
INTRODUCTION
Elbow injuries in general, and ulnar collateral ligament (UCL) injuries in particular, have become an increasing problem in baseball.1 Over the last 25 years the predominant injury in major league baseball (MLB) has shifted from the shoulder to the elbow.1 The vast majority of UCL injuries are seen in pitchers at both the professional and collegiate level.2
The muscles of the flexor pronator mass can provide dynamic stability to the medial elbow.3–7 Specifically, the flexor carpi ulnaris (FCU) and the flexor digitorum superficialis (FDS) have been shown to provide dynamic stability, with a lesser contribution from the pronator teres (PT).3,6,7 In line with these findings,3,6,7 exercise-induced wrist flexion fatigue has been shown to increase medial elbow gapping under valgus stress.5 The FDS and FCU are highly active during the acceleration and deceleration phases of the pitching motion8 (FDS 80%-71% MVC, FCU112%-77% MVC) and likely provide dynamic elbow stability. In support of this, FCU and FDS elasticity have been shown to increase after repeated pitches and the change was correlated with an increase in medial elbow joint space.9
In response to the increased prevalence of elbow injuries in baseball there has been increased interest in measuring the stress in the medial elbow during pitching. To this end, a wearable inertial sensor has been developed to quantify medial elbow torque during pitching.10,11 Medial elbow valgus torque, an index of valgus stress on the elbow, was shown to be higher for fastballs and changeups compared with curveballs.11 Additionally, valgus torque increased in later innings of a simulated game, despite a decline in pitch velocity, and this effect was attributed to fatigue.11 However, the association between valgus torque at the elbow during pitching and muscle fatigue in the dynamic stabilizers of the elbow has not been previously examined. It is possible that pitchers with high valgus torque during pitching experience greater fatigue in the dynamic stabilizers of the elbow and thus are at increased risk of injury.
The first step in studying a possible relationship between high valgus elbow torque during pitching and excessive fatigue in the dynamic stabilizers of the elbow is to develop a strength test for the dynamic stabilizers. Previous work in college pitchers has shown that grip strength is minimally impaired post game12 or the next day.13 It remains unclear whether grip strength is a good indicator of fatigue in the stabilizers of the medial elbow. Developing a strength test specific to the FCU and FDS could provide important information on dynamic stability of the medial elbow in pitchers. Middle finger extension strength measured with a hand-held dynamometer has been shown to provide a good measure of impairment in patients with lateral elbow tendinopathy.14 Applying the same methodology to finger flexion strength might provide an indicator of medial elbow function.
Therefore, the purposes of this study were twofold: (1) initially determine if finger flexion strength testing with a hand-held dynamometer selectively activates the FCU and FDS, (2) determine if baseball pitchers with higher valgus elbow torque experience greater FCU and FDS strength loss. It was hypothesized (1) that the FCU and FDS would be preferentially activated during middle and ring finger flexion MVC testing, and (2) that pitchers with higher elbow valgus torque would experience greater finger flexion fatigue and slower recovery.
MATERIALS AND METHODS
This study was divided into two sections: (1) a pilot study in healthy control subjects to develop FCU and FDS strength tests and (2) and a field study in college baseball pitchers to examine fatigue in the FCU, FDS and grip tests and the relationship to valgus elbow torque during pitching. The pilot study and the field study were approved by institutional review board and all participants gave written informed consent.
Pilot Study: Development of FCU and FDS Strength Tests
Electromyograms (EMG) were recorded from the FCU, FDS and PT during manual muscle testing of middle finger and ring finger flexion strength on the dominant side in 10 healthy men (age 36±12 yr) using a 16-channel BTS FREEEMG 300 system, CMRR: >110 dB at 50–60 Hz; input impedance: >10 GΩ (BTS Bioengineering, Milan, Italy). After the skin of each participant was shaved, cleaned, and lightly abraded, disposable silver/ silver chloride passive dual electrodes (2.0-cm interelectrode distance) (Noraxon, Scottsdale, AZ) were applied. Electrodes were placed over muscle belly at the proximal medial forearm (FCU),15 one quarter the distance from medial humeral epicondyle to the skin fold at the wrist (FDS)16 and diagonally over muscle belly, slightly distal to skin fold in cubital fossa (PT).15 Maximum voluntary contraction (MVC) tests were performed for each muscle: maximal resisted wrist flexion and ulnar deviation for FCU testing; maximal resisted four-finger flexion with opposition applied across the middle phalanxes for FDS testing; and maximal resisted forearm pronation with slight elbow flexion for PT.17 Since these MVC tests are not conducive to testing with a hand-held dynamometer for quantifying strength, the middle finger and ring finger flexion tests were chosen for strength testing.
