INTRODUCTION
Recently, it has been suggested that lower neurocognitive function is a risk factor for anterior cruciate ligament (ACL) injury.1 Swanik et al.1 utilized the “ImPACT” neurocognitive assessment test, primarily used to evaluate function after a concussion, to measure neurocognitive function. This computer-based test can be used to establish a pre-season baseline score. They conducted a retrospective comparison of mean scores between the non-contact ACL-injured group and the healthy control group. Lower scores were present in the non-contact ACL-injured group for reaction time, processing speed, and visual/verbal memory.1 Consequently, it was proposed that diminished neurocognitive function may contribute to the risk of non-contact ACL injuries. However, the precise mechanism by which lower neurocognitive function increases this risk remains incompletely understood.
The hypothesis that reduced neurocognitive function serves as a risk factor for non-contact ACL injuries suggests a need for assessment of alterations in neuromuscular control within the trunk, pelvis, and lower limbs.2,3 Sporting activities entail complex athletic tasks that do not afford athletes the luxury of pre-planning their movements. Moreover, athletes have limited time for cognitive processing during motion selection. Therefore, athletes experience a high cognitive load during sports activities.4 In other words, athletes with poor neurocognitive function may struggle to address postural control during landing motion due to the dual-task demands of situational judgment and movement selection. Specifically, deficiencies in visual attention, self-monitoring, agility/fine motor performance, processing speed/reaction time, and dual-tasking are believed to predispose individuals to landing mechanics that afford a heightened risk of ACL injury within complex sporting environments.5
The effects of difference neurocognitive function on lower limb kinematics and kinetics during unanticipated jump-landing task have been studied in male and female recreational athletes using the Concussion Resolution Index (CRI).2 From the six subtests of the CRI, three indices of Simple Reaction Time, Complex Reaction Time, and Processing Speed have been created and divided into a two groups based on the following criteria: the higher performers group was defined as participants scoring above the 80th percentile in one score and with two scores no lower than 60th percentile, and the low performers group were defined as participants with one subtest score below the 40th percentile and with two scores no higher than the 70th percentile, or with at least two scores below the 30th percentile.2 The low performers group exhibited significantly increased peak vertical ground reaction force (GRF), peak anterior tibial shear force, knee abduction moment, knee valgus angle, and decreased trunk flexion angle.2 Additionally, the landing biomechanics of the low performers group were more consistent with landing biomechanics which have been identified as a risk factor for non-contact ACL injury.6,7 It is important to note that the prior study participants consisted of mixed male and female recreational athletes. Although ACL injuries are more prevalent in males, the incidence is higher in females.8 Analysis of unanticipated single-leg drop-jump landing and cutting motion shows that female athletes have a higher incidence of ACL injury than male athletes due to an increased tendency to demonstrate increased knee valgus angle moment.3,9 In a previous study, only female athletes were included to examine the effects of neurocognitive function on landing mechanics. Moreover, the authors have previously examined the effects of differences in neurocognitive function on an unanticipated cutting motion.10 Female athletes with lower neurocognitive function were found more likely to produce significant greater quadriceps muscle activity patterns, thereby increasing their susceptibility to ACL injuries.10 The present study is an addition to prior projects and focuses on the single-leg drop-jump landing motion from a 30-cm high box.
The purpose of this study was clarify the effect of differences in neurocognitive function on landing mechanics during single-leg drop-jump landing motion followed by an unanticipated task. The authors hypothesized that female athletes with lower neurocognitive function would demonstrate higher knee joint valgus angle and moments, lower trunk forward flexion angle, and show quadriceps dominant muscle activities, all of which are associated with elevated ACL injury risk.
METHODS
Participants
Fifteen female athletes who played basketball or soccer in university athletic clubs were recruited. They belonged to the highest national competition level, and they practiced two to three hours a day, five to six days a week. Exclusion criteria included a history of lower limb injury and concussion within the prior six months, any disorder of the peripheral sensory system, a history of surgery on the lumbar spine or lower limbs, and ADHD or anxiety, which may influence psychomotor speed. Furthermore, alcohol and caffeine intake were restricted on the night before the experiment. All participants provided written informed consent prior to their participation. This study was approved by the Ethical Committee of the Faculty of Health and Sports Sciences at the University of Tsukuba (approval number. 28-37).
