 8% (450,000 golfers) and making up nearly a quarter of all golfers reaching upwards of six million.1
Despite the increase in popularity, playing golf does not come without risk of injury. One systematic review in 2009 described golf as an overall moderate risk activity for injury compared to other sports.4 In amateur golfers the incidence of injury annually has been reported to be between 15.8% and 40.9%,5–8 with a lifetime incidence between 25.2% and 67.4%.7 This contrasts with professional golfers, who have a slightly higher incidence for injury at 66% during their career and 31% in the last year.9 Professional golfers have a much higher volume of repetitive practice as compared to amateur golfers, which tends to be the most frequent cause of injury, compared to suboptimal swing biomechanics in amateurs.5,8 In most cases (82.6%) injuries reported in golf are due to overuse, with only 17.4% occurring because of a singular traumatic event.10
COMMON INJURIES IN GOLF
The most common injury sites documented in professional golfers are the low back followed by the wrist.9,11,12 Percent breakdown per joint includes lower back (44%), wrist (44%), elbow (23%), neck (20%), and shoulder (19%).9 It has also been noted that men are 2.5x more likely to sustain a lower back injury than women.9 Vad et al. found that a history of low back pain in golfers was significantly correlated with a decrease in lead hip internal rotation, FABER’s distance (knee to table measurement), and lumbar extension.13 In amateurs the most common site of injury is the elbow (24.9%) and shoulder (18.6%), followed by the lumbar spine (15.2%).12 Nearly half (46.2%) of injuries reported are sustained during the golf swing with 23.7% occurring at the point of ball impact, with the remainder of injuries occurring outside of the golf swing.10 Barclay et al. reported that of those who sustain an injury golfing, 72% take time off, relying on time to heal, whereas 83% seek out the assistance of a physical therapist.9
BIOMECHANICS OF THE GOLF SWING
The mechanics of the golf swing can be broken down into five distinct phases including the takeaway, forward swing, acceleration, early follow-through, and late follow through.10 This was initially described by Stover et al and Hosea et al in which they discussed the difference between the classic and modern golf swing.14,15 The most significant difference between the two is the emphasis on hip and trunk dissociation, which has been shown to improve performance, but has also been described as a risk factor for recurrent injury.11,14–16 The classic golf swing involves the pelvis and trunk rotating equally throughout finishing in a relaxed and upright position towards the target.16 The modern golf swing encourages further hip and trunk dissociation leading to an increase in elastic potential energy resulting in the ability to generate more force and maximize club head speed.16,17 McLean described this as the “X-factor” and noted that a larger X-factor (increase in the shoulder/pelvis dissociation) resulted in better performance.17 Despite the increase in performance, the modern golf swing has also been associated with an increased risk of injury due to the nature of finishing in a hyperextended position.18 This has been described as the “reverse C” finish which can lead to increased incidence of low back pain possibly due to increase facet joint irritation.18 Therefore, to maximize performance while minimizing the risk of injury, it is essential to optimize swing mechanics.
INJURY PREVENTION/PERFORMANCE
Golf has been shown to provide moderate intensity aerobic physical activity. As a result, a beneficial effect in both physical and mental health can be expected.19–21 Uthoff et al found that an eight-week program consisting of a combination of nonspecific and golf specific training enhanced both club head speed (4.1%) and hitting distance (5.2%) demonstrating the importance of golf specific training for performance enhancement.22 McHugh et al looked at the importance of transverse plane flexibility in golfers and found that proficient golfers, compared to those of similar skill level, had significantly better glenohumeral and hip joint flexibility as well as spinal mobility in the transverse plane with no difference in the sagittal and frontal plane.23 They noted that transverse plane hip flexibility accounted for 48% of the variability in ball speed and 45% of the variability in total distance which they attributed to greater separation between pelvis and trunk (known as the “X-factor”).23
Injury prevention programs have shown to be successful in other sports,24 however to date there are no studies assessing a golfer’s specific program. Gladdines et al. designed a protocol for a Golf Related Injury Prevention Program (GRIPP intervention) consisting of six different movements (leg swings, arm in the air, arm rotations, sideways bending, rotation of the upper back, powerful rotations) in which they plan to compare to their typical warm up.25 The Titleist Performance Institute (TPI) screening is also growing in popularity among health care professionals to evaluate a golfer for physical limitations which may inhibit swing efficiency and durability.26 Currently, there is no proven gold standard for screening. A systematic review completed by Ehlert et al. suggested that various warm-up protocols may enhance golf performance, however observational data suggests that many golfers do not regularly perform them.27 A good conditioning and warm up routine can help golfers train their body to better withstand the repetitive forces involved in the golf swing.10
The purpose of this clinical commentary is to describe three individualized and unsupervised golf exercise programs (The Golfer’s Fore, Fore+, and Advanced Fore+), of varying difficult, designed to reduce the risk of injury, improve strength/mobility, and optimize performance. The progressive program consists of three levels; therefore, they apply to all ages, level of competition, and training experience. It can be modified to be utilized as a warm prior to a round or serve as a foundation to your regular exercise program.
