
INTRODUCTION
The barbell back squat is considered a safe strength training exercise, provided it is performed and progressed in a controlled manner.1–3 However, the squat appears to be associated with injuries in people participating in powerlifting, weightlifting, bodybuilding, and strongman sports.4 In Sweden, 70% of sub-elite powerlifters reported a current injury, and 87% had experienced an injury within the prior 12 months.5 The lumbopelvic region were one of the most frequently injured areas for both sexes, although men appeared to have a slightly higher frequency of lumbopelvic injuries, 42%, compared to 23% for women.5 Also notable was the difference between men and women regarding injuries to other parts of the spine where women had a significantly higher frequency of neck (20%) and thoracic injuries (29%) than men which reported zero (0%) injuries to these parts of the spine.
Numerous authors have discussed the importance of optimal technique for prevention of injuries during the barbell back squat.6–8 With respect to the spine, a correct technique is described as maintaining the spine in an upright position with preservation of its neutral posture while the trunk is held stable without any observation of wavering or displacement in all planes of movement, throughout the entire squat movement6,8 In a neutral posture, where the spine usually has a gentle “S” shape where the lower back has a slight lordotic curve and the thoracic spine a slight kyphotic curve, it is said that axial load is distributed in a balanced way in all movement segments.9 It seems, however, that there is an ongoing discussion about what constitutes correct squat technique for different parts of the body,3,6 though robust evidence in the matter is somewhat lacking. Nevertheless, experts have stated that improper technique in combination with heavy loads may cause back injuries while squatting10 and that flexion (rounding), twisting (rotating), and side bending of the spine are movements that should be avoided to reduce risk of injury risk and improve performance.11 In support of this, previous studies have reported that the ability to maintain the lumbar spine in a neutral position modifies the forces exerted on the body structures12 and that an inability to maintain a neutral position increases the potential to overload spine and soft tissues to the point of injury, especially when repeated over time.6
Previous authors have described the kinetics and kinematics of the squat using video analysis, magnetic tracking devices, or motion capture systems.13–17 However, a growing body of scientific literature has investigated the utility of inertial measurement units (IMUs) to assess exercise technique18 and for monitoring of the spinal alignment during resistance training.19 Inertial measurement units have been validated to electromagnetic based system for measuring 3D spinal ranges of movement and spinal coupled motion measurement20 and are reliable for measuring joint angles during physical activities.21 Further, IMU systems have been shown to provide data that can distinguish between acceptable and aberrant squat techniques and have been shown to be able to identify technique deviations.22
Results from previous studies have shown that the spinal alignment is adjusted during the performance of the squat and that the adjustments may be influenced by sex,15 load,16 lifting phase (i.e. concentric or eccentric phase)15,16 and stance width.15 However, there are several more variables that might influence spinal alignment, for example, one is how proficient the lifter is in the specific movement and so far, no study has evaluated the kinematics in a group of experienced lifters.
Considering that the lumbopelvic region appears to be one of the most injured anatomical locations among powerlifters and weightlifters4,23 and that men and women who powerlift appear to have different injury rates to different part of the spine, it was hypothesized that men and women move, and thereby load, their spine differently when performing the barbell back squat. Therefore, the aims of the present study were to quantify the spinal alignment in the upper (thoracolumbar, T11-L2) and lower (lumbopelvic, L2-S2) lumbar spine during the barbell back squat exercise in male and female lifters. Secondary aims were to compare alignment during the barbell back squat to standing habitual lumbar spine alignment and determine whether male and female lifters differ in these aspects.
METHODS
To quantify lumbar spine alignment IMUs where used to measure three-dimensional angles of the upper lumbar spine (i.e. thoracolumbar) and lower lumbar spine (i.e. lumbopelvic). Spinal alignment was measured in habitual standing and during performance of three repetitions of the barbell back squat with a high load (70% of self-estimated one repetition maximum (RM)).
