INTRODUCTION
There are over 120,000 anterior cruciate ligament (ACL) tears per year in the United States.1 In athletes, the majority of these tears are addressed with ACL reconstruction (ACLR) surgery.2 Post-surgical rehabilitation attempts to restore knee function and promote return to activities of daily living (ADLs) and sport. However, despite surgery and rehabilitation, outcomes after ACLR may not be optimal. A systematic review of prospective studies found that 5.8% of patients sustained an ipsilateral ACLR autograft failure and 11.8% of patients had an ACL tear in the contralateral limb within the first five years after surgery.3 Ardern et al. reported that while 74% to 87% of patients returned to sports, only 59% to 72% of patients returned to their pre-injury sport, and only 46% to 63% of patients returned to competitive sports.4 Furthermore, fear of re-injury may contribute to the inability to return to sport. Kvist et al. found in a survey of patients after ACLR, of the 47% that had not returned to their pre-injury activity, with 24% of those patients reporting fear of re-injury as the reason.5
To optimize outcomes, sports medicine and rehabilitation professionals should attempt to restore patients to their prior level of function, including pre-injury physical and psychological performance. Clinicians may use return to sport (RTS) testing batteries to measure these outcomes and guide rehabilitation and return to sport after ACLR.6–10 A common return to sport test battery may include a series of horizontal and vertical hops.6,11–16 These tests are proposed to evaluate lower extremity status in a manner that is relevant to athletic ability by assessing dynamic movement in multiple planes.6,11,15 Patient reported outcome measures (PROMs) such as the Anterior Cruciate Ligament – Return to Sport Index (ACL-RSI) may also be included in RTS testing batteries after ACLR to quantify subjective information regarding patients’ psychological status, an area of paramount importance that may influence return to play ability and fear of re-injury.17–22
Many other RTS tests have been described to assess various physical, neurocognitive, and psychosocial outcomes however it is difficult to design the optimal RTS battery as the evidence is emerging (and is mixed) regarding the association between RTS testing, successful return to play, and future injury risk.23 Sports medicine and rehabilitation professionals must balance the challenges of clinical practice with a detailed understanding of RTS testing options in order to provide optimal care to patients after ACLR.23–30
Despite the challenges of RTS testing, hop testing and collection of PROMs are simple, low cost, and easy to perform in the clinic. They have demonstrated appropriate reliability and validity to evaluate outcomes after ACLR.18,31 The purpose of this study was to examine the relationship between patient-reported ACL-RSI scores and limb symmetry indices (LSIs) for single hop for distance (SHD), triple hop for distance (THD), crossover hop for distance (CHD), timed 6-meter hop (T6H), and single leg vertical hop (SLVH) in a cohort of National Collegiate Athletic Association (NCAA) Division 1 collegiate athletes after ACLR. Further research into the intersection between psychological status and functional performance may provide valuable insight into drivers of optimal outcomes after ACLR. The hypothesis was that SLVH LSI would be more highly correlated with ACL-RSI score than all other hop tests after ACLR as its vertical component may better reflect perceived knee function and influence self-reported psychological status.
METHODS
Participants
A retrospective review was conducted to examine a consecutive series of patients between August 2018-May 2022 who met the inclusion criteria of 1) being an NCAA Division 1 collegiate athlete referred one of two Sports Medicine practices and 2) having undergone unilateral ACLR. Patients were excluded from the study for 1) a history of prior ACLR to either knee or 2) any other lower extremity musculoskeletal surgery within the previous two years. Based on previous studies, an a priori power analysis was conducted to determine that a sample size of 14 was required to detect an effect size of 0.8 for the primary outcome measure, ACL-RSI, with α ≤ 0.05 and a power (1- β) = 0.80.11,14 The Institutional Review Board at the University of Maryland determined this study to be exempt.
Procedures
Demographic and outcomes data were extracted and de-identified from subjects’ electronic medical records. Demographic data is included in Tables 1 and 2. Outcomes included LSI for SHD, THD, CHD, T6H, and SLVH and ACL-RSI score and are reported in Table 3. Data were collected as part of usual clinical practice by two physical therapists who are board-certified in either sports or orthopedic physical therapy and each have over nine years of experience working with patients with ACL injuries.