THE GOLFER’S FORE PROGRAM(S)
The three programs outlined in this commentary (The Golfer’s Fore, Fore+, and Advanced Fore+) can be utilized for performance enhancement and/or injury prevention with an emphasis on strength, mobility, and core activation. The purpose is to create a simple and easy to follow program that incorporates the entire kinetic chain with multi-planar movements while preparing the golfer for the demands of their sport. All exercises performed are completed utilizing body weight and/or a single piece of TheraBand CLX, making them easy to perform and accessible for all athletes regardless of talent level or training age. The athlete is instructed to perform 2 sets of 10 repetitions for each exercise with minimal to no rest between movements. The intensity level and/or timing of season will dictate the number of sessions per week. Each program in its entirety can be found in Appendices 1-3, as well as a QR code with a video of each individual section, (mobility, strength, and core) for all three programs.
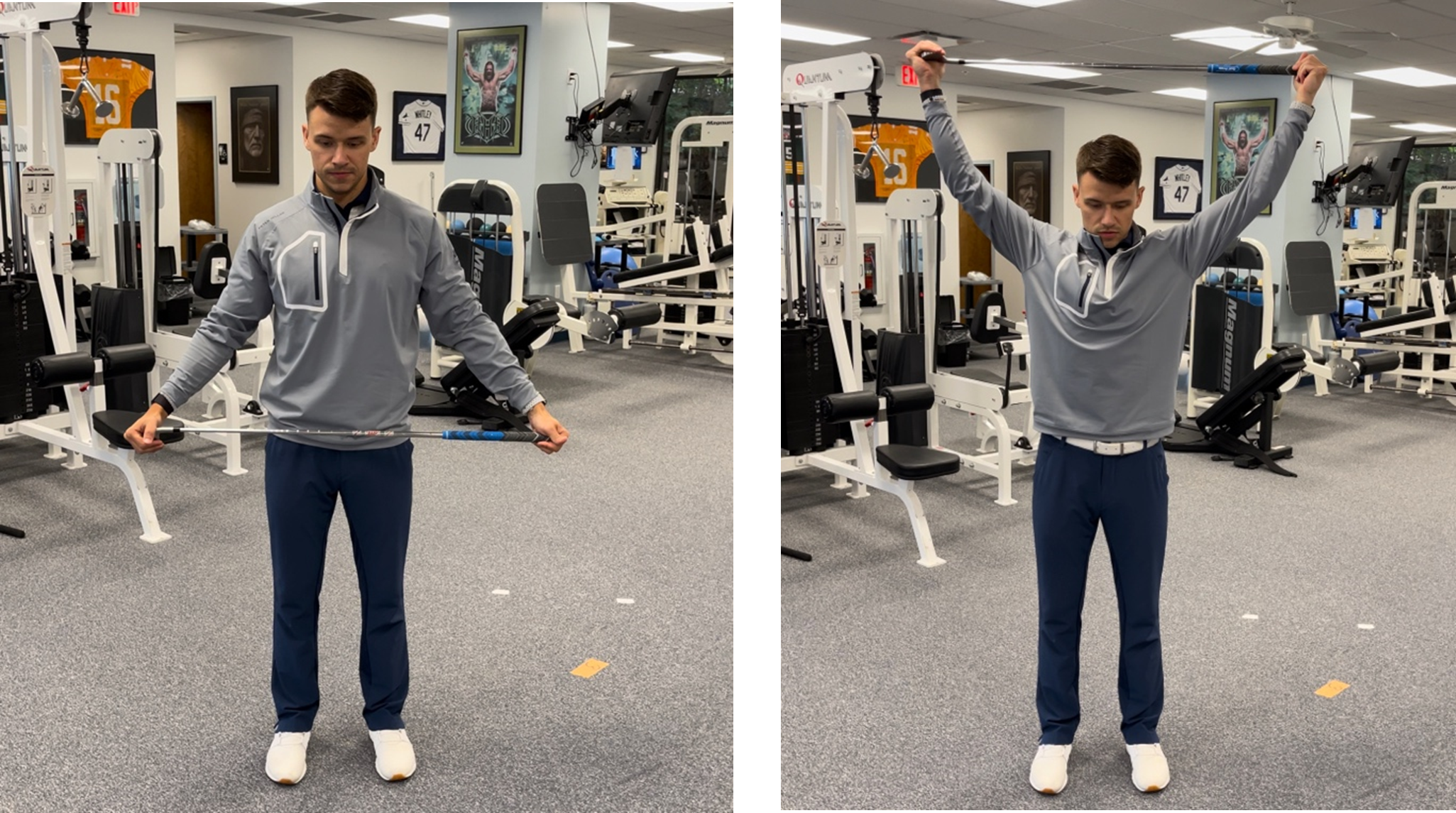