Neurocognitive Test
Neurocognitive testing was performed using the Symbol Digit Modalities Test (SDMT). SDMT was performed on the same day as the motion analysis and before the landing task operation. Participants were asked to fill out 110 boxes under symbols with a corresponding number within 90 seconds while referring to a key on top of the test form to identify which number goes with each symbol.11 The number of correct answers was counted.
The SDMT has been widely used to evaluate information processing speed (IPS) and selective attention.12 It has been utilized for neurocognitive assessment of patients with impaired IPS,13,14 as well as for functional evaluation before and after a concussion and for evaluation of neurocognitive function in patients with Multiple Sclerosis.15–17 The SDMT is suitable for serial neurocognitive function testing because it is easy to administer, inexpensive, and requires a short assessment time.17,18 Inter-rater reliability (ICC 2,1) of the SDMT was reported to be 0.72,17 and test-retest reliability was reported to be acceptable with r = 0.70-0.80 for healthy adults measured at 1-month or 2-week intervals.19,20 This assessment was adopted in this study as a neurocognitive function assessment test because it can be easily measured in sports situations. Furthermore, the SDMT has been reported to have a learning effect,17,21 albeit less pronounced compared to the Trail Making Test-B or the Stroop Interference Test.17 The mean SDMT score has been reported to be 58.2 ± 9.1 (range = 51.87-63.93) for young adults (< 30 years), and 53.2 ± 8.9 (range = 44.4-58.7) for middle adulthoods (30-55 years).22 Another study reported a mean score of 53.06 ± 11.50 for male college athletes.23
Participants were grouped according to SDMT score. The median SDMT score was used as a cut-off value to group the participants, since the mean of the participants in this study was higher than the reference value (the mean SDMT score: 71.5 ± 7.5).22,23 The upper group was the high-performance group (HP group), and the lower group was the lower-performance group (LP group).
Experimental Tasks
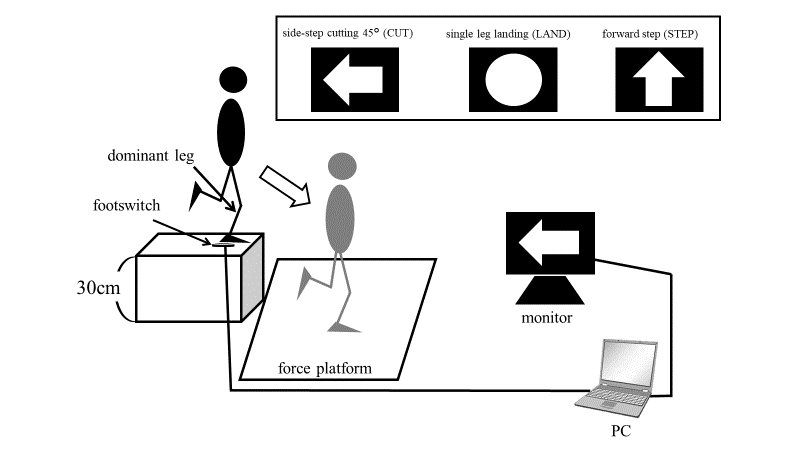
The experimental task involved a single-leg drop-jump task from a 30-cm high box using only the dominant leg, followed by three types of unanticipated tasks: side-step cutting, single-leg drop-jump landing, and forward stepping. The dominant leg was defined as the leg with which the participants preferred to kick a ball. In this study. Only the single-leg drop-jump landing task was analyzed, since side-step cutting motion had been previously verified.10
First, the participants stood on single-leg with the dominant leg on a 30-cm high box placed at the edge of the force platform. They then jumped down toward the center of the force platform and landed on their dominant leg. Immediately after leaving the box, one of the tasks was randomly presented on the personal computer (PC) monitor, and the participants were instructed to execute the one of three task before contact on the force platform. (Figure 1).

In the single-leg drop-jump landing task, the participants were required to maintain a single-leg standing position for two seconds after landing. During the experimental task, both hands were kept on the iliac crests. A failed trial was defined as a case in which participants were unable to maintain a standing position with a single leg for two seconds after landing, if their free leg made contact with the ground, or if their upper limb separated from the waist due to significant rotation and lateral flexion of the trunk. The experiment was terminated when participants successfully completed at least three trials, and the mean values over the three trials for the analysis. Prior to the actual experiment, participants performed five practice trials until they were comfortable with the tasks after sufficient warm-up. The specific content of the warm-up was not specified, and participants were instructed to perform their usual warm-up routine for approximately 15 to 20 minutes.
