INTRODUCTION
Anterior cruciate ligament (ACL) injury is one of the most common sport injuries and has a devastating influence on the activity levels and quality of life of individuals.1 ACL injuries can occur without physical contact, and thus, are considered preventable.2 The most common situation for noncontact ACL injuries appears to be deceleration, which is when the athlete cuts, changes direction, or lands from a jump.3 The Landing Error Scoring System (LESS) is a screening tool used to identify athletes presenting with high injury-risk movement patterns during a double-leg jump-landing (DLJL) task.4 Clinicians score 17 items based on movements during the DLJL task. The overall LESS score ranges from 0 to 17 errors where lower scores reflect fewer landing errors and thus fewer movement patterns linked with noncontact ACL injuries. Scores of five or more errors indicate poor jump-landing technique4 and have been linked to higher risk of ACL injury.5 Specifically, the risk ratio for sustaining a noncontact or indirect contact ACL injury was 10.7 in individuals scoring five errors or more compared to less than five errors.5 Compared to healthy controls, LESS scores are greater after an unilateral ACL reconstruction despite being cleared to return to physical activity, indicating that the LESS may provide useful information to guide rehabilitation and return-to-sport decisions.6
Across the literature, the overall LESS score demonstrates good-to-excellent reliability, and moderate-to-excellent validity versus 3-dimensional (3D) motion capture data for the items linked with risk factors for knee injury.7 Overall LESS scores are, however, sensitive to various factors, such as gender, previous injury, and intervention programs.8 Research has also identified that jump landing distance9 and final LESS score computational method10 can affect LESS scores and individual-level risk categorization. Altogether, these studies highlight that several factors and procedural methods need to be considered when administering and interpreting LESS outcomes.
Footwear plays a central role in sport and is typically designed to enhance performance and protect the body from injury. However, footwear can influence the human-ground interaction and result in different multi-joint landing strategies to moderate impact forces.11 Indeed, initial contact from a 30-cm DLJL task similar to the LESS has been associated with a more plantar-flexed ankle,12 greater foot-ground angle,12 and smaller knee range of motion13 when performed barefoot compared to with shoes. Together, these studies indicate that LESS scoring might differ between barefoot and footwear conditions, although this topic has not yet been explicitly examined. Although the LESS is traditionally performed wearing a person’s own athletic shoes,6,10 it has also been conducted barefoot.14 Therefore, the aim was to compare overall LESS scores, injury risk categorization, and specific LESS errors between habitual athletic footwear and barefoot conditions. The hypothesis was that wearing footwear would result in higher overall LESS scores, lead to a greater number of individuals classified at high risk of injuries, and influence specific LESS errors compared to barefoot. Given how footwear can influence jump performance,15 jump heights from flight times were also compared between conditions.
MATERIALS AND METHODS
Experimental approach
A randomized cross-over experimental design was used to explore the influence of footwear on LESS scores, LESS injury risk categorization, specific LESS errors, and jump height. Sample size calculations were performed a priori using G*Power 3.1.9.7, and applied a standard two-tailed hypothesis, 90% power (β = 0.10), 5% significance level (α = 0.05), one error LESS difference in paired means defining a clinically-meaningful change,4,8 and 2.47 standard deviation of the difference in paired means based on previous work implementing similar testing procedures and comparing LESS scores between two experimental conditions.9 Based on these assumptions, 67 participants were required and would be sufficient to detect a small effect size difference (Cohen d = 0.40) between conditions. A sample size of 80 participants was targeted to account for a 20% drop out rate.
Participants
Eighty participants were recruited and tested within one month in 2021 from a convenience sample of healthy university students. All volunteers were free of injury, illness, or conditions that may have affected their movements or landing mechanics. Participants with a lower extremity, back, or pelvis injury in the prior three months were excluded. LESS testing was performed in individuals’ own athletic footwear, as is typical in research and clinical settings.6,10 Participants were excluded when their footwear scored 70% or more on the Minimalist Index16 (described under Procedures) as deemed to represent minimal shoes17 that could potentially mimic barefoot.18 It was deemed inappropriate to merge data from trials performed in conventional athletic footwear to those from minimal footwear given the reported effect of these different footwear types on the biomechanics of dynamic tasks.18–20 All participants signed an informed consent document that explained the potential risks of participation (e.g., chance of injury due to physical activity). The University of Waikato Human Research Ethics Committee (HREC(Health)#2017-41) approved the protocol before data collection, which adhered to the Declaration of Helsinki. This project was retrospectively registered with the Australian New Zealand Clinical Trials Registry (ACTRN12622001358730).