The Golfer’s Fore (Appendix 1) program begins with four mobility movements, followed by ten strengthening and four core exercises. This program serves as the foundation for the remaining two programs. Starting with mobility, the program begins with standing cross body adduction. The athlete is instructed to stand against a wall to stabilize the scapula and maximize the stretch. The horizontal adduction stretch has been advocated to improve flexibility of the posterior shoulder region28–30 which is important throughout the golf swing in both the lead and trail arm. Next exercise includes, around the world with a golf club, emphasizing glenohumeral joint mobility in all planes, which is essential for the dynamic nature of the golf swing. The last two mobility exercises, half kneeling thoracic rotation (Figure 1) and squats with rotation, begin to incorporate lower extremity and thoracic spine mobility. Zouzias et al. noted the importance of a well-rounded golf specific exercise program including lower extremity and thoracic spine mobility.10
.png)
Next, the strengthening aspect of the program begins with low row in a split lunge. The exercise starts with the athlete in a split stance lunge with opposite arm forward (example: left leg and right arm) holding a TheraBand in their hand. Maintaining a stable base, they are instructed to row with the right arm and reach with the left until their right arm is parallel with their side. The reach on the opposite side incorporates thoracic spine mobility and emphasizes the dissociation between the lower half (pelvis). To perform the second set, the athlete will switch their footing such that their lead leg in the first set will now be their trail leg in the second, and vice versa. The purpose of the sustained split lunge is to incorporate the lower half into the movement and elicit activation of the entire kinetic chain. It also emphasizes single limb stability/control which is important throughout the weight shift from lead to trail leg during the golf swing.
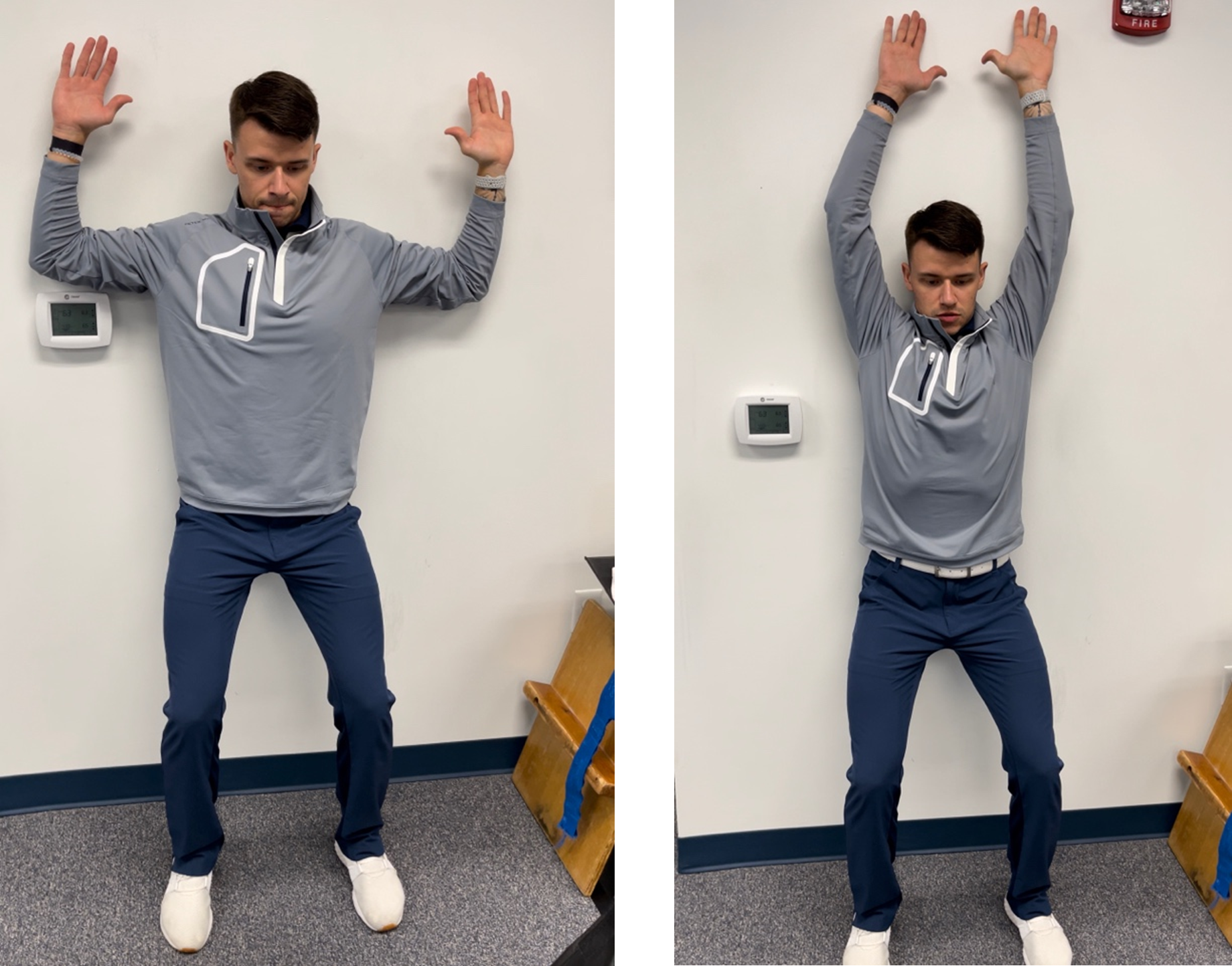
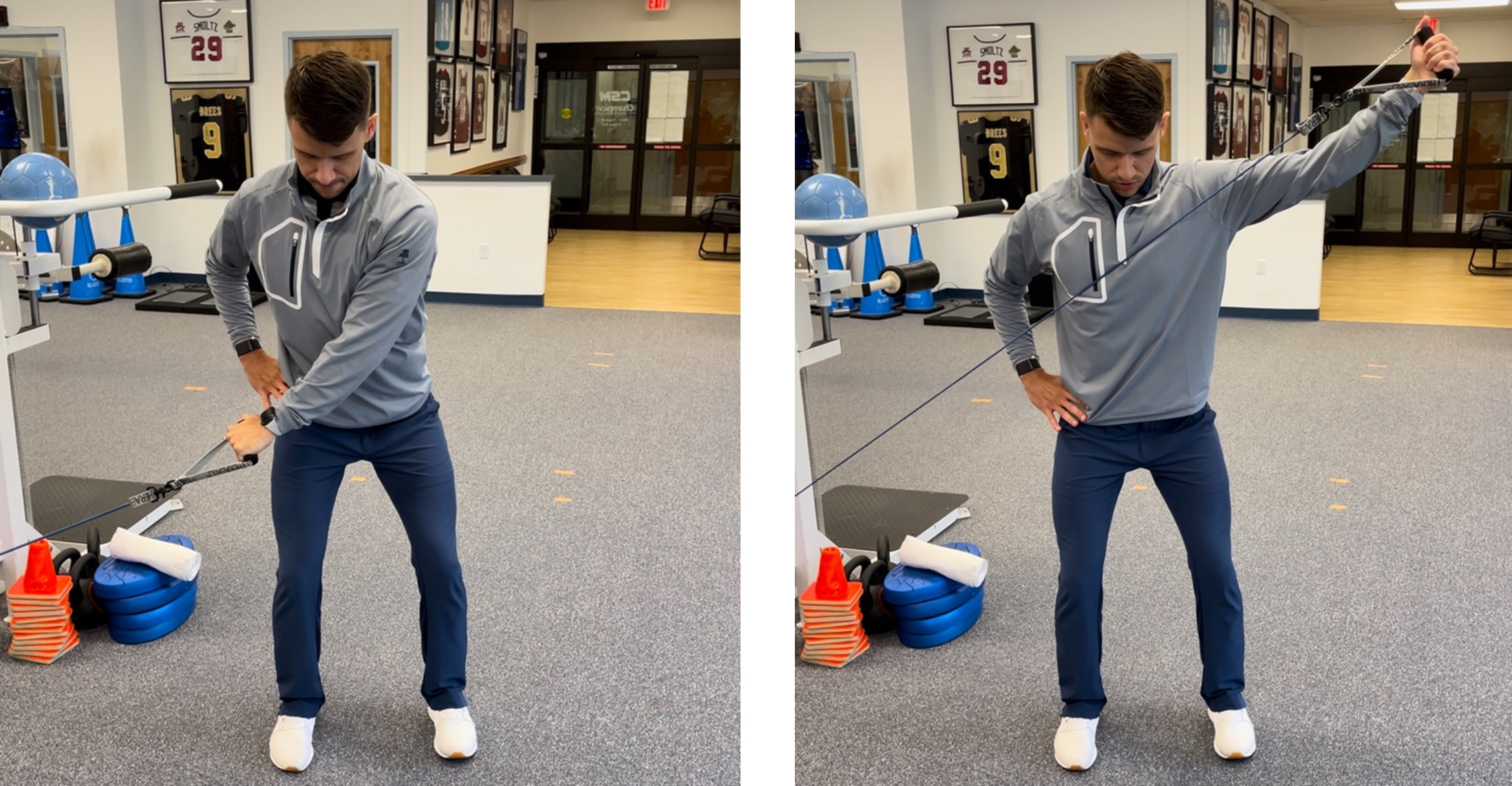
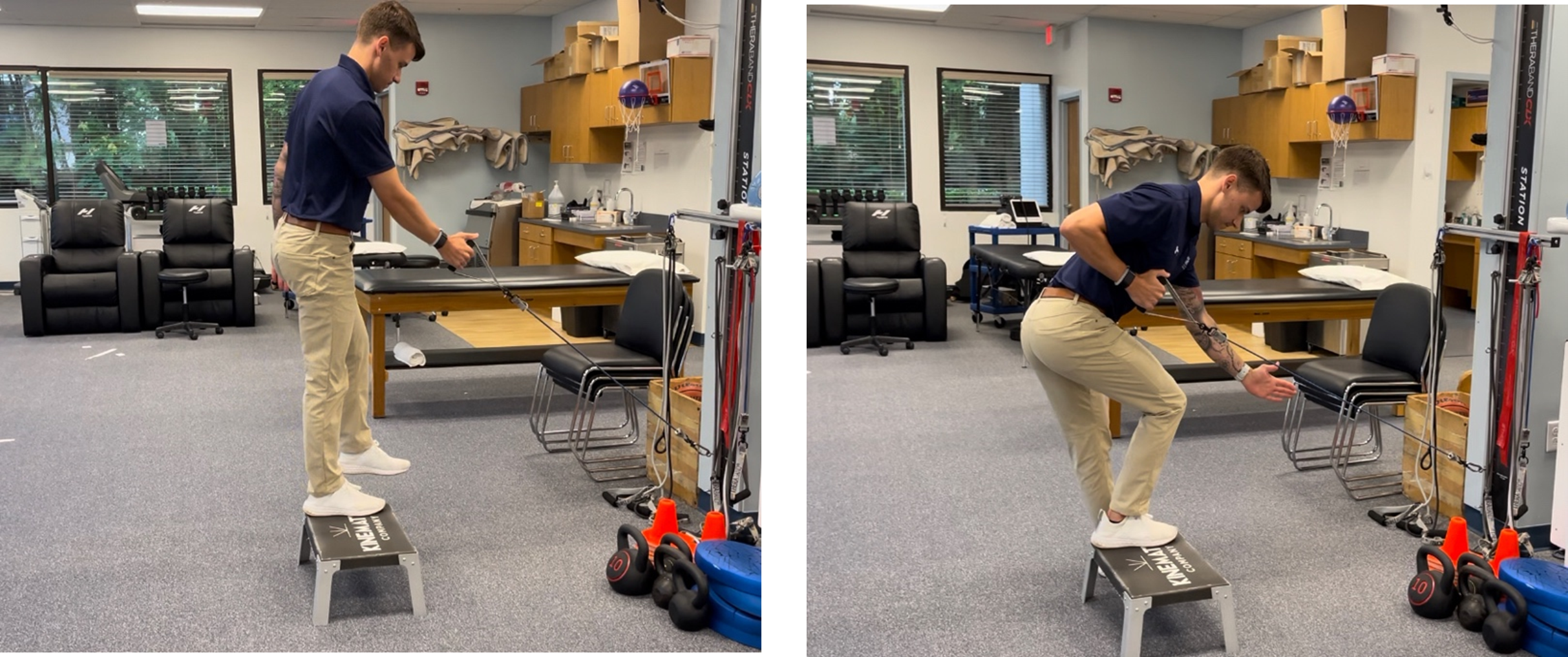
This is followed by proprioceptive neuromuscular facilitation (PNF) D1 and D2 flexion/extension in a squat. For this movement the athlete will stand parallel to the TheraBand and will be pulling across their body from low to high. D1 flexion begins with the TheraBand in their inside hand and on the inside hip as compared to D2 flexion which begins with the TheraBand in the outside hand on the inside hip. It is important to educate