For both the pilot study and field study finger flexion strength was performed with a hand-held dynamometer (Lafayette Instruments, Lafayette, IN). Subjects were seated for testing with the elbow flexed approximately 40°, with the forearm supinated and rested on a flat surface with the wrist in neutral position (Figure 1). The subject stabilized their forearm with their contralateral hand, pressing it firmly against the table while avoiding the surface electrodes. The subject then flexed the test finger (middle or ring finger) while the tester stabilized the other three fingers against the table. Then the tester placed the 1 cm diameter probe of the dynamometer distally on the middle phalanx just proximal to the distal interphalangeal joint. The subject maximally flexed the test finger against the dynamometer while the tester extended the finger (break test). Two trials were performed for each test. A third trial was performed if there was a marked difference between the first two trials (>30%) and subsequently the outlier was discarded and the mean of two was recorded. Index finger flexion break test strength has previously been shown to be reliable.18 Additionally, a hand-held dynamometer test set up has previously been used to detect middle finger extension weakness and treatment training effects in patients with lateral epicondylosis.14
_middle_finger_flexion_strength_test._(b)_ring_finger_flexion_strength_test._the_dynamo.png)
Pilot Study Statistics
Middle versus ring finger strength were compared using a paired t test. Differences in FCU, FDS and PT activation between the middle and ring fingers were compared using Test (middle versus ring finger) by Muscle (FCU, FDS, PT) repeated measures analysis of variance. The dependent variable was EMG expressed as a percentage of MVC. Pairwise comparisons between tests and between fingers were made using the least significant difference approach.
Field Study in Pitchers
Procedures
Middle and ring finger flexion strength and grip strength were measured immediately prior to a game, immediately after the pitcher was removed from the game, and on the day after the game. The study participants were 10 NCAA division 3 baseball pitchers (3 freshmen, 1 sophomore, 2 juniors, 4 seniors; age 21±2 yr, height 1.83±0.06 m, body mass 85.4±9.2 kg). Data were collected during intra-squad scrimmages and preseason games in the Fall season, with 6 pitchers having data from one performance and 4 pitchers having data from two performances (total 14 game data sets). Elbow valgus torque was measured from an inertial measurement unit (Motus Global, Massapequa, NY), housed in a compression sleeve, worn on the elbow during pregame bullpen pitches. The inertial measurement unit was removed prior to the game (the pitchers preferred not to wear the device). The elbow valgus torque from the bullpen pitches was averaged for each pitcher. Pitch velocities were not measured for the games used in this study. However, each player had his fast ball velocity measured earlier in the season which was used during analysis. All participants gave written informed consent, and the study was approved by institutional review board.
Middle and ringer finger flexion strength were measured as described in the methods for the pilot study. Grip strength measurements were taken in a standing position using a hydraulic hand dynamometer (Jamar; Performance Health, Warrenville, IL). Pitchers were instructed to have their shoulder adducted and neutrally rotated, elbow flexed at 90°, and forearm in neutral position during the grip test. Pitchers were instructed to squeeze the dynamometer as hard as they could (isometric test). The average of two trials was recorded and used for data analysis.
The inertial measurement unit was aligned with the medial aspect of the ulna approximately 5 cm distal to the medial epicondyle of the humerus and held in place with a commercial sleeve. In addition to elbow torque (peak elbow valgus torque) the sensor calculates arm slot angle (angle of forearm relative to the ground at ball release), arm speed (peak forearm angular velocity in degrees per second) and shoulder rotation angle (angle between forearm and ground at maximum external rotation). Pitchers were classified as high elbow valgus torque (above the mean for the group) or low elbow valgus torque (below mean for the group).
Field Study Statistics
Pitchers were categorized as having high or low valgus torque (see results section for details). Effect of valgus elbow torque on fatigue and strength recovery was assessed using mixed-model ANOVA. Based on the pilot study, it was estimated that with 14 pitching performances there would be 80% power to detect a 11% change in middle finger strength after a pitching performance (p<0.05). Pearson correlation coefficients and stepwise multiple regression were used to identify factors associated with post game fatigue.
RESULTS
Pilot Study
Finger flexion force was significantly greater for the middle finger test versus the ring finger test (75±17 N vs. 52±9 N, P<0.001). Muscle activations varied significantly between muscles and between tests (Table 1). FDS activity was greater than PT activity for both the middle finger test (p=0.005) and the ring finger test (p=0.002). FCU activity was higher than PT activity for the ring finger test (0.010). Therefore, the finger flexion tests preferentially activated the FDS and FCU over the PT.
