


Introduction
The core plays a vital role in providing stability, force transmission, and injury prevention in athletes. While we know training the core is essential to optimize its function and minimize the risk of injuries the literature is lacking a systematic and evidence-based approach to doing so. This clinical commentary aims to provide an overview of the anatomy, function, common injuries, and clinical evaluation of the core. Furthermore, it introduces a four-phase intervention program, the “Core Four Pyramid Principles,” which serves as a guideline for designing effective core training programs in sports physical therapy.
Anatomy
The core anatomy refers to all structures situated between the scapula and glutes.1 This encompasses the lumbo-pelvic hip complex, which spans from the diaphragm to the pelvic floor, and extends from the multifidus to the recuts abdomen. The core structures can be characterized into stabilizers, such as the internal and external obliques, which eccentrically control range of motion and mobilizers like the rectus abdomen and iliocostalis, which concentrically accelerate individuals through their ROM. While it’s important to train the core muscles independently, these muscles work interdependently through fascial slings, composed of dense connective tissue, which form a dynamic system that connects these muscle groups to allow for efficient movement, and force transmission throughout the body in a chain-like effect.
Core Functions
The core serves four primary functions that are crucial for athletic performance. Firstly, it anticipates movement, enabling the body to prepare for dynamic actions effectively.2 Secondly, it stabilizes the spine, providing a solid foundation for force transmission.3 Thirdly, it prepares the body for load-bearing activities, ensuring adequate support during weight-bearing exercises.4 Lastly, the core acts as a link between the upper and lower extremities, facilitating coordinated movements during activities such as walking, running, throwing.5,6
Core Stability
Core stability plays a vital role in athletic function and performance. It involves the detection of central nervous system changes for anticipatory muscle recruitment to maintain trunk position over a stable pelvic base and prevent buckling or promote return to equilibrium following perturbations.7,8 This contributes to overall movement efficiency, dynamic control, and injury prevention during sporting events.
Common Injuries in Sport
In various sports, core injuries are a common occurrence and can have significant clinical relevance in terms of training and injury prevention. Research studies have shed light on the prevalence and characteristics of core injuries in different sports.
Baseball: In professional baseball, abdominal strains have been identified as a frequent core injury. Conte et al 2012 reported that abdominal strains accounted for 5% of all injuries among players on the disabled list, with a notable upward trend in the 2000’s.9 These strains primarily involved the internal/external obliques with a higher occurrence in hitters and a contralateral (lead side) bias. Camp, Conte et al 2017 further emphasized the impact of oblique injuries in baseball, reporting 996 oblique injuries per year, leading to a substantial number of missed days (22,064 days in total).10 These injuries were more prevalent in the minor leagues, with hitting being the most affected aspect. The reinjury rate was significant, reaching 8.15%, and early season occurrences were more common. Injections for treatment led to longer return to play prognoses.
Basketball: Core training holds significant clinical relevance based on the injury data presented in the studies focusing on basketball players. Jackson et al conducted a 24-year overview of hip injuries in the NBA between the 1988 through 2012 season.11 This group revealed that hip injuries, including hamstring and adductor strains frequently occurred in the first month of the season. Patel et al analyzed return to play and player performance with regards to adductor injuries from 2010 to 2019. This group reported that groin injuries affected 72 players, with 6 cases requiring surgical intervention. The average return to play was approximately 7-10 games or 17-20 days, and there was an 18% reinjury rate observed, even up to 1.5 years later.12 Despite the risk of reinjury, the study found no change in return to performance, indicating effective rehabilitation strategies.