the athlete on the importance of both D1 and D2 extension as well to maximize eccentric control. Reverse wall slides (Figure 2) are next emphasizing upper extremity flexibility, thoracic mobility, and posterior rotator cuff activation. The athlete is instructed to complete this movement in a sustained squat maintaining contact with the wall at the hand, elbow, and lower back.
.png)
Next, is the scapular series including the prone horizontal abduction (T), prone high row into external rotation (W), and the modified robbery (Figure 3). Both the prone T and W are completed lying on a table, face down, and one arm off the side. The modified robbery is an alteration of the original robbery exercise described by Kibler et al.31 It is completed in a mini squat utilizing one piece of TheraBand, holding onto one handle in each hand with elbows bent to 90° and at their side. Thumbs should be positioned outwards with palms towards the ceiling. Maintaining elbows in contact with their side, the athlete rotates arms outward squeezing shoulder blades together. They are instructed to hold this position for two seconds then return to starting position. A pilot study completed at the American Sports Medicine Institute (ASMI) in Birmingham, AL examined the EMG activity of various scapular strengthening exercises noting that the modified robbery demonstrated the greatest lower trapezius activation with minimal upper trapezius contribution (unpublished).
.png)
Both double and single leg bridges further facilitate increased lower extremity strengthening. Power generation during the golf swing combines trunk and pelvis dissociation, optimal mechanics, as well as lower extremity strength. The athlete begins on their back with knees bent to approximately 90 degrees and feet shoulder width apart. Pushing through their heels, with both core and gluteal muscles engaged they will lift their bottom off the ground, hold for two seconds then return to starting position. Incorporating single leg bridges will increase the demand on the lateral hip musculature to optimize pelvic stability. The strength portion of the program finishes with a forward lunge into rotation. The athlete begins standing with arms straight out in front holding a golf club and feet shoulder width apart. They are instructed to perform a lunge, rotate towards the forward leg maintaining arms straight, then push from the front leg, returning to the starting position.