Data Collection and Processing
A three-dimensional motion analysis system, the VICON MX motion analysis system (VICON, Oxford, UK), was used to capture the tasks using 10 infrared cameras with a sampling rate of 250 Hz. Thirty-five retroreflective markers were placed over the whole body of each participant, according to the standard Plug-in Gait model (Helen Hays marker-set). GRF data were obtained at 1,000 Hz from two force platforms (Kistler Instruments, Inc. model 9281C, Winterthur, Switzerland), which were synchronized with the kinematic data. Joint moments were calculated on the side of the dominant leg using a full inverse-dynamic model implemented using the VICON Plug-in Gait. The estimated joint moments were normalized to the body mass of the participants. The joint angles were calculated for the trunk, pelvis, hip joint, and knee joint, while the joint moments were calculated for the hip and knee joints.
Surface electromyography (EMG) data were recorded at 1,500 Hz using a seven-channel EMG system (Telemyo DTS, Noraxon Inc., Scottsdale, AZ, USA) and collected synchronously with motion and force platform data. Bipolar surface electrodes (Ag-AgCl) were separated by 2 cm and placed on the following seven muscles: gluteus medius (GM), adductor longus (Add), rectus femoris (RF), vastus medialis (VM), vastus lateralis (VL), biceps femoris (BF), and semimembranosus (SM). Each electrode was placed as follows: GM, approximately 2 cm below the midpoint of the iliac crest over the muscle belly; Add, approximately 10 cm below the pubic symphysis over the muscle belly; RF, approximately halfway between the upper patella and the anterior superior iliac spine over the muscle belly; VM, approximately 5 cm from the medial patella at 45° over the muscle belly; VL, approximately two-third distal to the point between the patellar lateral side and the anterior superior iliac spine over the muscle belly; SM and BF, approximately halfway between the tibial lateral epicondyle and the ischial tuberosity over the muscle belly. The skin was shaved and cleaned with an alcohol swab before electrode placement.
Data Analysis
The raw kinematic and GRF data were filtered based on a frequency content analysis of the digitized coordinate data. Marker trajectories were filtered at 7 Hz using a 4th-order Butterworth filter with VICON Nexus 1.6.1 software (Oxford Metrics Ltd., UK). Since ACL injury has been reported to occur around 40 ms after IC,24 the analysis window of this study was set from IC to 40 ms. For the analysis of joint angles, the joint angular changes within the analysis window were calculated. Joint moments were calculated by determining the maximum value within the analysis window and using it for the analysis. The IC was defines as the time at which vertical GRF was higher than 10 N.
For EMG data, the stored raw signals were band-pass filtered (20-500 Hz), and root mean square (RMS) processed with a 10 ms time constant using Myomuscle (Noraxon Inc., Scottsdale, AZ, USA). Prior to data collection, the RMS data were normalized using the maximum voluntary contraction (MVC) for each muscle (%MVC). The MVC was recorded for five seconds, and the average amplitude was determined from the stable RMS for three seconds. The average activity of the knee flexors (HAM) was calculated from the BF and SM, and activity of the knee extensors (QUAD) was calculated from the VM and VL. The co-contraction ratio (CCR) was calculated as the relative muscle activity of QUAD to HAM.25 EMG data were recorded for 50 ms before IC (pre-IC), as in the previous study.26 I chose 50 ms before IC because this is suitable for evaluation of an individual’s pre-planned muscle recruitment strategy. The authors chose 50 ms after IC to assess muscle activation immediately after IC (post-IC). The analysis of muscle activity immediately after IC was conducted to analyze the muscle activity that occurs near the potential timing of ACL injury.
Statistical Analysis
Results are presented as means ± standard deviation (SD). Initially, the Shapiro–Wilk test was conducted to check the normality of each measurement. There were no variables for which normality could not be confirmed. Independent t-tests were utilized to compare the differences between the LP and HP groups with respect to the SDMT scores, age, height, body weight, joint angular change, peak joint moment, and muscle activities. The effect size (Cohen’s d) was also calculated and interpreted as weak (0.20), moderate (0.50), and strong (0.80). Statistical significance was set at p < 0.05. All statistical analyses were performed using SPSS Statistics 22.0 (IBM, SPSS Tokyo, Japan).