Procedures
Following informed consent, baseline characteristics of participants were collected, which included measuring body height using a stadiometer (seca model 0123, Medical Measuring Systems and Scales, Mount Pleasant, South Carolina) and mass on an electronic scale (seca model ESE813, Medical Measuring Systems and Scales, Mount Pleasant, South Carolina). Participants also completed a short sport participation questionnaire, as well as the self-administered short-form International Physical Activity Questionnaire.21 According to their responses to the latter, participants were categorized as having high, moderate, or low physical activity levels.21 Participants were pre-informed of the study aims and asked to bring their own athletic footwear for testing. Footwear characteristics were measured for all participants and included the use of the Minimalist Index16 alongside more traditional characteristics. In summary, the Minimal Index measures five shoe features to quantify the level of minimalism of footwear, where 100% represents the highest degree of minimalism. The five characteristics are footwear mass, longitudinal and torsional flexibility, stack height, heel-to-toe drop, and the presence/absence of technologies. Minimal Index scores of participants’ own shoes ranged from 4 to 64%. The hardness of the midsole material in the center of the heel region was assessed using an Asker-C durometer (Supertech Precision Supply Co., LTD, Osaka, Japan) with an accuracy of 1 unit. The average of three consecutive durometer measurements was recorded and used to quantify Asker-C heel hardness.
All experimentation took place in a biomechanics laboratory. The original LESS testing and scoring procedures were used,4 except in the barefoot condition when no shoes were worn. Participants jumped horizontally from a 30-cm box to 50% of their body height and jumped vertically as high as possible upon landing. The horizontal landing distance was indicated on the floor using tape. Trials were disregarded when participants did not land at 50% of their body height or did not perform the task in one fluid motion. Feedback on performance was not given to avoid influencing outcomes22 unless the task was performed inappropriately. Before the formal tests, participants were allowed up to three familiarization trials in both the footwear and barefoot conditions immediately before testing for each corresponding condition. For testing, each participant performed three trials in each condition with 30 seconds rest between trials and 15 minutes rest between conditions. The order of conditions was block randomized prior to study commencement by a third party to ensure an equal number of participants starting in each condition. The condition tested first (barefoot or footwear) was allocated sequentially and announced to participants upon study enrollment. It was not possible to blind the participants and examiners to the condition examined.
Two cameras with a focal length of 8.8 to 73.3 mm (35-mm equivalent focal length of 24-200 mm) captured the DLJL trials at 120 frames per second (Sony RX10 II, Sony Corporation, Tokyo, Japan). These videos were used to derive LESS scores post testing. One camera captured frontal plane movement and the other captured right-side sagittal plane movement. Each camera was placed 3.5 meters away from the landing area and mounted on tripods with a 1.3 m lens-to-ground distance. The videos were analyzed using Kinovea (version 0.9.4, www.kinovea.org). The time from take-off from the ground to the final landing was extracted from the sagittal plane videos to compute jump heights from flight times as23:
h= 18 ⋅g⋅t2⋅100
where h is jump height (cm), g is gravitational acceleration constant (9.81 m/s2), and t is flight time (s).
Data processing
A single rater (CBS) with over three years of experience analyzing human movement conducted all data processing after receiving four training sessions from an expert LESS rater (IH) who had completed over 400 LESS evaluations. The single rater completed more than 20 LESS assessments before analyzing the current dataset. After analyzing all videos for this study (i.e., 80 participants x 3 trials x 2 conditions = 480 videos), the rater re-analyzed the first 20 to ensure consistency in ratings. The rater was blinded to the randomization sequence and LESS scores of individuals from the other experimental condition, as trials were presented in a random order for rating.