Participants
Powerlifters and weightlifters were recruited through invitations to powerlifting and weightlifting clubs, respectively, in Umeå, Sweden. Only lifters with ≥two years of strength training experience, without present injuries that could affect squat performance, and with the intent of competing in powerlifting or weightlifting were included. Also, to avoid the risk of IMUs touching each other during the data collection, only lifters whose height was ≥150 cm were included. In order to ensure that eligibility criteria was met, all participants completed a questionnaire. No participant had any recent or previous medical issues which prevented them from participating in the study. They also signed written informed consent form prior to participation. The study was approved by the Regional Ethical Review Board of Umeå, Sweden (Dnr 2014-285-31M).
Procedures
At the day of data collection, participants first answered a questionnaire and thereafter they completed a self-administred warm-up typically consisting of squats with an unloaded barbell progressing to heavy squats. Thereafter, three calibrated IMUs (MPU-9150, InvenSense, San Jose, USA) were affixed with double-sided tape and elastic self-adhesive bandage wraps to their back by the test leader at processus spinosus T11 and L2, and Sacrum (S2). Thereafter, the lifters completed one further set of warm-up bodyweight squats before data collection while the test leader ensured that the IMUs were set firmly and did not hinder squat performance. The lifters, who were wearing their preferred shoes, were then instructed to assume their habitual standing posture with their arms at their sides while looking straight ahead. Habitual spinal posture (habitual posture) was measured using the IMUs in this position. Thereafter, spinal alignment was registered during the squat. The lifters were asked to perform one set of three repetitions at 70% 1RM. Weight plates of official measures were attached to each end of a powerlifting barbell and the weight was adjusted to the nearest 2.5 kg. After receiving a start signal, the lifters were instructed to descend by flexing at the hip, knee and ankle joints until the crease of the hip was lower than the top of the knee.24 From the bottom position, the lifters ascended to the start position by extending the same joints. They stayed in this erect position and waited for a new signal before beginning the descent of the next repetition. No equipment other than wrist wraps was allowed.
Instruments and measurements
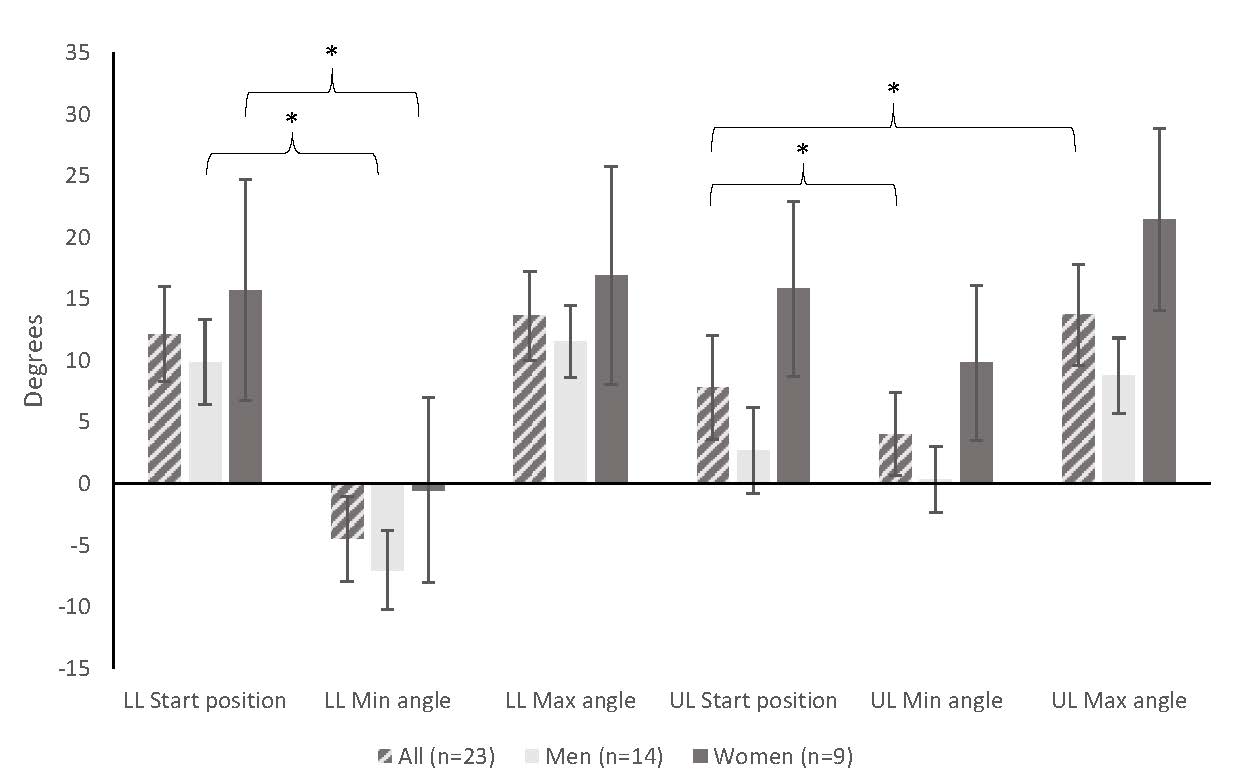
The spinal alignment (degrees) was measured during habitual posture in standing and during execution of the squat exercise. The IMUs recorded their position in all three planes of movement relative to each other and thus measured the three-dimensional angles of the upper lumbar spine (i.e. thoracolumbar spine, T11-L2) and lower lumbar spine (i.e lumbopelvic spine, L2-S2). A positive sagittal plane value indicated a lordotic spinal alignment and negative sagittal plane value indicated a kyphotic spinal alignment. A positive value in the frontal and horizontal plane indicated a right lateral flexion or rotation, respectively. A negative value in the frontal and horizontal plane indicated a left lateral flexion or rotation, respectively.