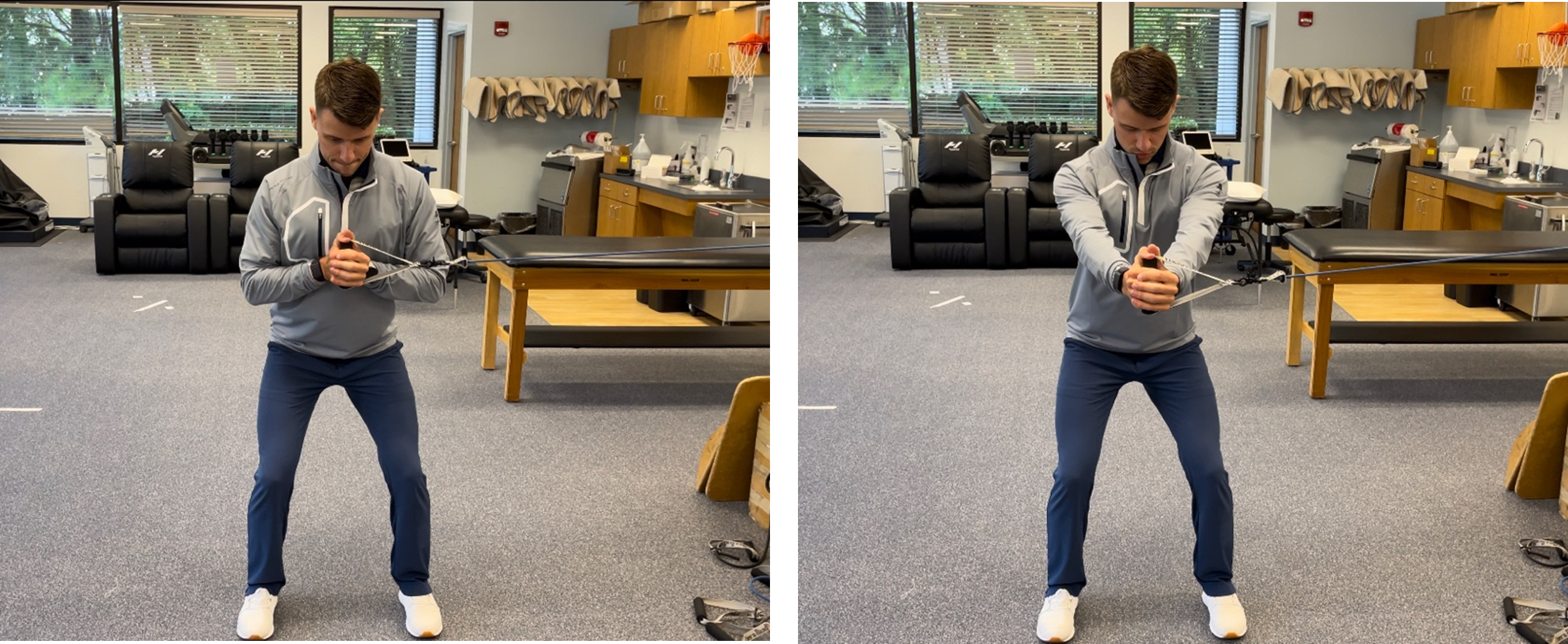
The three core movements within the Golfer’s Fore include a palloff press, quadruped arm/leg reaches (bird dogs), and supine arm/leg movements (dead bugs). For the palloff press the athlete begins in a mini squat facing perpendicular to the TheraBand holding it with both hands against their body just below chest height. Maintaining the squat, they are instructed to push both hands out directly in front until their arms are straight and not allowing the trunk to rotate. This movement works on transverse plane strength and stability in which McHugh et al demonstrated the importance of during the golf swing.23 The bird dog begins with the athlete in a quadruped position, shoulders stacked above wrist and hips above knees with core engaged and neutral spine positioning. The movement begins by reaching forward with one arm and at the same time kicking backwards with opposite limb, keeping both as straight as possible. After holding the finishing position for two seconds, they will then return to the starting position and complete with the opposite limbs, repeated for the desired number of repetitions. The dead bug is similar however completed while lying on their back and alternating arms and legs maintaining a stable core.
Both The Golfer’s Fore + and The Advanced Golfer’s Fore + progress from the foundational exercise program described above with continued emphasis on upper and lower extremity mobility/strength, core stability, and spinal mobility. The Golfer’s Fore + (Appendix 2) program begins with seven mobility movements, followed by seventeen strengthening and three core exercises (Figures 4-6).
