
INTRODUCTION
Return to sport decisions can be challenging for clinicians and patients. While the phases of healing and clinical practice guidelines for specific injuries such as anterior cruciate ligament rupture1 or acute ankle sprains2 can be useful decision aids, return to sport decisions are often individualized and criteria are poorly defined for many patients. Ensuring clinicians have the knowledge and skills to make an informed return to sport decisions is vital for the health and safety of athletes.
The return to sport (RTS) continuum was developed to support the sports medicine team in return to sport decision making. The RTS continuum is comprised of three stages that are aligned with the rehabilitation process.3 However, numerous factors influence RTS besides physical and functional performance measures. Contextual factors such as psychological, environmental, social/contextual, personal, and cognitive factors may impact the injury, treatment, and outcomes.3–5 Disablement models, such as the International Classification of Functioning or Disability and Health, bring attention to these contextual factors and provide a patient-centered framework that accounts for the contextual factors. While disablement models highlight the importance of contextual factors, they may not offer sufficient guidance for transitioning patients back to participation. Combining the components of disablement models with the RTS continuum may help guide the individual and their sports medicine team in RTS decision making; however, it still lacks another critical construct, situational awareness (SA).
The chaotic nature of the sporting environment suggests that additional consideration should be given to an individual’s SA. SA encompasses the ability to perceive and comprehend information from the environment that predicts future status.6,7 SA is an ongoing process and must be sustained while rapidly making decisions in uncertain and time constrained environments. Furthermore, SA on a cognitive continuum describes three levels of control (strategic, tactical, and reactive) that increase uncertainty and decision making at each level.8,9 The necessity to achieve tactical and reactive control during athletic competition may be crucial for safely and successfully competing in athletics, however, SA is not currently a consideration in RTS. Research has shown that when adding cognitive challenge to physical tasks there is a decline in performance10–12; therefore, neglecting to address circumstantial factors and SA may put individuals in a situation where they are ill-equipped for RTS. Developing theoretical perspectives that integrate SA with contemporary models for formulating return to sport decision making is an important step for further research and clinical investigation. Therefore, the purpose of this clinical commentary is to describe a return to sport model that integrates SA theory on the cognitive continuum with additional consideration for surrounding contextual factors.
THE RETURN TO SPORT CONTINUUM
The return to sport continuum is beneficial in guiding an inclusive sports medicine team in RTS decision making. Traditionally, RTS is viewed as an isolated decision at the end of rehabilitation rather than an involved process spanning from the moment an injury is sustained until after the individual has returned to full participation.3 Though not included in the original return to sport continuum by Ardern et al.,3 for the purposes of this paper the authors have added a stage prior to the beginning of the return to sport continuum, called pre-participation. Pre-participation may be considered when rehabilitation is being performed primarily in the clinic and the athlete is not participating in any training. Following pre-participation they may begin the return to sport continuum, which is comprised of three phases: return to participation, return to sport, and return to performance.3 During return to participation the athlete may participate in some training (generally non-contact or modified, early on in this phase), but they are not ready to RTS.3 Return to sport is when the athlete has returned to competition, though they have not reached their desired level of performance.3 In the last phase, return to performance, the athletes’ performance capabilities have returned to or exceeded the pre-injury level.3 It is important to note that these phases only describe a level of status and do not entirely define how that status is obtained.
SITUATIONAL AWARENESS (SA) THEORY
SA is an abstract concept that has been adapted and reconstructed over many years. There are many definitions of SA, though a commonly accepted definition is by Endsley in 1988 stating “situational awareness is the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future.”6 Endsley describes the three components of SA (perception, comprehension, and projection) as a state of knowledge pertaining to the dynamic environment.7 Further, SA, decision making, and action are depicted as distinct components of a linear process where SA dictates decision making and impacts how the individual responds.7 For example, a basketball athlete perceives where the ball, teammates, and opponents are in relation to a specific location on the court with attention to the game clock. Based on the disjointed knowledge they perceive from the environment; they piece together the information to paint a complete picture. The understanding developed from the position of the ball and other players allows them to predict the future movement of their opponent, decide how they want to respond, and act accordingly. Some argue against the linearity of this process, stating that perceiving an object or situation is both a decision made by the individual and an action; therefore, action both precedes SA and is a result of it.13,14 While SA, action, and decision making are linked, the view of the interaction between these three components has evolved.