During the squat, four measures were selected to quantify spinal alignment: First, start position (the lifters standing erect with the barbell held across the back), second, min angle (the minimum angle, at any time during the squat, of the respective lumbar region in degrees), third, max angle (the maximum angle, at any time during the squat, of the respective lumbar region in degrees), and fourth, range of motion (ROM) between the minimum and maximum angles of the respective lumbar regions. The mean value of the three repetitions were used for data analysis for all variables.
The IMUs have a size of length 60 x width 45 x height 10 mm and weigh 14 g each and the IMUs communicated with a laptop via WiFi and had a sampling frequency of 100 Hz, a 16-bit resolution and an anti-aliasing low pass filter set at 50 Hz. The full-scale range was ±1000 °/s for the gyroscopes, ±8 g for the accelerometers and ±4800 µT for the magnetometers. Using three axis gyros and three axis accelerometers, the IMUs detected three-dimensional spinal alignment and real-time orientation was calculated using a customised system MoLabTM POSE (AnyMo AB, Umeå, Sweden).25
Data handling and statistical analyses
Orientation data (i.e., segment angles) from the IMUs were processed in Matlab (version 7.10.0 (R2010a), The MathWorks, Inc., USA). The Euler sequence used for the segment angles were X (rotations in the sagittal plane), Y (rotations in the frontal plane), and Z (rotations in the transverse plane). To each segment, a caudally and adjacent segment was selected as a reference in the calculation of joint angles. All orientation data was low-pass filtered offline with a second order Butterworth filter at a cut-off frequency of 10 Hz. The filter coeffcient was set to 10 Hz as human gross motion selldom contains frequencies above 10 Hz.26 A more detailed description of the used algorithms can be found in Öhberg et al.25 Inter- and intra-tester reliability has been estimated in a previous study showing higher intra-tester reliability.27
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 23 (IBM Corp., Armonk, NY, USA). A factorial repeated measures analysis of variance (mixed ANOVA) was conducted to compare the influence of the independent variables (group: 1=men and 2=women) and the effect of the dependent variable (segment angle at four different positions (1=habitual posture, 2=start position, 3=min angle at any timepoint, and 4=max angle at any timepoint)) using the mean values for the three repetitions. Sphericity was calculated using Mauchly’s test of Sphericity. If sphericity was was not assumed, a correction was made using the Greenhouse-Geisser estimation. If significant position x group effects were found, the results were also presented separately for male and female lifters. If significant within-subjects effects were found, post-hoc pairwise comparisons were calculated. Partial eta squared (η2p) was calculated for effect size, using 0.01, 0.06 and 0.14 to indicate small, medium and large effects respectively.28 Significance level was set at 0.05 and Bonferroni corrections were performed for multiple comparisons.