Testing procedures for hop tests included standardized instructions, warmup, and two practice trials followed by two test trials. Test trials were averaged and included in statistical analysis.6,31 The testing order began with the SHD, THD, and CHD which were performed over ground and measured with a tape measure. The T6H followed and was performed over ground and measured with the stopwatch function on a smart phone. The SLVH was last and was performed using the Just Jump System (JJS, Probotics Inc, Huntsville, AL, USA), a commercially available jump mat that calculates jump height and is valid when compared to three-camera motion analysis.32
For all hop tests, LSIs were calculated by dividing the result on the involved limb by the result on the uninvolved limb and multiplying by 100 to produce a percentage, except for the T6H, when the numerator and denominator were reversed as a lower time indicates better performance. For all hop tests, an LSI less than 100% indicates a worse performance on the surgical limb compared to the non-surgical limb while a value greater than 100% indicated better performance on the surgical limb compared to the non-surgical limb.
The ACL-RSI is a twelve-item PROM that evaluates emotions, confidence in performance and risk appraisal and has been validated for use after ACLR.18 It was administered electronically using a smart phone application after all completion of all hop tests with the final score expressed as a percentage out of 100% (Felipe Andai Ignacio, Orthosoft ©).18 A higher percentage on the ACL-RSI indicates greater psychological function in the context of return to sporting activity.
Statistical Analysis