Cognitive function influences the ability to achieve SA, though it is also an independent process.7 Cognitive constructs such as attention, perception, and memory should be considered when understanding SA.7 Attention allows individuals to direct their focus and dictate what aspects of the environment are vital and relevant. Attention has a limited capacity, so in complex environments where many events are happening simultaneously, such as the sporting environment, the increased attentional demand takes away from SA.7 Additionally, each individual’s perception of the environment, whether accurate or not, will influence expectations and the projection of the future (direct components of SA).7 Furthermore, manipulating short-term memory stores in conjunction with existing knowledge is used to adapt to the current situation, a process of working memory.7 Beyond working memory, long-term memory categorically stores information linked to relevant goals and scripts.7 It has been shown that long-term memory, rather than working memory, distinguishes between an expert and a novice.15 When an individual identifies specific cues in the environment, long-term memory allows them to draw on those scripts and make rapid decisions.7 Along with long-term memory stores, individuals may achieve automaticity. Automaticity is quick and effortless cognitive processing that requires little attentional demand.7 The individual is aware of their surroundings and the context of the situation; however, they can automatically retrieve the information from memory stores necessary to respond according to the circumstances.7 For example, in a basketball game numerous events are taking place at the same time. Suppose the athlete’s attention is on the opposing player directly in front of them. In that case, there is less attention on the surrounding environment, so they may miss what is happening on the other side of the court (i.e., there is increased SA regarding the player in front of them and decreased SA of the surrounding environment). If the coach devises a new play and a teammate gesture to signal the play (perception), there are certain expectations on what that means and the immediate actions that will follow. The ability to remember and adapt the play to the present circumstances (working memory) is crucial for successful execution. Naturally, plans don’t always work out perfectly. When plans go awry, individuals may revert to what they have practiced numerous times with little thought or planning (long-term memory and automaticity), such as going for the layup when there is an opening. Becoming more effective in these cognitive processes may aid in an individual’s ability to achieve SA.
SITUATIONAL AWARENESS ON A COGNITIVE CONTINUUM
Varying degrees of SA and consequently, decision making, may differ based on the uncertainty of the situation and the time contraint.8 SA on a cognitive continuum describes three levels of decision making and control in response to complex situations: strategic, tactical, and reactive.8,9
Strategic control is when there is little to no uncertainty with no time constraints.7 Strategic control is primarily employed in controlled environments during rehabilitation where the athlete can coordinate movements at a self-designated pace.9 During the early rehabilitation phase, the athlete can form high-quality movements and establish a solid foundation upon which they can build.9
Tactical control transitions the individual from the controlled clinic settings to sport-specific drills in relatively controlled environments.9 Tactical control grows in complexity as uncertainty increases and/or the time allotted to complete the task decreases.7 The increased time constraint and uncertainty during the tactical level forces the athlete to rely on working memory and challenges the athlete’s attention and perception; these cognitive processes aim to help facilitate SA. They begin to increase reliance on previous knowledge and experience to counteract the increased demand.9 During tactical control, the individual applies what was previously established during strategic control but in time-dependent and ambiguous situations.9
As uncertainty and time constraints increase, tactical control progresses to reactive control. The environmental complexity in this phase is reflective of live gameplay. Due to the intricacy of a situation, athletes may exhibit a “panic” style of coordination instead of reactive control in which they are unable to achieve SA while simultaneously carrying out coordinated physical movements.8,9 During the reactive “panic” style of coordination, athletes may exhibit impulsive and high injury risk behaviors.9,16 As task complexity, cognitive load, and attention demand increase, the likelihood of attaining SA decreases.7 Due to limited attention capacity, some components of the environment will demand increased attention, taking attention away from other aspects of the environment. In areas of compromised attention there may be altered perceptions and expectations resulting in diminished SA.7 The culmination of altered cognitive processes that result in diminished SA may result in increased cognitive or movement errors, placing individuals at an increased risk of injury.16 Furthermore, where working memory falls short, there may be an increased reliance on long-term memory stores and automaticity during reactive control.7 Automaticity may combat the negative effects of increased uncertainty and time constraints by bypassing the cognitive processes. Automaticity may aid in the transition from exhibiting a panic style of coordination to reactive control.