RESULTS
Background characteristics for participants are presented in Table 1. Comparisons between male and female lifters showed that male lifters were significantly taller and heavier, had more resistance training experience and were stronger (Independent samples t-test, p<0.05) than the female lifters. There was no significant difference between male and female lifters for age. The lifters (n=23) reported current injuries (i.e., pain and impaired ability to perform the squat or deadlift exercises) of the lumbopelvic region (n=2), hip (n=3), knee (n=2) and shoulder (n=2).
The spinal alignment of the upper lumbar spine during standing habitual posture, and during the squats for the start position, minimum and maximum angle, and range of motion are presented in Table 2. For the upper lumbar spine, there were no differences between male and female lifters in spinal alignment (group x position interaction in the sagittal plane (F[1.6, 32.8] = 1.2, p = 0.309), frontal plane (F[1.7, 35.4] = 1.61, p = 0.217), or horizontal plane (F[1.9, 39.3] = 0.14, p = 0.860). In all participants their sagittal plane spinal alignment in standing habitual posture differed from the alignment at the start position and spinal adjustments were made in all three movement planes during the squat (significant main effect for position in the sagittal plane (F[1.6, 32.8] = 51.6, p < 0.001, η2p = 0.711), frontal plane (F[1.7, 35.4] = 21.27, p < 0.001, η2p = 0.503), and horizontal plane (F[1.9, 39.3] = 22.10, p < 0.001, η2p = 0.513). All three statistically significant comparisons for the upper lumbar spine had large effect sizes (η2p > 0.14).
For the lower lumbar spine (Table 3), only the male lifters decreased their lumbar lordosis during the start position compared to during standing habitual posture (group x position interaction in sagittal plane spinal alignment (F[1.9, 38.9] = 8.59, p = 0.001, η2p = 0.290). There were no differences between men and women in spinal alignment in the frontal (F[1.6, 34.3] = 1.16, p = 0.316) or horizontal planes (F[1.7, 34.7] = 0.45, p = 0.605) spinal alignment. In all participants their sagittal plane spinal alignment in standing habitual posture differed from the alignment at the start position and spinal adjustments were made in all three movement planes during the squat (significant main effect for position in the sagittal plane (F[1.9, 38.9] = 131.52, p < 0.001, η2p = 0.862), frontal plane (F[1.6, 34.3] = 19.15, p < 0.001, η2p = 0.477), and horizontal plane (F[1.7, 34.7] = 30.92, p < 0.001, η2p = 0.596). All three statistically significant comparisons for the lower lumbar spine had large effect sizes (η2p > 0.14).
The factorial repeated measures ANOVA simple effects for position in upper and lower lumbar sagittal plane spinal alignment are presented in Figures 1 and 2.
_and_lower_lumbar_spine_(lumbopelvic_region)_sagittal_plane_ha.jpg)
_and_lower_lumbar_spine_(lumbopelvic_region)_sagittal_plane_st.jpg)
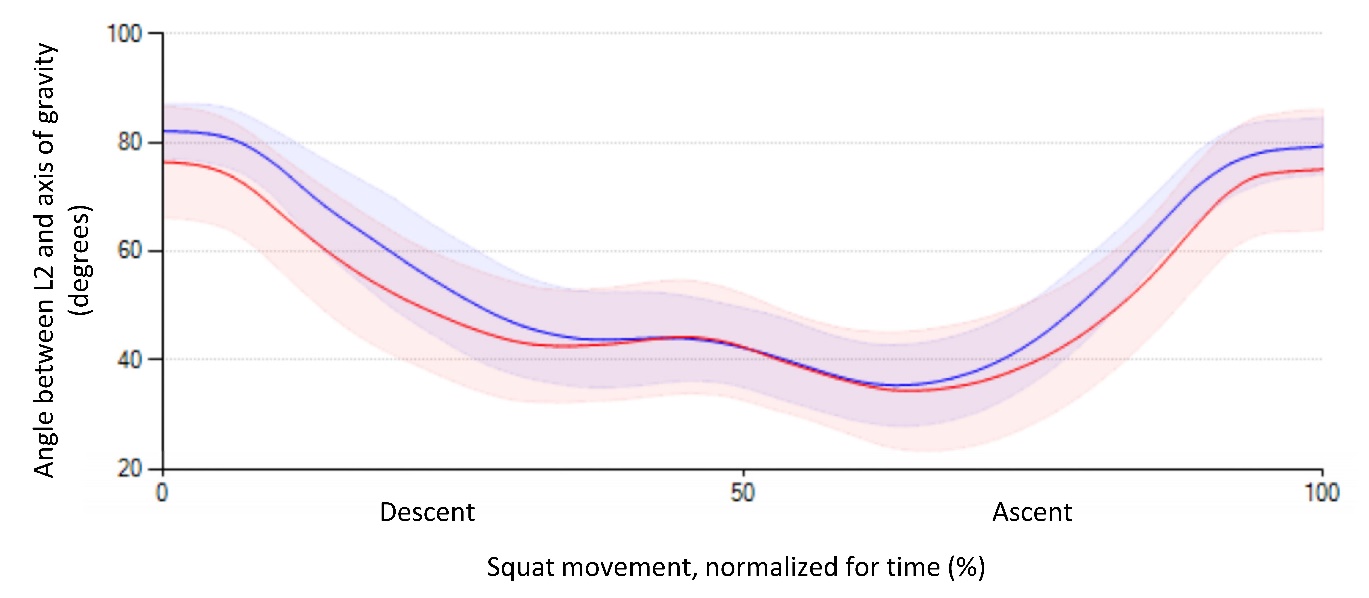
The full kinematic tracings of the angle between the IMU at L2 and axis of gravity, in the sagittal plane, for the full sample (n=23), during the squat is visualized in Figure 3.

DISCUSSION