To ensure rater reliability of the videos collected, two raters (CBS and DB) with similar experience and LESS training participated in an inter-rater and intra-rater reliability study of the overall LESS score using a subset of videos from 10 participants. Inter-rater reliability was excellent based on intra-class correlation coefficient (ICC) and 95% confidence interval [lower, upper] values for both footwear (ICC(2,1) = 0.957 [0.815, 0.990]) and barefoot (ICC(2,1) = 0.957 [0.847, 0.989]) conditions. Intra-rater reliability was also excellent for both footwear (ICC(3,1) = 0.974 [0.903, 0.993]) and barefoot (ICC(3,1) = 0.970 [0.815, 0.993]) conditions.
Statistical analysis
The effect of footwear on group mean LESS scores, injury risk categorization (high risk, LESS ≥ 5 errors; low risk, LESS < 5 errors), individual-level risk categorization, and jump height was examined. The average of participants’ three trials was used for analysis. Taking the average of three trials is consistent with the original LESS protocol4 and is the most common approach used to interpret LESS data.10 Differences in group mean LESS scores and jump heights between conditions were assessed using mean differences, two tailed paired t-tests, and Cohen’s d effect sizes for paired samples using an average variance with 95% confidence intervals. Cohen’s d effect sizes were considered small, medium, and large when reaching 0.20, 0.50, and 0.80, respectively, and trivial when less than 0.20.24
Differences in the number of participants categorized at high and low risk of injury based on the 5-error LESS threshold between conditions were assessed using McNemar’s tests and odds ratio with 95% confidence intervals. The odds ratio reflects the number of participants exclusively at high risk in the footwear condition versus those exclusively at high risk in the barefoot condition. Hence, odds ratios>1.0 reflect a higher proportion of at-risk individuals in the footwear condition. The number of participants demonstrating a clinically meaningful change in LESS scores (i.e., one error or more difference)4,8 between conditions was also examined. Finally, differences in the occurrence of specific LESS errors between conditions were