Field Study
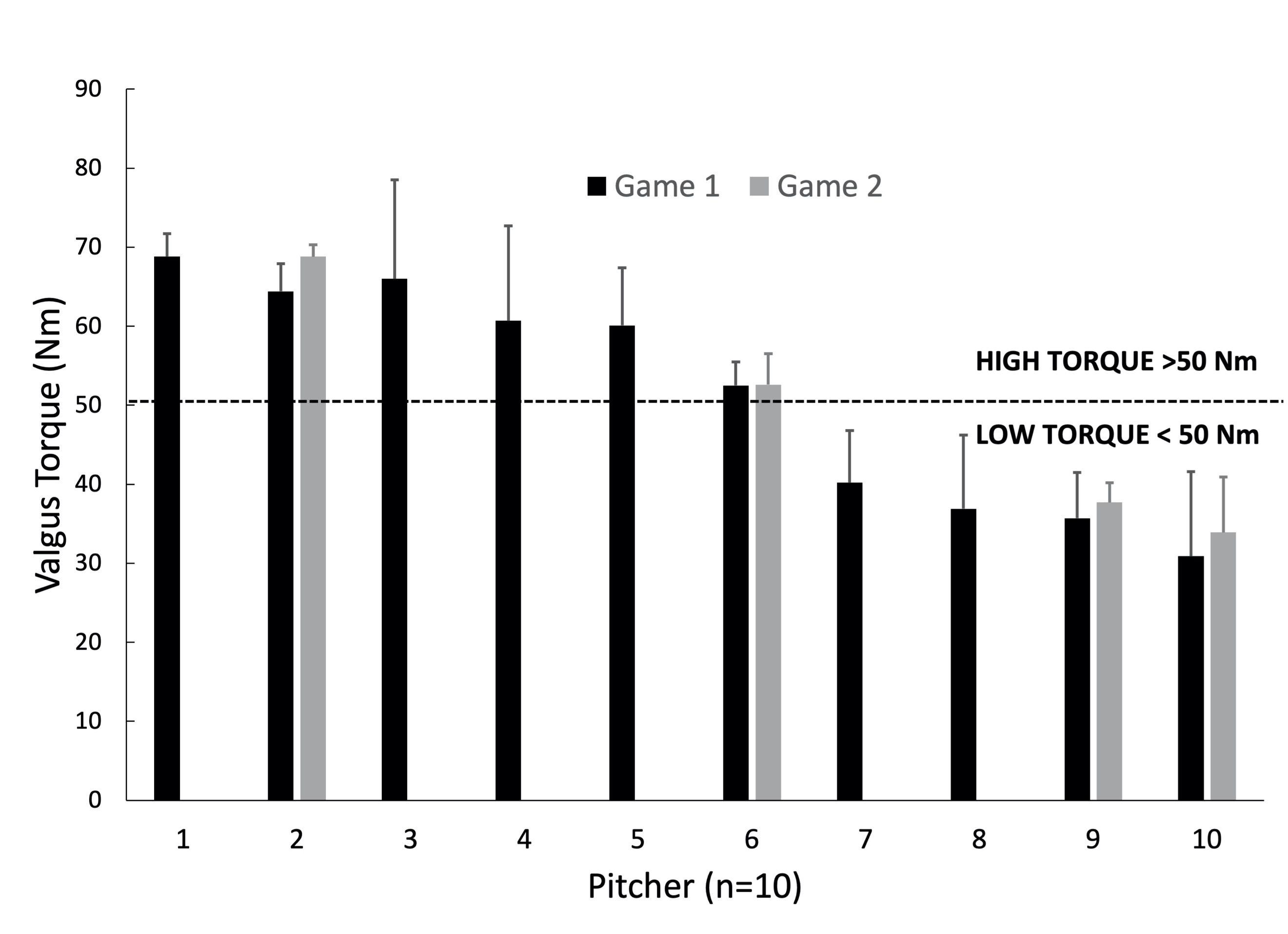
The pitchers threw 58±13 pitches in the 14 games (range 42 to 82 pitches) not including bullpen warm up throws. For the bullpen pitches valgus elbow torque was 50.7±14.3 Nm with an arm slot angle of 48±9°, an arm speed of 912±116°/s and a shoulder rotation angle of 145±10°. The number of bullpen pitches varied between pitchers (range 20-29), but elbow valgus torque for a given pitcher did not vary markedly between pitches, with an average coefficient of variation of 14%. Elbow torque values were very similar between games for the four pitchers with data from two games, varying by 6.6%, 9.3%, 0.2%, and 5.4% (Figure 2).
_or_low_(n_4.jpeg)
Four pitchers (6 games) had elbow torques below 50 Nm (35.9±3.2 Nm, range 30.9-40.2 Nm). Six pitchers (8 games) had elbow torques above 50 Nm (61.7±6.5 Nm, range 52.5-68.8 Nm). The total number of game pitches was not different between the low and high elbow valgus torque groups (53±11 vs 61±13, p=0.263). The high torque group comprised pitchers with higher (p=0.010) pitch velocity (87±2 mph) than the pitchers in the low torque group (82±2 mph).