Football: In football, both hip and core injuries have been investigated. Tramer et al studied nonoperatively treated hip and core injuries in National Football League (NFL) athletes between 2010 and 2016, identifying a total of 112 players affected. This study indicates that offensive and defensive players missed 4.0 ± 5.2 and 3.1 ± 2.6 games after injury, respectively. Furthermore, a study by Jack et al analyzed performance and return to sport rates amongst NFL players who underwent sports hernia surgery between 1996 and 2015. They conclude that 94.7% of players were able to return to sports and defensive backs and wide receivers were amongst the most common positions affected.13
Hockey: Hockey players are also prone to core injuries, specifically groin and abdominal strains. Tyler et al. reported a rate of 3.2 groin strains per 1000 player-game exposures.14 Emery C A et al. previously highlighted the prevalence of groin strains in the National Hockey League (NHL) and revealed that these injuries were more 5x and 20x more likely to occur during training camp compared to the regular season and post season, respectively. They further found that the most common mechanism was non-contact (90%) with a mean time loss of 10.59 sessions for abdominal injuries and 6.59 sessions for groin injuries.15
Soccer: Core injuries in professional soccer have been a prevalent concern, impacting the performance and availability of players. According to Giza et al (BJSM, 2005), groin strains affected 9.5% of all professional male soccer players in the United States during the 2002 season.16 A more recent review by Sherman et al. revealed that hip and groin injuries accounted for 14% of all soccer injuries.17 Ekstrand et al. she light on the epidemiology of muscle injuries in professional soccer, stating that most injuries occur later in the game and are more common to occur among older players. Of the muscle strains reported, 23% were adductor-related, resulting in an average of 14.0 ± 6.2 days, while abdominal strains accounted for less than 1% but caused an average absence of 12.6 ± 9.2 days.18 These findings highlight the significance of core injuries in professional soccer and emphasize the need for effective preventive measures and targeted rehabilitation protocols to mitigate their impact on players.
Clinical Evaluation
Clinical evaluation of core injuries involves understanding the mechanism of injury, demands of sport followed by subjective and objective assessments, functional testing, and specific special tests to identify root cause of injury.
The rectus abdominis and adductor longus are commonly injured as they have opposing force vectors and act as antagonists during hip extension and core rotation. These fibers join on the pelvis along the pubic symphysis forming the pubic aponeurosis or “plate”, which serves as a fulcrum for these structures. It is hypothesized that injury to either tendon alters the biomechanics and thus the stability of the pelvis leaving the symphysis susceptible to further injury.19
Subjectively, patients most commonly report deep, chronic groin or lower abdominal pain with exercise that resolves at rest and is exacerbated with change of direction.20 They may report experiencing a “catch” or a “bite” in the affected region and may exhibit pain-related behaviors such as grabbing the area or grimacing when provoked. Common mechanisms of injury, as identified by Anderson et al. in Sports Health 2013, include excessive forceful rotation, hyperextension with rotation, excessive spinal load, and poor trunk-pelvic dissociation.21
In the objective component of the evaluation, palpation is used to assess tenderness in the core region.22 Range of motion in the thoracic spine and pelvis is measured in various positions and the position of the ribs is to be examined. The control of the diaphragm and pelvic floor is also assessed. An ideal state is characterized by a 360° pressure chamber, where the diaphragm domes through rib internal rotation during exhalation with posterior pelvic tilt. However, many individuals exhibit rib external rotation with a flat diaphragm which can be seen by a flared position in resting state which may lead to longer lasting pain.23,24 It is important to note that the left diaphragm is lower with a smaller central tendon, which may contribute to natural asymmetries and potential injuries, especially in rotational athletes. Lastly, it is essential to measure strength, specifically the adductor-to-abductor ratio, as Tyler et al. (AJSM 2001) report a 17-fold higher risk of injury in individuals with a ratio below 80%.14
Functional testing involves specific exercises to assess core function. These include the single-leg squat/step-up, single-leg hip bridge, and trunk endurance test. Chaudhair et al. (AJSM 2014) found that increased peak anterior-posterior pelvic deviation during a 3" step-up was associated with a higher risk of shoulder injuries, UCL tears, and other elbow strains amongst major league pitchers during a competitive season.25 Meister et al (AJSM 2021) also found a link between decreased core stability, as determined by pelvic deviation during single-leg balance, and upper extremity injury among a group of professional pitches during a competitive season.26
Trunk endurance testing plays a crucial role in understanding the relationship between core stability and lower extremity injuries. Research conducted by McGill et al. provides valuable insights into the average endurance times for various trunk exercises. The study revealed that females generally exhibited greater endurance in flexion and extension exercises, while males demonstrated better endurance in side-bridge exercises. Additionally, the ratio of endurance between flexion and extension exercises was found to be slightly higher in males than in females. These findings highlight the significance of gender-specific differences in trunk endurance.27 Moreover, Leetun et al. demonstrated that athletes with lower core stability measures were more prone to lower extremity injuries compared to those with higher stability measures. Injured athletes exhibited less hip abduction and external rotation percentage of strength compared to body weight, and reduced side-bridge and back extension endurance.28 This underscores the importance of maintaining proximal stability to prevent distal injuries. Overall, trunk endurance testing serves as an essential tool in assessing core stability and its impact on the risk of injuries.