explored using McNemar’s tests. For each participant, an error was considered present when present in two of the three trials for Items 1-15. For Items 16-17, an error was considered present when the ‘average’ rating was present in two of three trials or when the ‘poor/stiff’ rating was present in one of three trials.4,9 The significance level was set at p≤0.05 for all analyses, which were conducted using Microsoft Excel for Microsoft 365 MSO (version 2109, Microsoft Corp, Redmond, WA, USA) and RStudio® version 1.1.463 with R version 4.0.5 (R Core Team, 2021). There were no missing data, and all participants completed the experimentation without harm.
RESULTS
Eighty participants (44 males and 36 females) completed the study. Their demographic and footwear characteristics are presented in Table 1. Approximately half of participants (52.5%) participated in court or field sports (e.g., basketball, football, netball, rugby), with most of the others (42.5%) participating in another sporting activity (e.g., running, cycling, rowing).
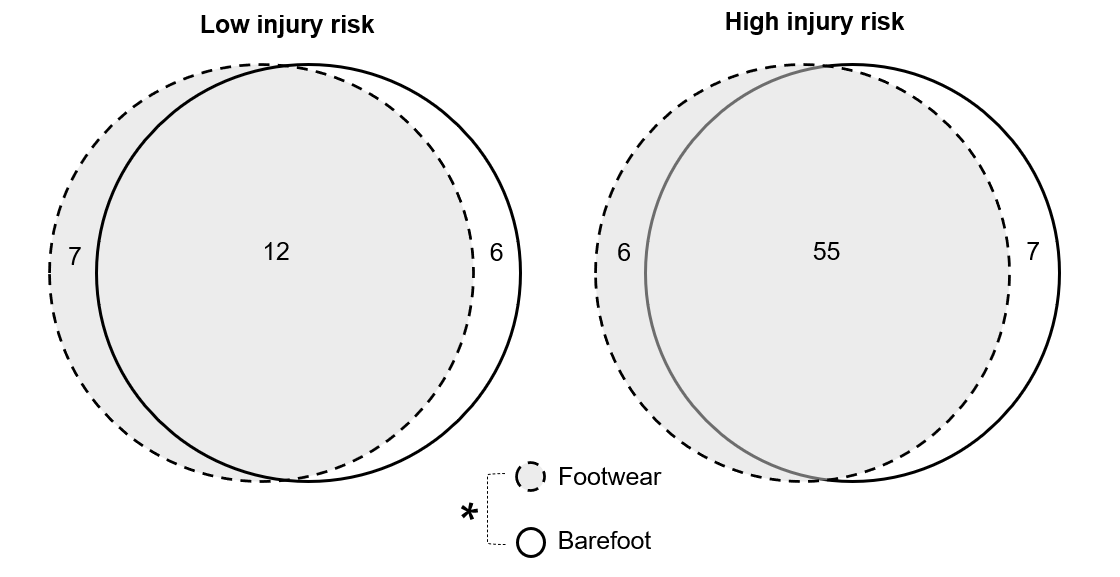
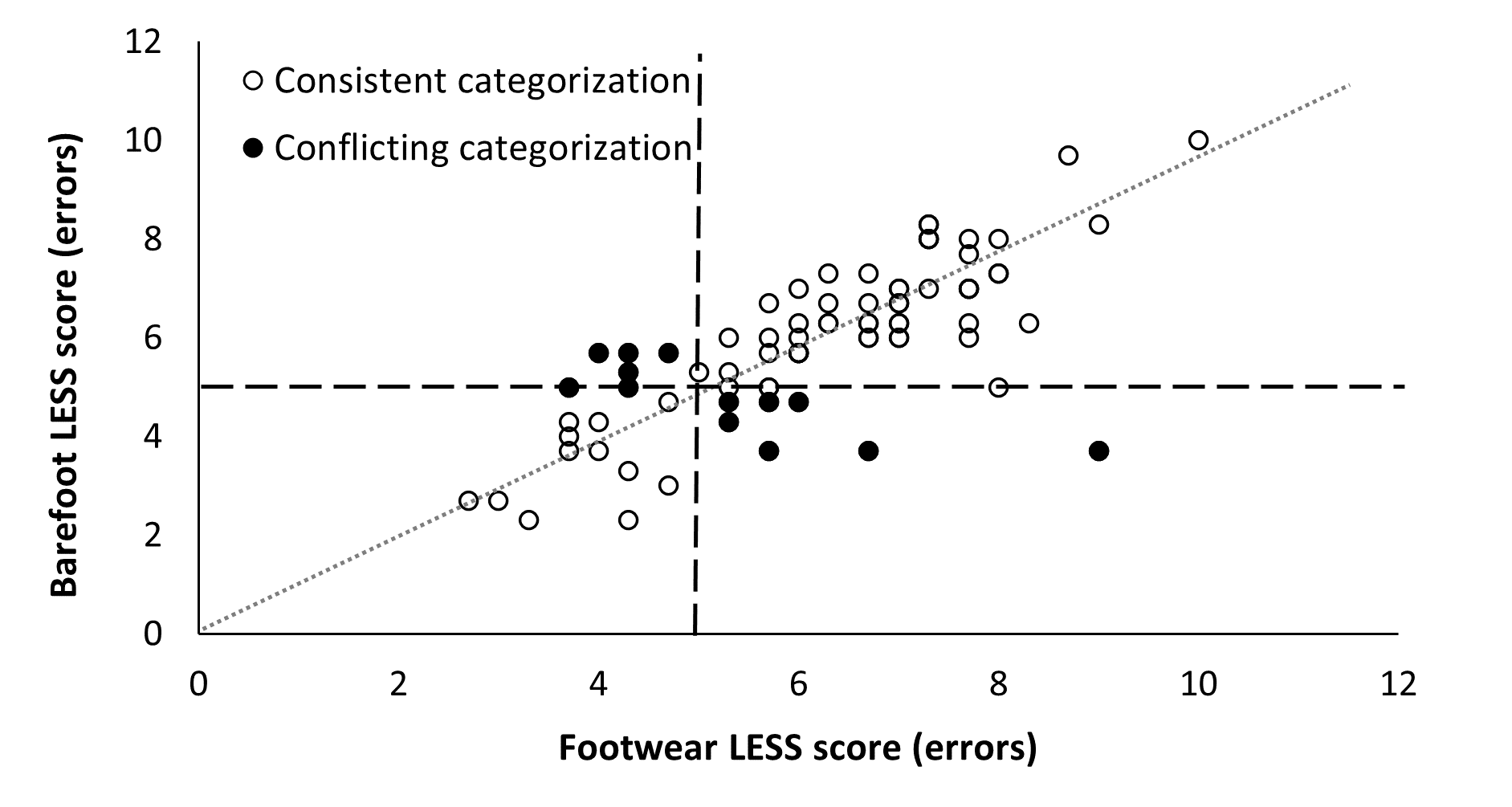
The group mean LESS scores in the footwear condition (range: 2.7-10.0 errors) was significantly greater (0.3 errors, p=0.022) than barefoot (range: 2.3-10.0 errors), as shown in Table 2. However, the magnitude of the difference was trivial (Cohen d=0.18 [0.03, 0.33]). The number of individuals classified at high risk was not significantly different between conditions (62 participants footwear vs 61 participants barefoot, p=1.000), with seven participants categorized at high risk exclusively in footwear and six barefoot (Figure 1). At an individual level, 27 participants (33.8%) demonstrated a clinically meaningful difference of one error or more in LESS scores between conditions. The risk categorization was conflicting between conditions for 13 participants (16.3%, Figure 2). Six participants changed from being categorized as low risk in footwear to high risk barefoot, and seven from high risk in footwear to low risk barefoot. The difference in mean LESS score was one or more in all but one of these participants (92.3%). Jump height in footwear (range: 8.5-56.4 cm) was significantly lower (-0.6 cm, p=0.029) than barefoot (range: 11.4-55.1 cm), but the difference was trivial (d = -0.07 [-0.13. -0.01], Table 2).