This is the first study to investigate spinal alignment during the barbell back squat in experienced male and female power- and weightlifters. During the squat, spinal alignment was adjusted in all three planes of movement, especially in the sagittal plane. Lordosis in the upper lumbar spine (T11-L2) decreased among all participants from habitual posture to start position. In the lower lumbar spine (L2–S2) lordosis also decreased, but only among the male lifters. The difference in spinal alignment are consistent with the results of a study by McKean et al.,15 showing that with both a wide and narrow stance width the lumbar spine adjusts to a less lordotic alignment when a loaded barbell is placed on the shoulders.15 It is reasonable to hypothesize that the participants adjusted their spinal alignment in order to cope with the load and keep the combined body and barbell center of gravity within the base of support.15 However, the reason why male but not female lifters decreased their lordosis in the lower lumbar spine in their habitual posture compared to the start position is somewhat unclear. One possible explanation could be the female lifters, on average, used a load of 125% of their bodyweight and male lifters 192% of their bodyweight, and thereby not creating the same need to adjust their spinal alignment in order to keep their center of gravity within their base of support. Also, whether these differences between men and women in spinal kinematics could account for differences in injury localizations are unknown.
The results showing that lifters decrease their lumbar lordosis during the squat, is consistent with previous studies.13,15,16,29,30 Hebling Campos et al.29 found that the lumbar curvature is more flexed in the deepest position of a squat compared to the habitual standing. Further, the lumbar flexion is more evident when restricting the anterior translation of the knees.13,29 The less lordotic spinal alignment could, at least in part, be explained by the inherent hip flexion performed during the squat. Powerlifters in particular tend to perform a so called powerlifting style squat by “sitting back” into the squat. A greater forward lean during lifting tasks increases the likelihood of a less lordotic spinal alignment31 and it has further been argued that it is easier to maintain lumbar lordosis with an upright trunk when deadlifting.32 However, to the authors knowledge no studies have investigated underlying causes behind the different squat exercise movement patterns seen in male and females.
In contrast, Walsh et al.16 found that athletes extended their lumbar spines to a significant degree when squatting with heavier loads (60 and 80% of 1RM) but not with light loads (40% of 1RM). However, regardless of load, the athletes flexed their spines while descending to the bottom position. Walsh et al. noted that as a result, the athletes brought the weight in front of the spinal column and shifted their center of gravity anteriorly towards the forefoot. It was therefore speculated that lifters hyperextended their lumbar spine to shorten the moment arm length and to keep the center of gravity within the base of support. However, a shorter moment arm length could be achieved both by flexing and extending the spine and the reason for choosing one over the other direction is yet to be determined and may be dependent on the torso inclination. It should also be noted that in the study by Walsh et al.16 the subjects did not squat to IPF approved squat depth, but rather reversed the movement at apporixmately 90 degrees of hip flexion, which could explain the opposing results compared to the present study and the study by McKean et al.15
Minor adjustments of spinal alignment were made in the frontal and horizontal planes. This is in agreement with previous research showing less than 5° of lateral flexion and axial rotation when squatting with moderate to heavy loads.16 These minor adjustments in the frontal and horizontal planes are most likely not clinically relevant and implies that analyzing and correcting movements in these planes may be of less importance for the overall lifting performance.