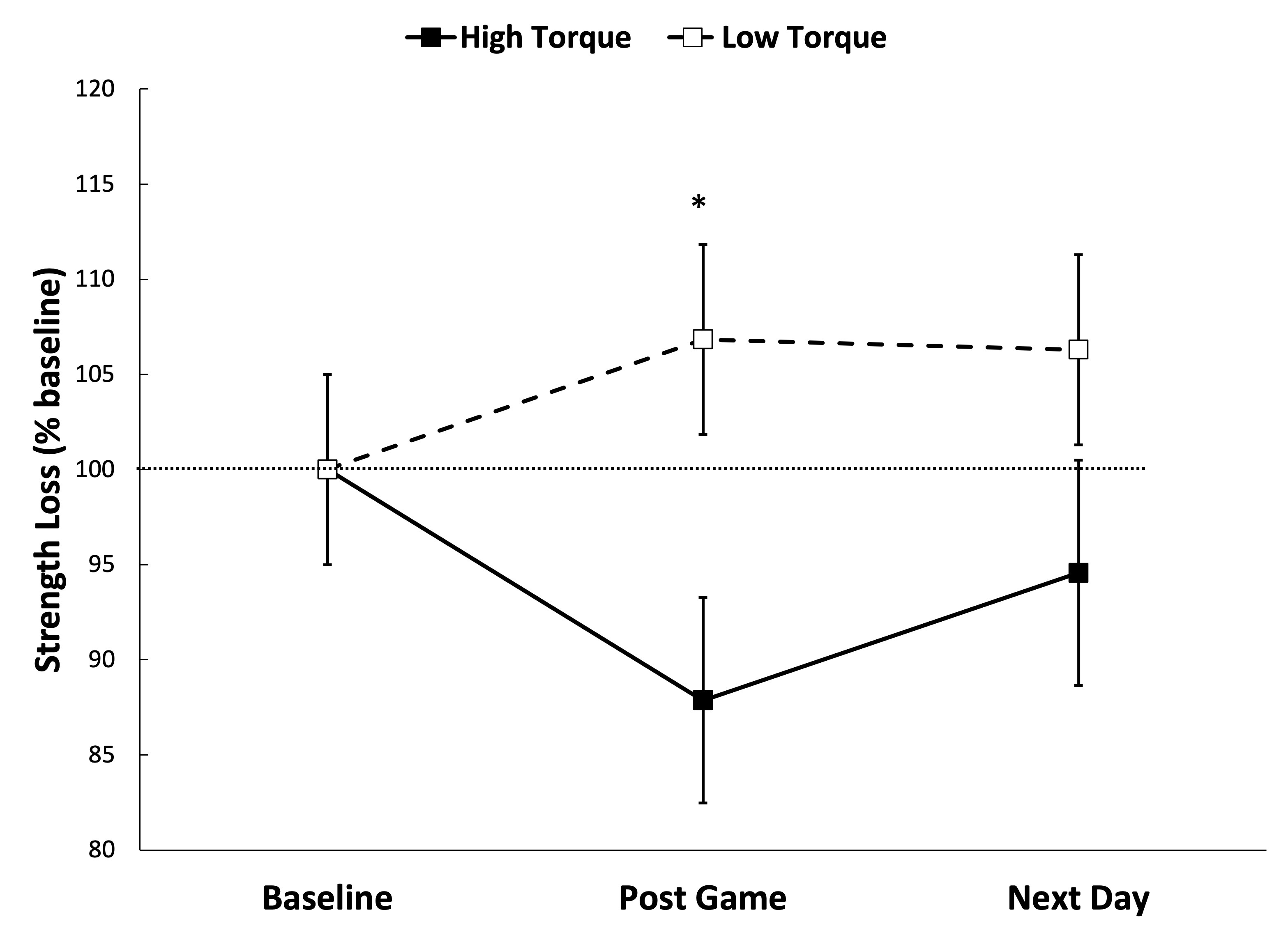
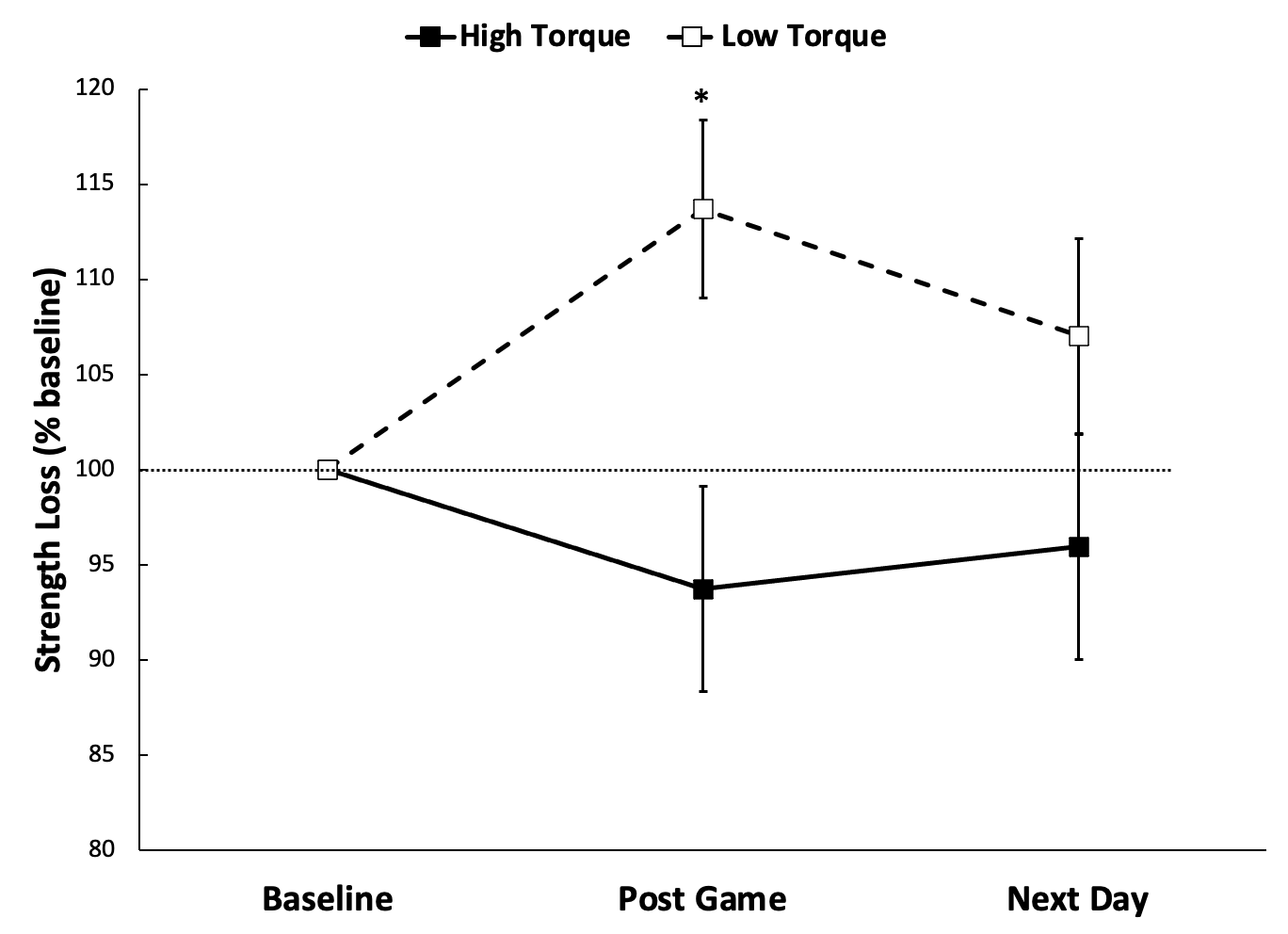
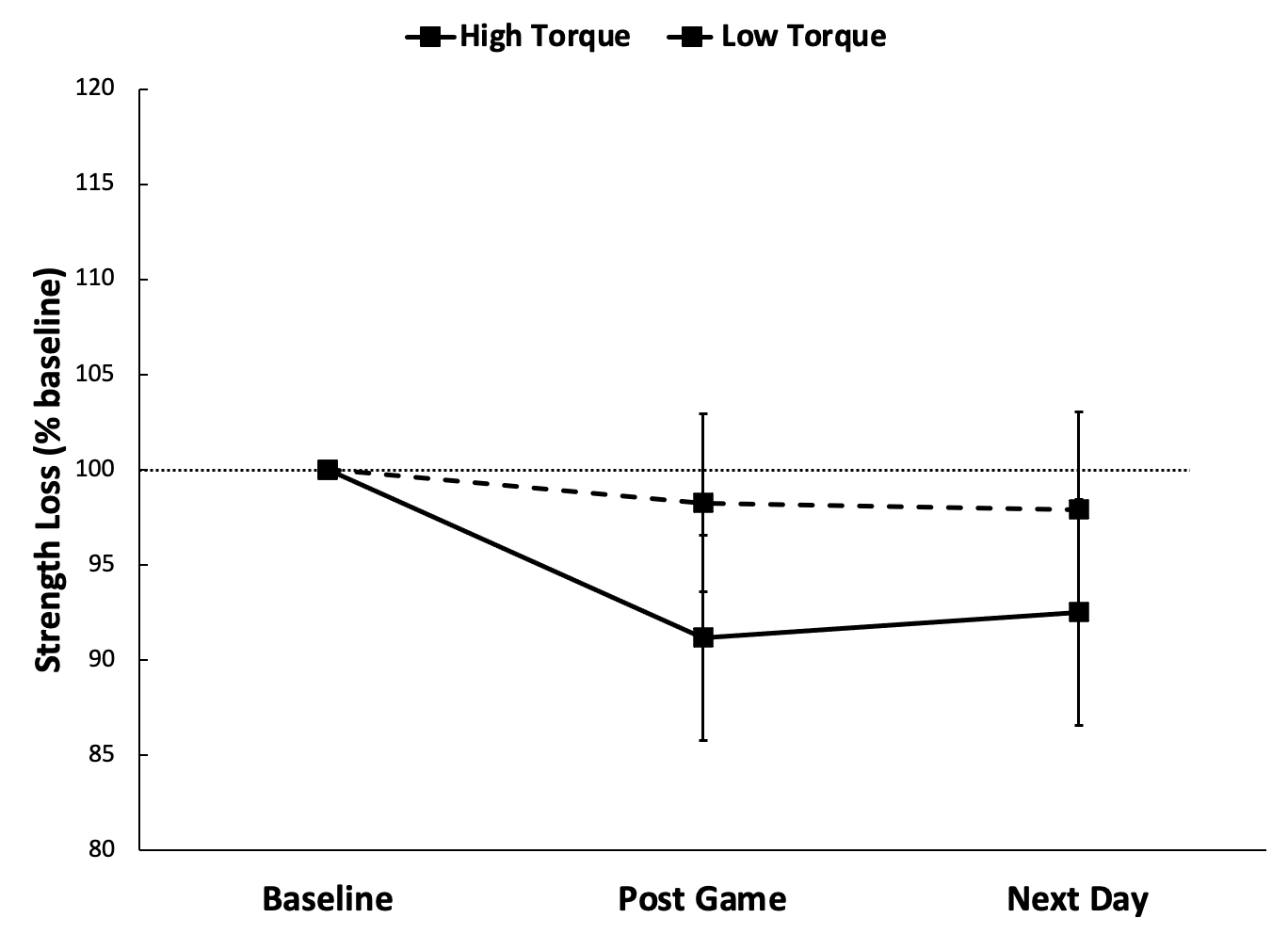
Pregame strength was 77.1±11.3 N for middle finger flexion, 58.5±11.2 N for ring finger flexion and 552±76 N for grip strength. Middle and ring finger flexion fatigue, and subsequent recovery, were worse for pitchers with high valgus elbow torque compared with pitchers with low valgus elbow torque (Group by Time p=0.022 middle finger, Figure 3, p=0.031 ring finger, Figure 4). Pitchers with high torque had greater post-game fatigue than pitchers with low torque for middle finger flexion (88±10% of baseline strength vs. 107±18%, p=0.026) and ring finger flexion (94±13 vs. 114±13%, p=0.016). By contrast, changes in grip strength were unaffected by elbow torque (Group by Time p=0.143, Figure 5).