Descriptive statistics (means and standard deviations) were calculated for demographic data and all dependent variables (hop test LSI and ACL-RSI score). Normality of the primary outcome measures was assessed using Shapiro-Wilk test. Due to a significant Shapiro-Wilk test for five of the six variables (indicating non-normal nature of the data), a non-parametric Spearman’s Rho correlation coefficient was used to determine if a significant relationship exists between LSI for each hop test and ACL-RSI. Significance level was determined a priori as p ≤ 0.05. Correlations were qualified as very strong (r = 0.90-1.00), strong (r = 0.70-0.89), moderate ( r= 0.40-0.69), weak (r = 0.10-0.39) or negligible (r = 0.00-0.10).33
Finally, LSI variables determined to have a significant correlation with RSI were then utilized in a step-wise linear regression model to determine which hop tests (independent variables) best predicted the ACL-RSI (dependent variable). All statistical analyses were performed using SPSS version 28.0.0.1 (14) (IBM Corp.).
RESULTS
A total of 21 patients (7 males, 14 females) with an average age of 20.38 ± 1.67 years were included (Table 1). Sport played by each patient is displayed in Table 2. All patients had undergone primary ACLR with bone-patellar tendon-bone autograft and were an average of 6.62 ± 1.69 months since surgery. Descriptive statistics (means and standard deviations) for all outcome measures are included in Table 3.
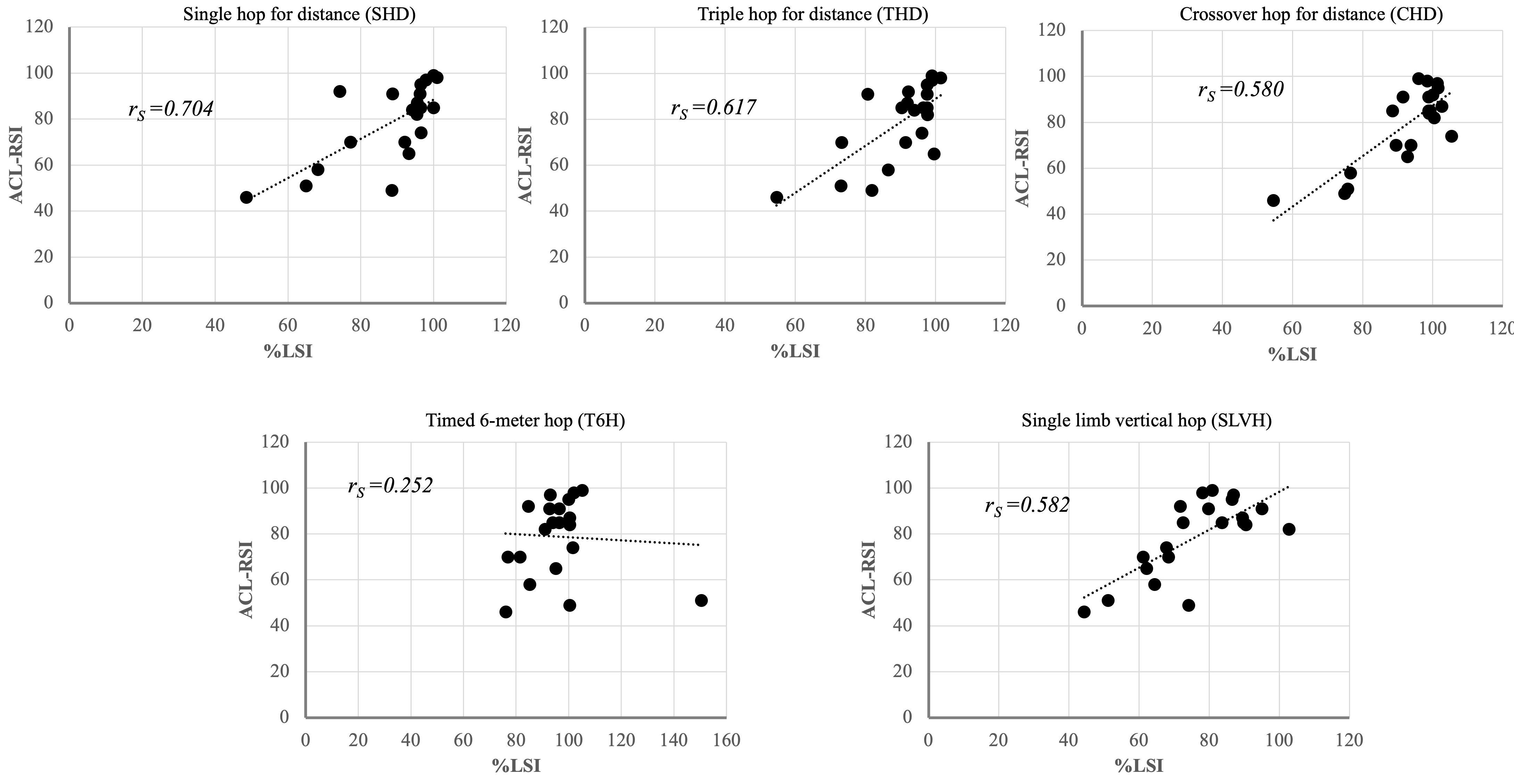
There were significant correlations found between ACL-RSI and SHD, THD, CHD, and SLVH (Figure 1). Overall, the correlation was strong when comparing ACL-RSI and the LSI for SHD (rs = 0.704, p < 0.001), moderate when comparing ACL-RSI and the LSI for THD (rs = 0.617, p = 0.003), CHD (rs = 0.580, p = 0.006), and SLVH (rs = 0.582, p = 0.006). There was a poor correlation (non-significant) between ACL-RSI and the LSI for the T6H (rs = 0.252, p=0.271).