RESULTS
Means and standard deviations for these participants were: age of 20.1 ± 1.3 years, height of 166.6 ± 7.3 cm, weight of 60.6 ± 6.9 kg. For all participants, the mean SDMT score was 71.5 ± 7.5, with a median score was 70. The SDMT score in the HP group was significantly higher than that of the LP group (HP: 77.9 ± 5.5; LP: 66.0 ± 3.4; p < 0.001) (Table 1).
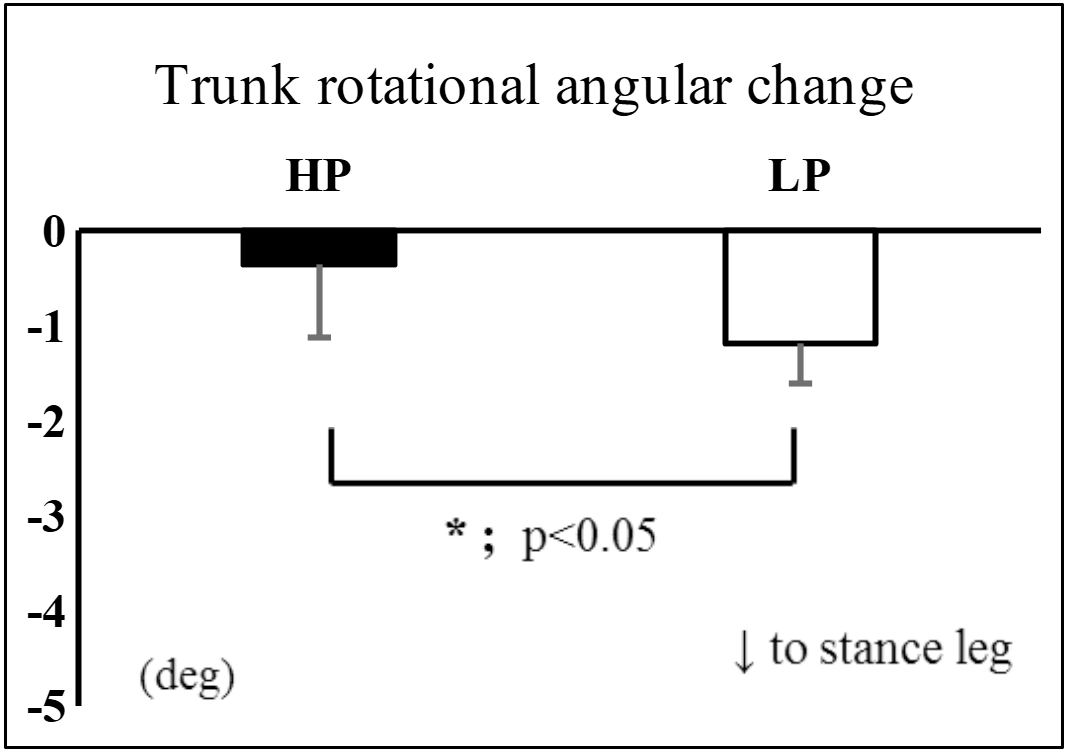
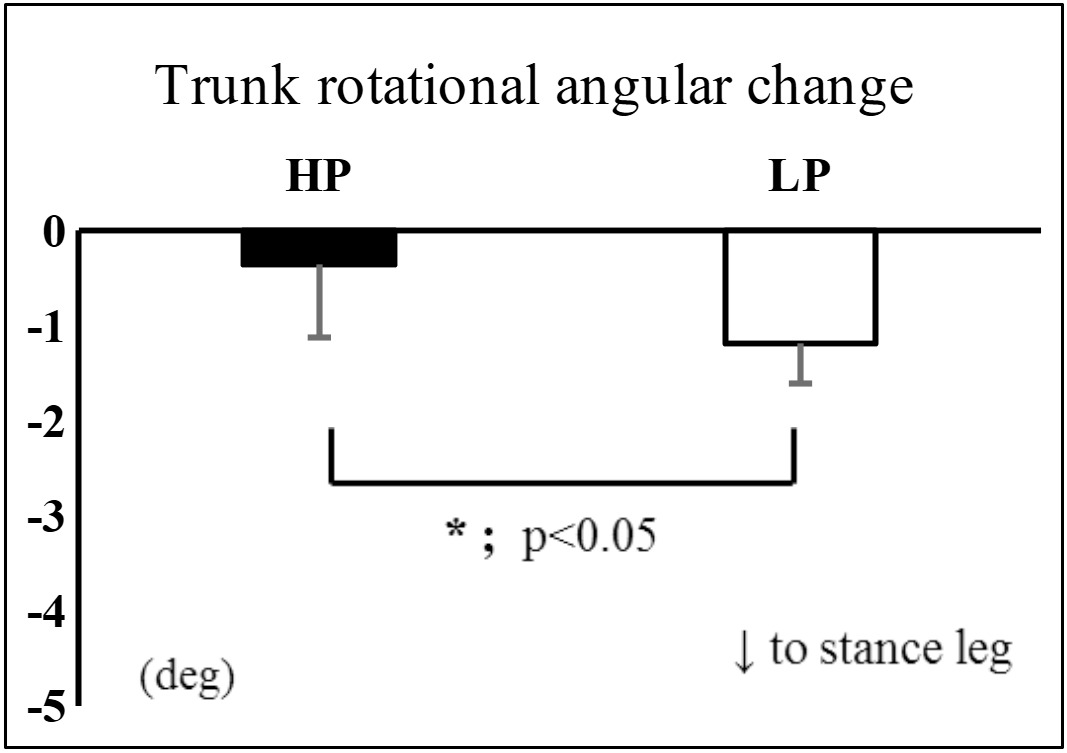
The LP group exhibited a significantly greater trunk rotation angular change toward the stance leg side compared to the HP group (HP: 0.4 ± 0.8; LP: 1.2 ± 0.4; p = 0.020) (Figure 2). There were no significant differences between the two groups in terms of joint moments, and muscle activities (Tables 2, 3). However, the large effect sizes were observed in the pre-IC CCR (HP: 145.0 ± 113.4%; LP: 74.6 ± 17.5%; p = 0.112. d=0.89) (Table 4).
DISCUSSION
This investigation was conducted to examine the influence of neurocognitive function differences, as measured by SDMT, on kinematics, kinetics, and muscle activation during single-leg drop-jump landing followed by an unanticipated task in female athletes. The findings revealed that the LP group exhibited a significantly larger trunk rotation angular change to the stance leg side during the early landing phase.
Trunk position variations have been reported as potential risk factors for ACL injuries. Previous analyses of single-leg drop-jump landing and cutting motions have indicated a consensus that limited trunk forward flexion and increased lateral trunk flexion towards the injured leg side are associated with a higher risk of ACL injury.27–29 However, there have been inconsistent findings regarding trunk rotational movement. Several authors have observed trunk rotation away from the injured leg at the time of ACL injury.30–32 Critchley et al.33 demonstrated that axial trunk rotation during double-leg landing leads to decreased knee flexion angles, increased peak impact vertical GRF, internal knee extension moments, and increased knee abduction and internal rotation angles for the ipsilateral leg when compared to the neutral trunk condition. Furthermore, it has been suggested that cutting motions involving trunk rotation and lateral flexion in the direction of cutting may reduce the risk of ACL injury and enhance performance.34 In the current study, participants with lower neurocognitive function exhibited a greater change in trunk rotation angle towards the stance leg side during the early landing phase. Therefore, it is plausible that differences in neurocognitive function are linked to variations in motor strategies of the trunk in the horizontal plane during single-leg drop-jump landing. However, the precise effect of trunk and pelvis movements in the horizontal plane on the occurrence of ACL injuries remains unclear or the amount that is potentially injurious is also not known. Furthermore, the amount of trunk rotation angular change observed in this study was very small and may not be clinically significant. Future studies should concentrate on investigating trunk and pelvis rotational movements and their relationship to the risk of ACL injury.