Special tests are performed to further evaluate core injuries and confirm clinical diagnoses. The “cough test” involves having the individual cough, which may reproduce pain in the affected area.29 The resisted adduction sit up test (RASUT) is used to differentiate pelvic from hip pathology and identify patients without athletic pubalgia as it has a diagnostic odds ratio of 6.08, a sensitivity of 78% and 88% negative predictive accuracy. (figure 1)30

Kurowicki et al. found 100% sensitivity identifying core muscle injury utilizing four criteria. The following tests will elicit pain or reproduce the patients’ symptoms. The first; resisted cross-body sit-up in a figure of four position. The patient lies supine and places the symptomatic side limb into a figure of four position and brings the contralateral shoulder towards the symptomatic side against resistance. The second is a straight leg sit-up where the patient lies supine and raises both shoulders and the symptomatic leg approximately 10 inches off the table and attempts to maintain this position against resistance. The third is resisted hip flexion in an externally rotated position. The final is the presence of an adductor contracture while in a figure of four position.31 (Figure 2)

Lastly, the author utilizes a personalized dynamic core assessment to assess multiplanar stabilization. The therapist has the patient lie in a dead bug starting position (Figure 3) and applies resistance in multiple directions challenging the stability of each fascial line. The therapist communicates with the patient to determine the most challenging stabilization direction. This assessment helps identify deficits and develop a personalized program.

Core Four Pyramid Principle
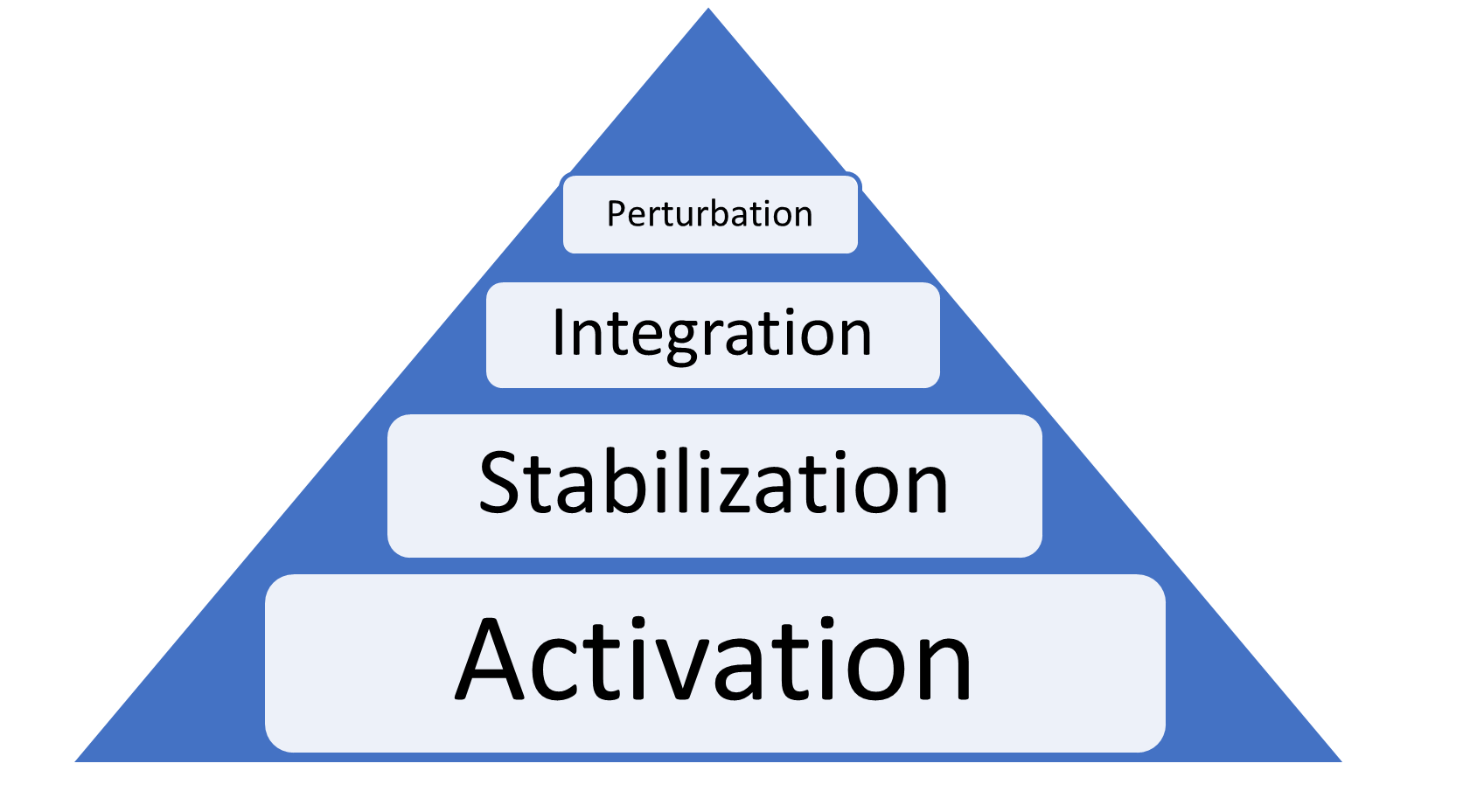
Core training plays a crucial role in optimizing athletic performance and preventing injuries. In our programming and intervention approach, we implement the “Core Four Pyramid Principles,” which encompasses four distinct phases: activation, stabilization, integration, and perturbation. Each phase has specific criteria for entry, goals to achieve, and targeted exercises to support those goals.