.png)
.png)
.png)
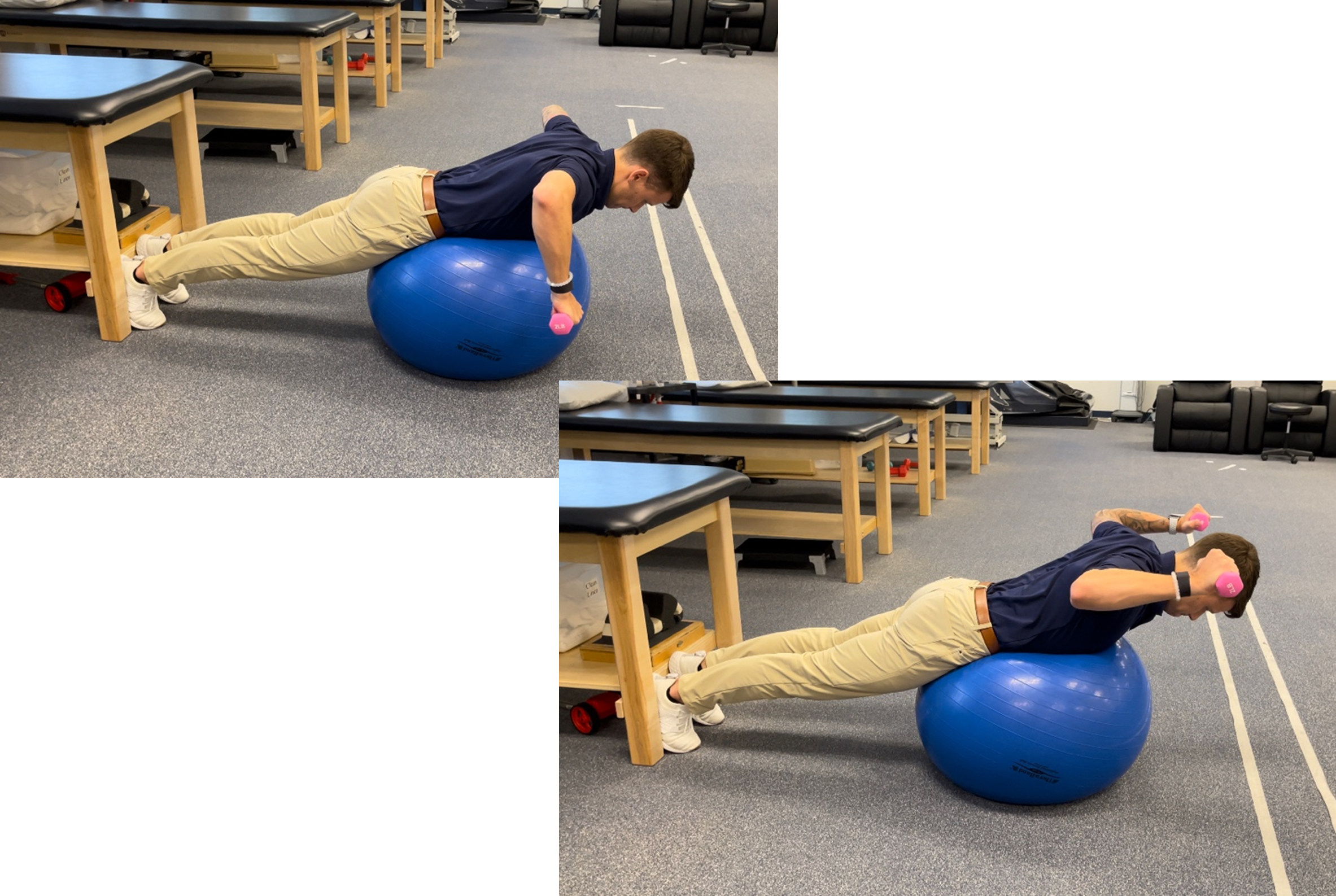
The Golfer’s Advanced Fore + (Appendix 3) program begins with eight mobility movements, followed by nineteen strengthening and three core exercises (Figures 7-10). For a more detailed description of the Fore + and Advanced Fore + programs refer to Table 2 and Table 3 as well as the QR codes provided.
.png)
_on_stability_ball_(the_advanced_golfer_s_fore_).png)
.png)
.png)
SUMMARY
The golf swing is a physically demanding and repetitive task that can lead to a variety of upper body, lower body, and/or spinal injuries. In recent years, there has been a rise in the number of golfers both in the U.S. and globally resulting in an increasing number of injuries. With a lack of consensus and research on a golfer’s specific injury prevention or performance enhancement program, it is imperative to educate the golf community on ways to train for the demands of the sport safely, efficiently, and effectively. Although not a full comprehensive or stand-alone program, The Golfer’s Fore, Fore +, and Advanced Fore + presented in this commentary provide a foundational program(s) which can be utilized for golfers of all ages and varying levels of competition to prepare for participation.
Conflicts of interest
The authors report no conflicts of interest.