.png)
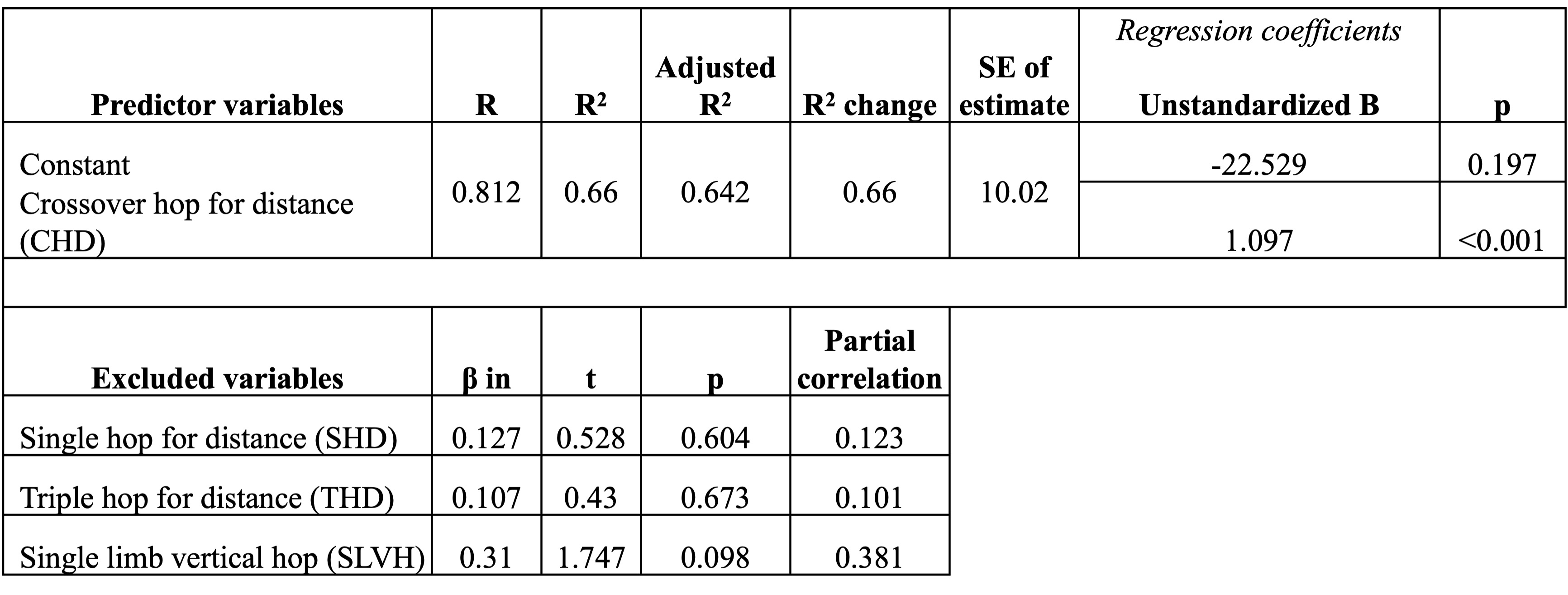
While the LSI for SHD, THD, CHD, and SLVH were significantly correlated with ACL-RSI, when all four of these variables were entered into the stepwise regression model, only CHD remained in the model as a significant predictor for the primary outcome of ACL-RSI. The CHD explained 66% (R2 value of 0.660) of the variance in ACL-RSI (Table 4).

DISCUSSION
The initial hypothesis that SLVH LSI would be more highly correlated with ACL-RSI score than all horizontal hop tests was not supported. The correlation between ACL-RSI and SLVH was moderate, as were the correlations between ACL-RSI and THD and CHD. The correlation was strongest between ACL-RSI and SHD. Additionally, the CHD explained 66% of the variance in ACL-RSI and was the strongest predictor variable shown in the regression analysis.
The SHD, THD, and CHD require the patient to decelerate horizontal momentum in the sagittal plane.34 These tests may simulate deceleration and landing in the context of sport and explain their correlation with ACL-RSI. Furthermore, the patients can self-reflect on their outcomes as the tape measure in the testing area provides immediate feedback regarding hop distance while providing an external focus of attention. The perception of successful performance on horizontal hop tests may influence ACL-RSI scores as patients may be more likely to believe that they will perform well on deceleration and landing tasks in sport.
Furthermore, the CHD provides an additional challenge to frontal and transverse plane stability that may be more related a change of direction or cutting activity, directly stressing the function of the ACL.6,35 Approximately 70% of ACL injuries are non-contact and caused by multidirectional forces during landing, cutting, and deceleration movements during sport.36–38 Patients may be familiar with these tasks and their relationship to injury mechanism which may indicate why performance on the CHD explained approximately two-thirds of the variance in ACL-RSI score and remained the best predictor variable in the overall regression model.