A MODEL FOR APPLYING SITUATIONAL AWARENESS THEORY TO THE RETURN TO SPORT CONTINUUM
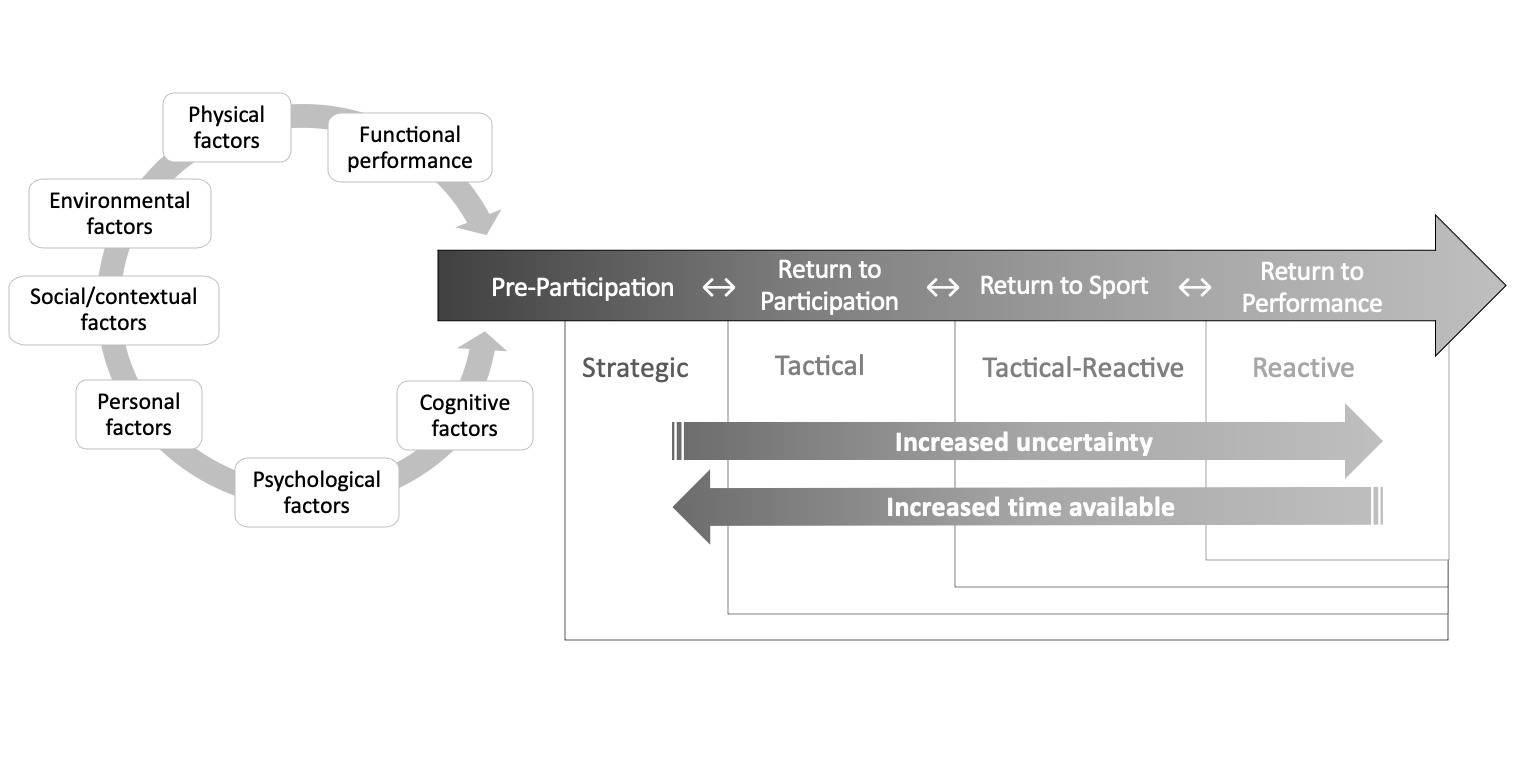
Applying SA theory to the return to sport continuum may provide additional considerations regarding an individual’s ability to display control and make rapid decisions during the RTS process. In addition to functional performance, cognitive, psychological, personal, social/contextual, environmental, and physical factors should be considered before a patient initiates the return to sport phase. To promote the health and safety of the athlete, most individuals enter the model at pre-participation or return to participation, regardless of injury type or severity. This ensures that they meet the necessary criteria and contextual factors are considered before progressing through the RTS continuum (Figure 1). Strategic control should be established during pre-participation, tactical control should be established during return to participation, tactical-reactive (the transition from tactical to reactive) control should be established during the return to sport, and reactive control should be established during return to performance (Figure 1). While this model provides general guidelines, it is a fluid process where individuals may shift forward or backward between different levels of SA depending not only on the phase of RTS, but the specific task and environment as well. For example, an individual may exhibit proficiency at a reactive level of control during one task and a tactical level of control during another. Progressing through the phases of SA on the cognitive continuum should be a gradual process where there is successful task completion with minimal errors before adding additional challenges, constraints, or environmental complexity.