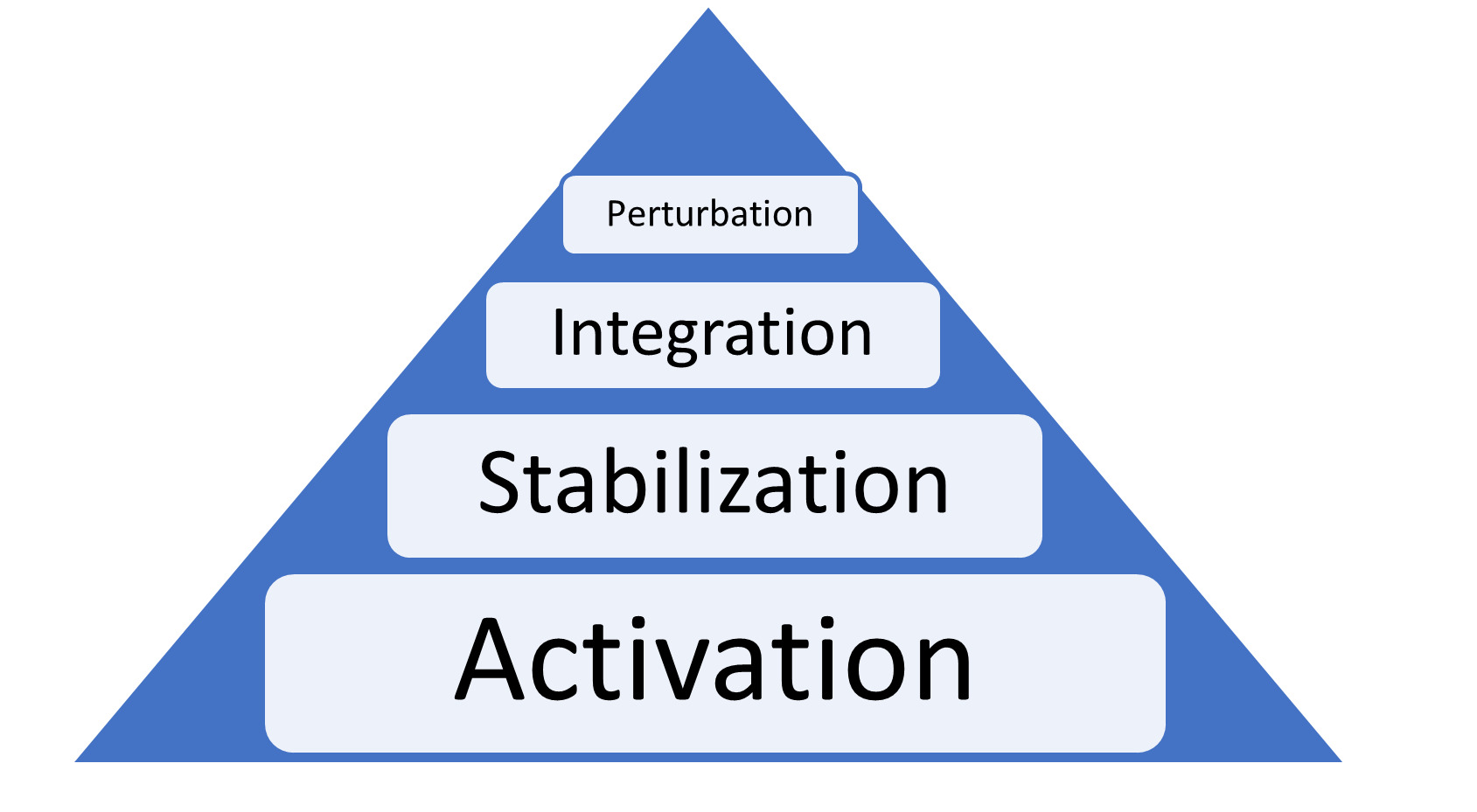
During the activation phase, our objectives are to reduce pain, restore proper breathing patterns, improve posture and range of motion, teach core bracing, increase hip strength and provide education to the patient. Therapeutic interventions such as modalities, biofeedback, diaphragmatic breathing, core isometrics, hip exercises, pelvic positioning and trunk-hip dissociation mobility drills are employed to facilitate these goals.
As athletes progress to the stabilization phase, criteria for entry include coordinated breath, adequate postural alignment, the ability to voluntarily brace the core without cueing, improved hip strength rations (ABD:ADD ratio), and enhanced trunk endurance ratios. The goals of this phase are to maintain proximal stability with distal mobility, generate torque and force, introduce rhythmic stability, and restore trunk endurance and hip strength ratios. Therapeutic interventions include anti-movement exercises like dead-bugs, bird-dogs, pallof press, chops, lifts and endurance-based core exercises such as plank variations (side, Copenhagen), revers and regular hyperextensions, bridging, and balance/proprioception exercises. Haroy et al. investigated the efficacy of Copenhagen exercises in core training amongst a group of 35 semi-professional soccer teams. The randomized controlled trial design had one half of the teams perform three levels of Copenhagen planks three times per week during the preseason (6-8 weeks) and once per week during the competitive season (28 weeks). The results indicated a remarkable 41% decrease in groin-related injury rate in the intervention group, emphasizing the importance of this specific exercise.32
Moving into the integration phase, athletes must demonstrate restored ratios and exhibit no postural breakdown during multi-joint exercises. The goal in this phase is to load functional patterns, and interventions involve movements like squatting, hinging, lunging, carrying, vertical/horizontal pressing and rowing, lateral sliding and crawling.