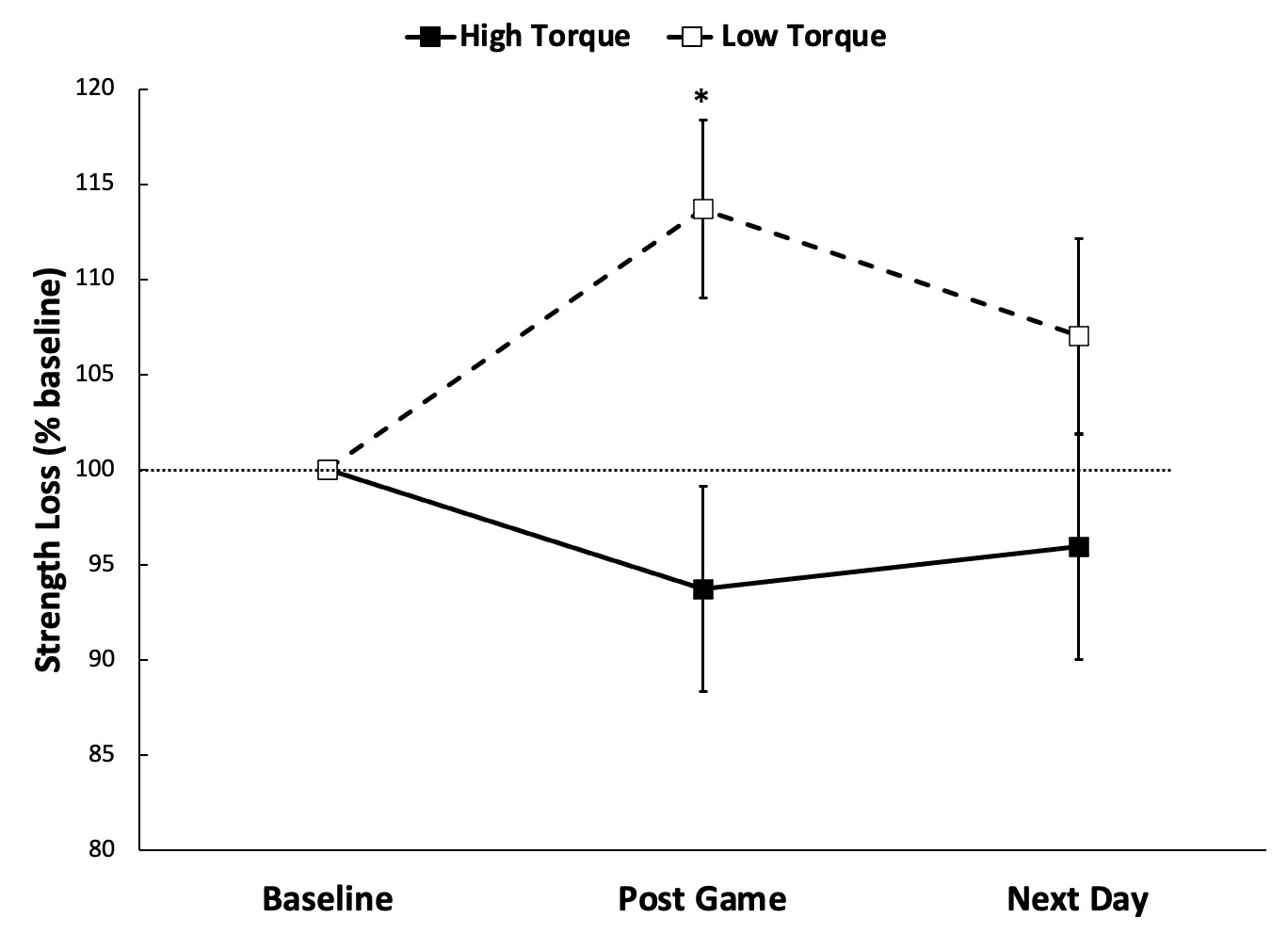
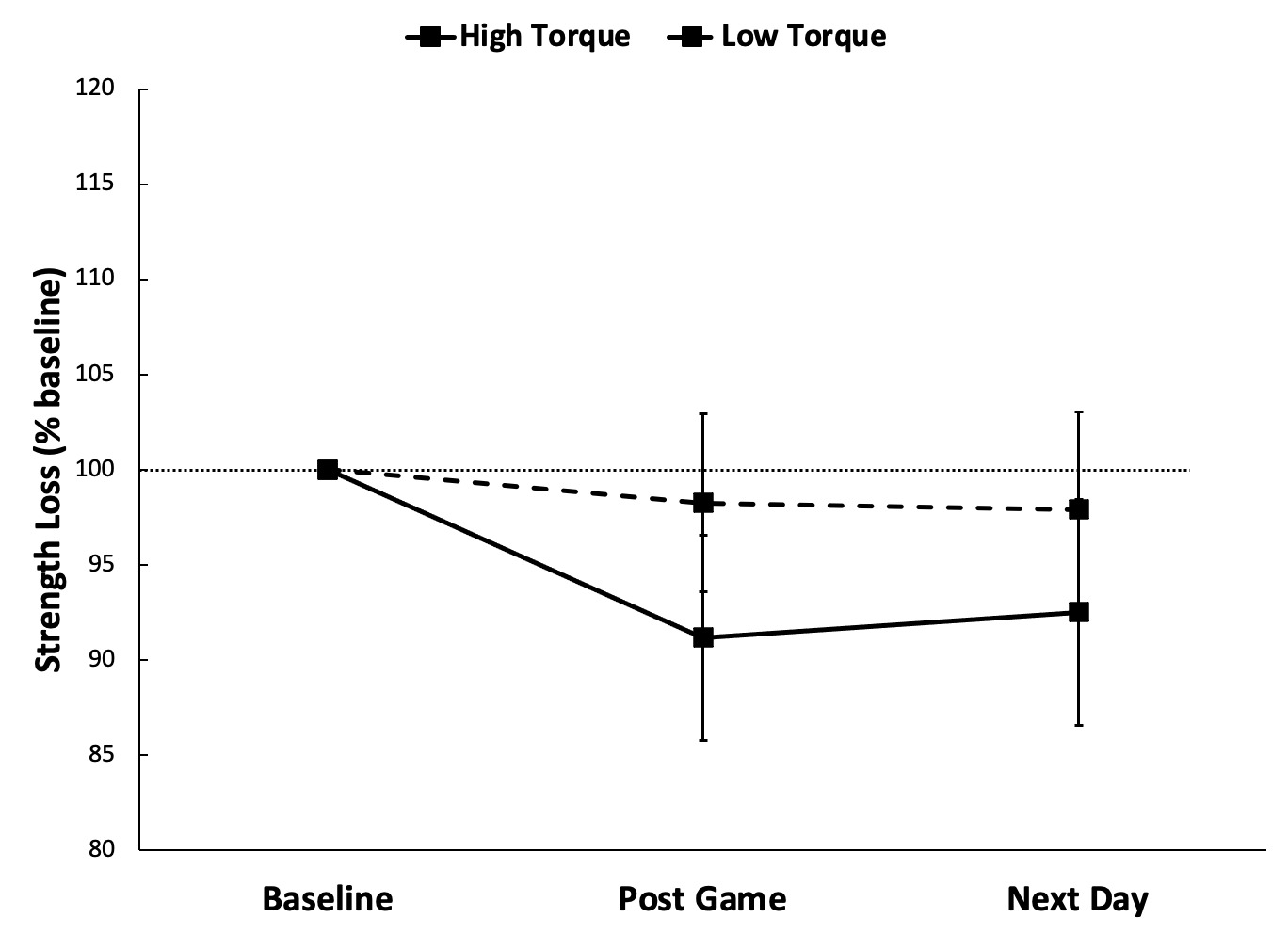
Post-game middle finger flexion fatigue was correlated with the number of pitches thrown (r=0.617, p=0.019) and elbow valgus torque (r=0.597, p=0.024). The combination of pitch count and elbow valgus torque explained 57% of the variance in middle finger flexion fatigue (R=0.755, p=0.010). Post-game ring finger flexion fatigue was correlated with the number of pitches thrown (r=0.552, p=0.041) and elbow valgus torque (r=0.632, p=0.015). The combination of pitch count and elbow valgus torque did not further improve the prediction of ring finger fatigue. Neither pitch count (r=0.058, p=0.845) nor elbow torque (r=0.426, p=0.129) were correlated with grip fatigue.
DISCUSSION
In the pilot study the EMG data from the FCU, FDS and PT indicated that middle and ring finger flexion tests activated the FCU and FDS substantially more than the PT. Previous literature showed that the FCU and FDS provide dynamic stability to the medial elbow.3–7 In the field study pitchers with greater elbow valgus stress during pitching experienced greater fatigue in the finger flexion tests. This indicates that pitchers with high valgus elbow stress place greater demand on the dynamic stabilizers and thus exhibit greater fatigue in these muscles. By contrast, change in grip strength, which is a more general test of forearm fatigue, was unaffected by elbow valgus stress.