Furthermore, the RTS process should be individualized. Two individuals with the same injury and comparable physical function may exhibit different levels of control during the same task; one maintains reactive control while the other reaches failure and experiences a panic style of coordination under similar levels of constraint. The RTS process should hinge on an individual’s ability to display movement control safely and successfully in uncertain and complex situations. For continuity, the authors maintain one example throughout the application of SA theory being applied to the RTS continuum. There are three example scenarios presented in Appendix 1 for application of the model; however, the purpose of this commentary is not to provide specific clinical guidelines.
Depending on the severity of the injury, athletes may be initially removed from sports participation prior to entering the RTS continuum to protect the health and safety of the athlete. During this time, the pre-participation phase, athletes typically undergo rehabilitation in a controlled clinic setting. Strategic control should be the primary focus during this phase. Regaining range of motion, building strength, and focusing on proper biomechanics are some appropriate tactics to improve strategic control. For example, following an acute lateral ankle sprain in a basketball player, the individual may be completing alphabet drills for range of motion, 4-way ankle exercises for strength, and working on returning to a normal gait pattern. When the player is ready to start dynamic load bearing exercises, they may complete plyometric tasks, working on proper jumping and landing mechanics. With no time constraints, the individual can become comfortable with the task at their own pace and form appropriate techniques in a safe environment.9
As an athlete integrates rehabilitation in a clinical setting with sports-specific drills on the sideline, they enter the return to participation phase of the RTS continuum. During this phase, individuals should work toward gaining tactical control by adding decision making to movement competence. Cognitive challenges (i.e., choice-reaction time and working memory) can be added to jumping, landing, and linear movements to gain tactical control. To progress within this phase, increasing the complexity of activities to multidirectional cutting and agility tasks with cognitive challenges may be appropriate. For the lateral ankle sprain patient, it may start with a choice-reaction hopping task where the individual jumps and lands on a specific limb in rapid response to different visual or auditory cues. They should aim to maintain the proper landing mechanics they previously learned. When control during foundational tasks is established, they may progress to non-linear patterns of unanticipated cutting tasks requiring multidirectional movements that are unanticipated and in response to an external cue (i.e., a verbal command or visual cue).
When tactical control has been achieved and the athlete has met all other criteria (i.e., functional performance, cognitive control, and psychological readiness) they may transition to return to sport. While they may be ready to return to sport, it does not mean they have returned to their previous level of performance. Depending on the demands of their sport they may need to improve in aspects of speed, agility, accuracy, reaction time or decision making. During this phase, the increased uncertainty and time constraints shift from tactical control to tactical-reactive control. To achieve tactical-reactive control the athlete should be introduced to sports-specific reactive drills in which they are making rapid decisions in response to their environment (i.e., other players and obstacles). These tasks can be completed individually or integrated into practice, beginning with team drills and transitioning to live gameplay as they achieve greater tactical-reactive control. The lateral ankle sprain patient may increase the number of cues they have to remember and react to during the unanticipated cutting drills. Where previously only two scenarios could happen (cut right or cut left), now with increased cues (cut right, cut left, backpedal, forward sprint), it increases the amount of uncertainty within the task. With the team, they may complete exercises where they dribble through obstacles and are required to act in response to an environmental stimulus (i.e., shooting if an opponent comes from the left versus passing if an opponent comes from the right).