_and_low_(__5_errors)_injury_ri.png)
_score_plots_for_both_footwear_and_barefoot_conditions_.png)
The occurrence of specific LESS errors significantly differed between conditions for four of the 17 items. Specifically, there were more errors for Item 4 (ankle plantar flexion at initial contact) and Item 5 (knee valgus at initial contact) in footwear, and more errors for Item 8 (stance width-narrow) and Item 10 (foot position-toe out) barefoot (Table 3).
DISCUSSION
In agreement with the hypothesis, footwear led to significantly higher LESS scores than barefoot; however, the difference was trivial and not clinically meaningful as it was less than one error.4,8 Footwear led to significantly lower jump heights than barefoot, but the difference was also trivial and not clinically meaningful as it was less than the 2 cm typical error associated with this measure.25 A greater number of participants at high risk of injury when wearing footwear was hypothesized; however, the number of high injury-risk participants was not significantly different to barefoot. Despite the similarities in LESS scores and high injury-risk categorization at a group level, differences in LESS scores were clinically meaningful (i.e., one error or more) for approximately one third of participants, and individual-level risk categorization was inconsistent for approximately a sixth of participants between conditions. Furthermore, differences in specific landing errors were noted, with greater odds of knee valgus and heel-to-toe or flat foot landing at initial contact in footwear, and lesser odds of landing with a narrow stance width and toe-out foot position. Overall, performing the LESS with compared to without footwear led to comparable mean LESS scores, group-level injury risk categorization, and jump heights, but influenced specific LESS errors, individual-level risk categorization (i.e., 16.3% of individuals inconsistently categorized between conditions), and LESS scores of some participants in a clinically meaningful manner (i.e., change of one error or more for 33.8% of individuals).