Position statements and guidelines have proposed that neutral posture should be preserved during the squat, and that the trunk should be held stable without wavering or displacements throughout the movement.6–8 The observed adjustments of the lumbar spine alignment would imply that the lifters in the present study completed the squat with a technique proposed to increase risk of back injuries.6–8 However, the causative relationship between back injury and spinal alignment when squatting is yet to be confirmed.33 Further, the magnitude of the adjustments into flexion during the squat were 3.8 ± 4.3 and 16.7 ± 5.6 degrees in upper and lower lumbar spine, respectively, and should therefore be well within the lumbar spine range of motion in flexion/extension.
Some methodological considerations should be considered. Firstly, the lifters were asked to perform a squat with the only instruction being to, at their own pace, descend to a depth where the crease of the hip was lower than the top of the knee. Regarding depth, it was ascertained that they descended until the hip crease was lower than the top of the knee but some of them might have reached a greater depth. Therefore it is possible that these variations could, at least in part, explain the adjustments in spinal alignment.
Secondly, the lifters were instructed to perform three repetitions with a load equivalent to 70% of the lifters self-estimated 1RM. This repetition range and load are commonly used by both powerlifters and weightlifters and previous studies quantifying spinal alignment when squatting have used loads ranging from 40% to 80% of 1RM. It has to be noted though that load might influence on spinal alignment among recreational lifters.16 It is not yet known whether this also is true for competitive lifters, who are more used to lifting heavy loads.
Thirdly, when performing the ANOVA analysis the mean value of the three repetitions was used. This could have resulted in a regression to the mean. However, this was chosen over using a single repetition since using the mean values reduces the risk of random variations between repetitions.
Fourthly, angles measured using sensors on the skin might differ from the actual skeletal spinal alignment when musculature underneath is contracted. Skin tissue artefacts is a problem that cannot, however, be eliminated when using measurement systems that are based on mounting markers or sensors on the skin and must be considered when interpreting the results.
Lastly, a few lifters reported current injuries to the lumbopelvic, hip, knee and shoulder regions which impaired, but did not hinder, their ability to perform the squat and/or deadlift. It is also possible that some lifters had previously experienced pain and injury to the lumbopelvic region and lower extremities. Since it is well known that pain conditions can cause short term adaptations to lumbar spine kinematics and possibly also long term adaptations,34 the injury prevalence in the current sample could have affected the results. However, there were only two/three participants in total who reported a current lumboplevic or hip injury and therefore no statistical analysis of how pain could be associated with differences in lumbopelvic kinematics was included.
CONCLUSIONS
The results of the present study show that spinal adjustments are made by experienced male and female power- and weightlifters in all planes of movement during the barbell back squat. Most significantly, all lifters reduced their lordosis in the start position of the squat compared to their habitual posture, and all lifters reduced their lordosis even further during the squat. Male lifters also seem to reduce their lower lumbar spine lordosis significantly more than females in the start position compared to their habitual posture. The results can impact practice with relevance to how the barbell back squat is assessed, instructed, and executed in regard to the notion that the lumbar spine needs to maintain its neutral position during lifting. For example, the results imply that coaches and lifters might not need to be over vigilant in correction of spinal movements as long as the amplitude of movements do not place the individual in their outer ranges of motion. In all, spinal adjustments during heavy resistance training need further study to reveal their importance for performance and/or injury risk and possible explanations to why they occur.
Conflicts of interest
The authors report no conflicts of interest.
Acknowledgments
The authors wish to thank Jimmy Falk for his help with the data collection and to Boxen Umeå, Sweden, for allowing us to collect data in their facilities.
Funding
None declared.