Traditionally, when an individual returns to competition that often signifies the end of formal rehabilitative care. However, additional intervention may be necessary to return to previous levels of performance. During return to performance, the athlete is working to transition from a “panic” style of coordination where there is increased susceptibility of sustaining injury to achieving reactive control.9 As the lateral ankle sprain patient continues to work on unanticipated cutting, they may now have to increase the speed at which they are required to complete the task, giving them little time to process the external situation, predict future actions, and make decisions. Increased exposure to chaotic situations and training to gain reactive control will develop mental models in long-term memory that the individual can draw on, as well as form efficient automaticity where less attention is required and quicker processing occurs.7
Return to sport is a complex and fluid process, therefore athletes may have setbacks and not progress through the continuum as expected. This may be due to numerous factors such as reaggravation of the injury, poor responses to loading, or psychological challenges. If an individual experiences a setback, they may return to the previous level in the continuum, return to the beginning of the model, or be removed from sport. They may return to a previous level due to one or more factors: failure to achieve or maintain the appropriate level of SA, inability to adapt to increased load, or surrounding contextual factors. This is highlighted in the figure with the use of bidirectional arrows between the stages (Figure 1). Following any obstacles, wherever the individual re-enters the RTS model they will continue to work on identified goals and progress through the model until they have achieved the desired level of performance.
There are innumerable factors that may hinder or facilitate in return to play decision making. Contextual factors include cognitive function, psychological factors, personal factors, social or contextual factors, environmental factors, physical factors, and functional performance. Cognitive performance may influence how quickly an individual is able to achieve SA and progresses through the phases of RTS. Psychological factors such as readiness or fear of reinjury may impact how effective an athlete is on the field.4 If the athlete is not ready psychologically they may more rapidly display a panic style of coordination or freeze in complex situations, predisposing them to reinjury. Personal factors such as sociodemographic factors, health behavior, or socioeconomic status may not all be modifiable, but are still important considerations in healing and RTS.4,5 There can be a wide range of social and contextual factors such as expectations of recovery, quality of life, level of competition, time of the season, and type of sport that may influence stakeholders’ decision to return to play.3,4 This includes, but is not limited to, whether they have realistic expectations of recovery versus impractical expectations, if it is preseason versus the conference championships, or if the athlete is a redshirt freshman versus a senior. Environmental factors such as living conditions, transportation, and support from community, family, and friends may create barriers to access and impact efficient RTS. Physical factors (e.g., muscle strength, swelling, and range of motion) and performance on functional tests (e.g., crossover hop, Y-Balance test, Agility t-test) should be within acceptable limits of the contralateral limb or pre-injury levels before attempting to return an athlete to sport.3,17 While physical and functional performance may not be direct indicators for RTS readiness, they are vital for the athlete’s safety. Contextual factors surrounding the individual interact with one another and, therefore, must be considered in conjunction rather than in isolation.
Research has explored the development of integrated neuromuscular-cognitive assessments. These assessments may be used to evaluate situation awareness in the RTS context. Some assessments have added cognitive challenges (reaction time, working memory, and inhibitory control) to traditional hop tests (single leg hop, single leg triple hop, single leg crossover hop, and single leg six-meter hop).11 Additionally, other assessments evaluating upper and lower extremity reaction time and inhibitory control, reactive agility, and unanticipated cutting have been developed.18 Further, Walker et al.19 proposed a criterion-based progression in which tasks may increase in physical or cognitive difficulty when there is a low (0-1 errors) neuromuscular and cognitive error rate. If there is a high error rate (≥3 errors) or significant errors the task may be too challenging.19 Guidelines from Walker et al.19 were utilized for exercise progression in the provided scenarios (Appendix 1). Further research is needed to determine the best approach for assessing SA during the return to sport process.
CONCLUSION
The proposed model for applying SA theory on the cognitive continuum to the return to sport continuum was developed to aid return to play decision making. This model identifies levels of SA that should be targeted during the varying stages of return to play. Additionally, the model considers the numerous contextual factors that influence RTS decisions. Applying this new model may further optimize disablement models by providing guidance on transitioning individuals back to participation. Conversely, neglecting to consider contextual factors and SA in RTS decisions could contribute to an increased risk of re-injury.
Conflicts of Interest
The authors have no conflicts of interest.