The mean LESS scores in footwear in this study are similar to means reported elsewhere for similar cohorts of young active individuals.9,10 The current findings also reflect previous ones where altering the jump landing distance of the LESS did not meaningfully affect group-level LESS scores and risk categorization, but significantly influenced the odds of individual LESS errors and individual-level injury risk categorization.9 The comparable outcomes imply that studies can implement the LESS either with shoes or barefoot when the main outcome is the group mean LESS score or group-level injury risk categorization. Implementing the LESS barefoot can be easier to standardize across participants as guarantees no effect of footwear or footwear type on landing mechanics. Nonetheless, it would be inappropriate to compare specific LESS errors between studies or infer similar risk of injury at an individual level between conditions. For instance, O’Malley, Murphy performed the LESS barefoot.14 Their results would likely be comparable if performed with shoes in terms of the group mean LESS score and proportion of high injury-risk individuals, but the individual-level risk categorization might differ. Furthermore, the predictive value of the LESS performed barefoot for noncontact ACL injury has not been researched. Hence, when using the LESS in a clinical setting, test parameters should be kept constant for a given individual on separate occasions and the use of footwear is recommended given that it has demonstrated predictive value in youth.5 Most ACL injuries that occur during sports and recreational activities probably involve individuals wearing their own athletic footwear; hence, performing the LESS with shoes is arguably more ecologically valid.
In biomechanics research, relying solely on null hypothesis significance testing without use of appropriate effect sizes or consideration of the magnitude of the difference is discouraged.26 It has been proposed that a one error change in LESS score is clinically meaningful.4,8 In fact, the inter-session standard error of measurement for the LESS is 0.81 error,27 which exceeds the observed difference of 0.3 errors between footwear and barefoot conditions. Hence, although the difference between conditions reached statistical significance, the effect of footwear on overall mean LESS scores is not clinically meaningful. Despite this, differences of one error or more were observed in 33.8% of individuals and changes in injury risk categorization in 16.3% of individuals between footwear and barefoot conditions, again supporting use of a consistent footwear or barefoot protocol for a given individual when assessing injury risk or movement strategies over time.
The odds of errors significantly differed between footwear and barefoot conditions for four LESS items: knee valgus, ankle plantar flexion, narrow stance width, and toe-out foot position at initial contact (Items 4, 5, 8, and 10). The two first errors were 12.5% more prevalent in footwear, whereas the latter two were 8.7% and 17.5% less prevalent. Arguably, though, differences less than 10% are likely trivial in nature (i.e., narrow stance width).28 Hanzlíková and Hébert-Losier9 also found that these specific LESS errors differed between self-selected and 50% body height landing conditions, alongside knee valgus displacement (Item 15). Furthermore, review of the running literature indicate that footwear influences knee, ankle, and stride kinematics.19 A heel-to-toe drop of zero, for instance, is more commonly associated with a forefoot strike pattern in running studies compared to running in footwear with a drop of 8 mm or more.29 These findings combined suggest these specific LESS errors (Items 4, 5, 8, and 10) are more sensitive to change and alterations in protocol and footwear than the other errors. The differences in likelihood of specific LESS errors between footwear and barefoot conditions indicate differences in multi-joint strategies used to moderate impact forces during landing tasks, as shown elsewhere.11 Barefoot, participants were more likely to land with greater ankle plantar flexion and the front part of their foot. These observations are comparable to findings of a more plantar-flexed ankle and greater foot-ground angle at initial contact from a 30-cm DLJL task similar to the LESS when performed barefoot compared to with shoes.12 Landing in greater ankle plantar flexion during DLJL likely shifts loading between joints, with greater ankle but lesser knee joint loading. Indeed, participants with an ACL reconstruction landed from a 60-cm drop with greater ankle plantar flexion and absorbed a greater amount of force at the ankle compared to non-injured controls, presumably to protect their injured knee.30 Furthermore, research also indicates that single-leg landing with greater ankle plantar flexion from a drop jump increases total energy dissipation and reduces peak vertical loading rates.31 Since landing in greater plantar flexion may reduce the risk of knee and hip injuries, DLJL barefoot may be considered as a training tool in the early stages of ACL injury rehabilitation to reduce knee loads and peak vertical loading rates. In addition, our data indicate that maximal jump performance is not compromised barefoot, which is often of concern to coaches, clinicians, and athletes.