It was anticipated that the middle and ring finger flexion tests would activate the FDS since the MVC test for the FDS is resisted four finger flexion. A hand-held dynamometer test of four finger flexion was not attempted because there would be no way to uniformly apply resistance across the four fingers to allow comparable contributions from each finger. Since the FCU tendon inserts on the pisiform and is not attached to the carpal bones, it is surprising that it was so highly active during ring finger flexion. This may reflect synergistic action between finger and wrist flexion and the role of the pisiform. In fact, ring finger flexion has been shown to contribute to medial stability of the elbow.19 However, both middle finger flexion and index finger flexion have been shown to provide greater medial stability that the ring finger.19 Future work should examine index finger strength changes in baseball pitchers.
While the focus of this study was middle and ring finger flexion strength in relation to medial elbow stability, previous work has shown that full grip contraction (mass grasp) can stabilize the medial elbow.20 However, changes in grip strength in the present study were not associated with the valgus torque on the medial elbow during pitching. Therefore, these results support finger flexion strengthening exercises for baseball pitchers as opposed to grip strengthening exercises. Similarly, others have proposed that index and middle finger flexion exercises be added to throwers’ injury prevention training programs.19
Higher pitch velocities are associated with greater valgus torque at the elbow, however, this relationship is more pronounced within pitchers than between pitchers.21 Pitch velocity explained 96% of the variance in elbow torque when looking at individual professional pitchers throwing at a range of different velocities.21 By contrast, pitch velocity only explained 8% of the variability in elbow torque when comparing data across a group of professional pitchers.21 Thus, variation in individual pitchers’ stature, anthropometrics and biomechanics likely contribute markedly to the elbow torque.
The wearable inertial sensor used in this study can provide useful information for monitoring and managing pitchers. Part of the rationale for the study was the finding that valgus elbow torque measured with this sensor increased progressively after three innings of a simulated game despite a decline in pitch velocity.11 This increased medial elbow stress was attributed to fatigue, but the only measure of fatigue was a visual analog scale used to capture the pitcher’s perception of fatigue with each inning pitched. There was clear heterogeneity in valgus elbow torque between the pitchers studied here, and homogeneity between games for pitchers with data from two games. Given the individual nature of valgus torque profiles in pitchers10,11 a prospective study of valgus elbow torque and injury risk across a large sample of pitchers is warranted.
One limitation was the relatively small number of pitches (58±13) thrown by the pitchers in this study. Because the games were intrasquad scrimmages and preseason games, pitchers were scheduled to pitch a set number of innings in each game. Most pitchers were restricted to four innings thus limiting the total number of pitches. Middle and ring finger fatigue were correlated with pitch count. For the middle finger, pitch count and elbow torque combined to explain 57% of the variance in fatigue. For the ring finger elbow torque explain 40% of the variance in fatigue and pitch count explained 30%, but the combination did not further explain the variance.
While the sample size was sufficient to demonstrate an effect of elbow valgus torque on finger flexion fatigue the data should be viewed as preliminary. Data on a greater number of pitchers throwing a greater number of pitches is needed to fully understand the role of elbow valgus torque in fatigue of the dynamic stabilizers of the medial elbow. Additionally, the sample size was insufficient to fully examine recovery of finger flexion strength on the day after the game. The data were equivocal with regards to the role of elbow torque and the extent of recovery.
Ideally pitch velocity would have been measured in the games studied here (instead of at an independent time during the season) since higher velocities are associated with greater elbow valgus torque.21 However, the relationship between fastball velocity and elbow torque was not strong in professional pitchers.21 Furthermore, weighted-ball throwing training was sufficient to increase pitch velocity with no change in elbow torque.22 It remains to be determined whether high elbow valgus torque independent of pitch velocity leads to earlier fatigue of the dynamic stabilizers of the medial elbow. If so, identifying high velocity pitchers that pitch with low valgus elbow torque may be beneficial.
It would have been preferable if the EMG measurements to validate the tests of FCU and FDS function were performed on the baseball pitchers. However, this would have involved significantly more time with the pitchers, who were in season at the time of data collection. The team did not provide additional time to conduct EMG testing on the players. Using a healthy control group in a laboratory setting provided a greater degree of control than would have been possible with the pitchers and was able to confirm the recruitment of key muscles during various tests.
While the results of this study point to the potential utility of finger flexion strength measures in baseball pitchers it is important to establish the reliability of this measure and the degree of tester expertise required to obtain reliable measures. The tester in this study had more than 20 years of experience using this hand-held dynamometer to test baseball pitchers. Had there been substantial measurement variability it would not have been possible to detect the effects of elbow valgus torque on finger flexion strength. However, since this is not a widely used strength test it remains to be seen how useful the measurement is in the hands of other clinicians.
CONCLUSION
The results of this study indicate that pitchers with higher valgus elbow torque during pitching experience greater fatigue in the dynamic stabilizers of the medial elbow. This may lead to excessive stress on the UCL. These pitchers may benefit from finger flexion strength training to maintain dynamic stability of the medial elbow during a pitching performance.
ACKNOWLEDGEMENTS
This study was presented at the IJSPT Research Symposium at the Orthopedic Summit. Dec 11-14, 2021, Las Vegas, NV.
Conflicts of interest
The authors have no conflicts of interest to report.