Despite not demonstrating the highest correlation with ACL-RSI, the SLVH was moderately correlated and does carry clinical value. For example, this test requires concentric impulse to achieve high jump heights, likely making it a good proxy for quadriceps function which may influence overall psychological status.11,13,14,16,39,40 Previous research has demonstrated that SLVH is sensitive to capacity at the knee joint and patients typically exhibit greater asymmetries when compared to horizontal hop tests suggesting it is relevant to a comprehensive evaluation.11,14,16
Testing order may also have affected the results as SLVH was performed as the final hop test. Though there has been no published research specifically evaluating the effect of test order on performance after ACLR, there is evidence that neuromuscular fatigue can diminish functional performance, knee stability, and increase forward tibial translation.41 This is problematic as authors have proposed that neuromuscular fatigue is a risk factor for ACL injury and re-injury.42 Interestingly, during RTS testing, fatigue may decreased performance more in the involved limb than the involved limb after ACLR.43 In the case of the present study, SLVH performance could be decreased on the uninvolved limb as it was tested last, altering LSI asymmetry. This may result in a weaker correlation and variance relationship with ACL-RSI compared to horizontal hop tests performed earlier in the testing battery and should be considered in future studies.
Criterion- and performance-based testing remains a critical component of the return-to-sport process. Without these objective measures, the clinical decision process would rely on time since surgery or other non-performance related factors.44 However, there is considerable need to optimize criterion-based return-to-sport testing batteries that typically include a series of strength, performance, neurocognitive, and patient reported outcome measures. Webster and Hewett indicate that only 23% of athletes fully pass a testing battery before returning to sport.23 Further, passing a return-to-sport test may not reduce the overall risk of a subsequent ACL injury, potentially reducing the risk of graft rupture but increasing the risk of contralateral injury.23 A 2021 consensus statement suggested that return-to-sport testing should also involve the assessment of specific functional skills, psychological readiness, and contextual factors such as type of sport, time of season, and level of competition.44
Both the ACL-RSI and single-leg hop tests used in this study can inform return to play decisions. They require minimal equipment or expertise to reliably carry out in a standard clinical setting. Most standard paradigms utilize distances or LSIs as outcome measures of these hop tests, though advanced technology like three-dimensional motion capture systems and force platforms may allow for more discrete measures and analysis and may become more available in the future.45,46
While the data and interactions between ACL-RSI and hop tests is interesting, there are several limitations to consider. First, the study was retrospective in nature, which could introduce selection bias and is limited by the accuracy of the electronic medical record. Strict inclusion and exclusion criteria and careful data extraction by two authors were emphasized to reduce error. Similarly, despite exceeding the number of subjects determined by power analysis, the sample included twice as many females than males and were all NCAA Division 1 collegiate athletes; therefore, the results cannot be generalized to all patients after ACLR. Lastly, as psychological status is multifactorial, the present study is unable to draw conclusions regarding several important variables such as gender, injury mechanism, or playing surface, which likely have a large influence on ACL-RSI. Future studies should investigate these variables to improve the overall understanding of predictors of psychological status after ACLR.
CONCLUSION
The results of this study suggest that physical function has the capacity to influence psychological status after ACLR. To improve outcomes, clinicians should consider this important relationship and recognize that SLVH, SHD, THD, and CHD are correlated with ACL-RSI but the psychomotor properties of each test likely relate to their clinical utility. Specifically, CHD explained the greatest variance in ACL-RSI and may be relevant due to the multiplanar nature of ACL injury. All horizontal hop for distance tests are valuable in that deceleration and landing in the sagittal plane are important qualities to consider as well. The clinical relevance of SLVH lies with its ability to assess knee function with a vertical propulsion bias. Lastly, the T6H did not correlate with ACL-RSI however continuous hopping for speed may still be part of the overall clinical picture. All together these tests appear to influence ACL-RSI through different, yet converging, avenues and carry value as combing them may enhance the robustness of clinical assessment after ACLR. Clinicians should consider the emerging data regarding the benefits and shortcomings of various hop tests to promote a comprehensive approach to rehabilitation and optimize outcomes after ACLR and better appreciate the intersection between physical and psychological function.
Conflicts of interest
The authors have no conflicts of interest to report.