Although knee valgus at initial contact was one of the most frequent errors in both footwear and barefoot conditions, this error was 12.5% more prevalent in footwear. Previous research has identified knee valgus as a risk factor for ACL injury.32,33 Hewett, Myer tracked 205 female adolescent athletes over 13 months: nine sustained ACL injuries.32 These nine athletes all exhibited increased knee valgus when performing drop vertical jumps pre-injury. Therefore, this metric alone in the context of the LESS might suggest an increased ACL injury risk when wearing footwear compared to barefoot. However, knee valgus alone does not cause ACL injury.1 ACL injuries are moreover linked with multi-planar mechanisms,3 often with a hyperextended of slightly flexed knee undergoing a valgus motion with either internal or external rotation.34 Despite overt methodological limitations,35 more recent research continues to challenge that knee valgus during drop jumps is a valid predictor of ACL injury, with no association between 2D frontal plane knee and hip motion during drop jumps and noncontact ACL injuries.36
In the current study, a threshold of five or more errors was used to categorize participants at high injury risk based on previous research.5 However, the predictive value of the LESS is debated in research given other studies indicating a lack of association between LESS scores and noncontact ACL injury.37 Noteworthy is that in these two studies,5,37 photographs of participants suggest performance of the LESS in shoes in one study5 and barefoot in the other,37 which might have influenced LESS scores at an individual level. The five-error threshold may be appropriate in footwear only. Furthermore, there is no population-specific LESS cut-off score established in the literature. For instance, there is a tendency in the literature for higher LESS scores in younger individuals.8 Hence, it remains to confirm whether the five-error threshold established from youth elite soccer players (age: 13.9 ± 1.8 y)5 apply to young active adults like those in the current study (age: 20.0 ± 2.3 y) in whom the LESS is often used.6,9,10,14,27,37 The mean LESS scores in this study are within the range of those reported for non-injured active young adults across the scientific literature.8 Nonetheless, over 75% of participants were categorized as high risk, which could reflect the inappropriateness of the 5-error threshold in this cohort or the fact that most participants were not involved in jump-landing sports. Non-contact ACL injuries are multifactorial in nature, with the LESS examining gross movement patterns only. It is also worth noting that a series of studies suggest that the vertical drop jump and DLJL tasks are poor predictors of future ACL injury.38–40 Out of five biomechanical variables examined across these studies (knee valgus angle at initial contact, peak knee abduction moment, peak knee flexion angle, peak vertical ground reaction force, and medial knee displacement), only medial knee displacement during the drop vertical jump was linked to ACL injuries prospectively, but sensitivity (0.6) and specificity (0.6) were poor.38 In recent investigations, the ability to control the knees in the frontal plane during landing from a DLJL was unable to distinguish between athletes who sustained an ACL injury to those who remained uninjured.40 Despite these findings, DLJL tasks can still be useful as part of neuromuscular training programs for reducing ACL injury incidence41 and guiding rehabilitation or return-to-sport decision making post ACL reconstruction.6,42 The LESS can also be useful for monitoring the effectiveness of programs and changes in biomechanical patterns.43 Performing the DLJL in footwear and barefoot likely involves different multi-joint strategies, loads, and muscle recruitment and activation patterns, which might ultimately lead to different adaptations. As such, performing DLJL tasks in both footwear and barefoot within neuromuscular training programs could provide different stimuli to individuals. Given that participants wearing minimal footwear were excluded, the generalization of the current findings comparing DLJL measures between barefoot and different types of footwear needs confirmation.
CONCLUSION
Overall LESS scores were significantly greater and jump heights were significantly lower in footwear than barefoot, but differences were trivial and not clinically meaningful. At the group level, the proportion of participants categorized at high risk of injury was comparable between conditions; however, differences in specific landing errors, inconsistency in injury risk categorization, and clinically meaningful changes in LESS scores at an individual level were noted. In clinical settings or for screening purposes, performing the LESS with shoes is still recommended given that the predictive value of the LESS barefoot has not been established. If the DLJL is used in neuromuscular training programs, performing the task both with and without shoes can offer variety in landing strategies and potentially different stimuli and neuromuscular adaptations to individuals.
Conflicts of interest statement
The authors report no conflicts of interest.
DATA AVAILABILITY
The data that support the findings of this study are openly available in OSF at https://doi.org/10.17605/OSF.IO/KHS7V.44
Acknowledgments
The authors thank Dr. Shannon O’Donnell and Mr. Dalton Berry for their assistance during the data collection process. The authors also thank the participants for their voluntary participation.