In this study, a large effect size was observed in the pre-IC CCR, indicated that the LP group had relatively larger quadriceps muscle activity relative to the hamstring just prior to landing. Many previous studies have pointed out that an imbalance between quad and ham muscle activity during landing may induce ACL injury, and in particular, activity with a predominantly large quadriceps muscle is considered dangerous.35 Therefore, I would say that the muscle activity observed in this study is muscle activity at high risk for ACL injury.
It is thought that the neurocognitive functions required for athletes were: selective attention for simultaneously processing various information at all times, and instantly performed IPS in a limited time.4,36 The authors thought that the SDMT could measure the neurocognitive functions required during sports activities of athletes because it could measure functions such as the ability to IPS and selective attention.12,37 Another reason for employing SDMT in the current study is that it can evaluate neurocognitive function without the need for specialized equipment before sports activities. Previous research investigating the effects of neurocognitive function on landing and cutting motions have utilized computer tests such as CRI and ImPACT, with no reports using paper-and-pencil tests. Computer-based tests offer the advantage of simultaneously measuring multiple components of neurocognitive function separately. However, they require special equipment and are difficult to administer easily before engaging in sports activities. This study proposes that differences in SDMT scores, which can be easily assessed before sports activities, may be associated with changes landing mechanics representing the trunk rotation angle during single-leg drop-jump landing followed by an unanticipated task.
Although the current study identified differences in trunk rotation angles during single-leg drop-jump landing followed by an unanticipated task between groups based on SDMT scores, no variations were observed in other kinematic, kinetic, or muscle activity parameters due to differences in neurocognitive function. This may be attributed to the relatively high mean SDMT scores of the participants in our study. The mean SDMT score for all participants in this study was 71.5 ± 7.5, the mean for the LP group was 67.3 ± 5.0, and the lowest score was 61. In comparison, previous studies reported a mean SDMT score of 58.2 ± 9.1 (range = 51.87-63.93) for young adults (< 30 years),22 and 53.06 ± 11.50 for male college athletes.23 Therefore, the current study participants exhibited good SDMT scores, and may represent the absence of individuals with low neurocognitive function which may have contributed to the lack of group differences in lower limb mechanics during single-leg drop-jump landing motion. Because ACL injuries occur more frequently in athletes involved in sports activities and less frequently in the general population,38 it was appropriate to focus on highly competitive athletes. The results of the current study suggest that SDMT may be too easy of a task for assessment of neurocognitive function healthy competitive athletes. Future investigations should examine which tests are more likely to identify neurocognitive differences among competitive athletes by employing additional paper-and-pencil tests such as the Trail Making Test or the Stroop Interference Test.
Limitation
This study had several limitations. Firstly, the method used for simulation during the unanticipated tasks used in this study was to display a symbol such as a simple arrow on a monitor. This stimulus method was not necessarily consistent with a situation during actual games and might be too simple. To create tasks more closely resembling real sporting scenarios, it may be necessary to employ images of games, models of opposing players, or virtual reality images. Secondly, the authors selected the single-leg drop-jump landing motion from the platform as the experimental task, but this is not a motion that occurs during sports activities. In this study, the simple single-leg drop-jump landing motion was analyzed to examine the effect of neurocognitive function on the motion as directly as possible. Future studies should incorporate tasks that more closely align with sports activities, such as landing from a rebound in basketball, landing from a header in soccer, or cutting from a dribble. Thirdly, there is always a problem of reliability in three-dimensional motion analysis using surface markers. It has been reported that the use of body surface markers during motion analysis may cause errors in recording actual joint motion , because the position of the marker shifts on the skin.39 Therefore, it is important to recognize that the joint angular changes in the current study may contain some measurement errors. Lastly, the small sample size resulted in insufficient statistical power. However, since there were several items with large effect sizes, it is possible that different results could be obtained by increasing the number of participants. Future studies should strive to enhance the generalizability of my findings by increasing the sample size and conducting similar analyses on male athletes.
CONCLUSION
The female athletes who had low SDMT scores had a statistically greater amount of change in the trunk rotation angle toward the stance leg side during single-leg drop-jump landing followed by an unanticipated task. However, there were no significant differences in other kinematic, kinetic, or muscular activation values due to differences in neurocognitive function. Therefore, differences in neurocognitive function as measured by SDMT affect horizontal trunk movement during single-leg drop-jump landing followed by an unanticipated task, but the relationship with ACL injury risk is not clear.