Finally, in the perturbation phase, athletes need to meet the criteria such as maintaining good alignment under loaded conditions and exhibit adequate neuromuscular control on unstable surfaces or on firm surfaces with eyes closed. The main goal here is to enhance the central nervous system’s ability to detect changes, adapt to external forces for improved stability and force transmission and enhance reaction time. Interventions include dual tasks, manual resistance/perturbations, visual-based reaction tasks and verbal command activities.
By following this systematic and criterion-based approach to core training, athletes can optimize their core function, stability and overall athletic performance while reducing the risk of injuries.
Conclusion
In conclusion, this clinical commentary emphasizes the importance of a comprehensive approach to core training in sports physical therapy for optimizing athletic performance and minimizing injuries. The core plays a vital role in providing stability, force transmission, and injury prevention in athletes. Through an in-depth exploration of core anatomy, functions, common injuries in various sports, and clinical evaluation techniques, this commentary provides valuable insights for sports physical therapists. The implementation of the “Core Four Pyramid Principles,” consisting of activation, stabilization, integration, and perturbation phases, offers a systematic and evidence-based framework for designing effective core training programs. By following this approach athletes can enhance their core function, stability, and overall performance while reducing the risk of injuries. The findings and recommendations presented in this paper contribute to the growing body of knowledge in the field of sports physical therapy and serve as a valuable resource for practitioners working with athletes at all levels.