



Introduction
Ankle sprain is the most common sports injury1 and it becomes recurrent when sensorimotor dysfunction persists including muscle weakness and/or impaired processing of somatosensory information.2,3 Sensorimotor dysfunction that occurs after an initial ankle sprain alters an individual’s ability to stabilize the ankle joint which impairs dynamic postural control.2,4–6 People who develop this dysfunction after ankle sprains are commonly described as having “ankle instability.”2,4 Thus, current clinical practice guidelines recommend assessing dynamic postural control in people with ankle instability to determine their risk for recurrent injury.7
A scoping review revealed that clinicians and researchers commonly assess dynamic postural control in people with ankle instability by measuring the maximum reach distance (MRD) of the posteromedial reach direction of Y-Balance Test (PM-YBT).8 The PM-YBT requires a person to maintain balance while they stand on a single limb and reach their opposite limb as far as possible in a posteromedial direction.9 While the MRD of the PM-YBT provides a measure of dynamic postural control that distinguishes people with ankle instability from healthy people,10,11 it remains to be shown whether motor output or sensory processing3 predict MRD performance. Thus, to better understand the extent that PM-YBT performance reflects underlying ankle impairments, there is a need to determine the influence of deficits in muscle activation or sensory processing on MRD. A previous study showed that artificial disruption of somatosensory input in healthy people decreases the MRD of PM-YBT by 4.6%.12 It remains to be shown whether torque control of ankle musculature contributes to PM-YBT performance.
In general, the ability to accurately control ankle torque in isometric and isotonic contractions is necessary to maintain single limb stability. The relationship between maximum isometric ankle torque and dynamic postural stability was investigated by Chtara et al13 who showed that maximum isometric torque of ankle dorsiflexion and plantarflexion explained 21-30% of the MRD of the PM-YBT. However, that study did not show consistent results between the dominant and non-dominant stance limbs and torque was assessed with a handheld dynamometer.13 In addition, Hubbard et al14 found that concentric ankle torque does not relate to dynamic postural control in people with ankle instability. While concentric torque does not explain YBT performance and isometric ankle torque may partially explain YBT performance, the ability of eccentric ankle torque to predict dynamic postural control is not known.
Eccentric activation of lower extremity muscles is necessary during most athletic movements.15,16 The ability to eccentrically control the ankle joint is also necessary to maintain balance during single limb stability.17 For example, performance of the PM-YBT requires eccentric activation of ankle musculature acting in the sagittal plane to stabilize the ankle joint during the reaching phase.12,18 Taken together, the ability to modulate eccentric muscle force at the ankle joint may be an indicator of dynamic postural control assessed by the PM-YBT. To our knowledge it is currently unknown whether the ability to control eccentric ankle torque output is predictive of YBT performance.
Therefore, the purpose of this study was to determine whether the ability to accurately control eccentric ankle torque explained PM-YBT performance. It was hypothesized that eccentric dorsiflexion/plantarflexion torque control would be positively related to the MRD of PM-YBT.
Materials and Methods
PARTICIPANTS
Twelve healthy subjects were recruited for the study. Subjects with a history of lower extremity surgery, injuries in the six months prior to the study, or neurological disease including balance impairments were excluded. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the Juntendo University (protocol ID: 2021-93; date of approval: 22 September 2021). The subjects signed the informed consent before starting the test protocol.
PROCEDURES
A cross-sectional study was conducted. Before all testing, the subjects’ height (cm), body mass (kg), and limb length (distance from the anterior-superior iliac spine to the medial malleolus, cm) were measured. The testing limb was the dominant limb defined as the limb used to kick a ball. The subjects performed the PM-YBT, five-second maximum voluntary isometric contractions (MVIC) for both the dorsiflexors and plantarflexors, and then the torque control testing of the ankle. Subjects rested as needed between each testing.
DYNAMIC POSTURAL CONTROL MEASUREMENT
The YBT kit™ (Move2Perform, Evansville, IN), which contains a center board and indicator boxes with poles that indicate the reach distances in centimeters, was used to assess dynamic postural control ability (Figure 1). Only the posteromedial direction with the pipe positioned 135 degrees from the anterior pipe (PM-YBT) was used. The subjects were instructed to place the testing limb (stance limb) on the center board with their second toe positioned at the red line on the board and to push the indicator box as far as possible in the posteromedial direction. Before completing the PM-YBT trials, subjects were allowed to practice the PM-YBT task at least four times followed by a short rest break.9 While performing the PM-YBT, the subjects were asked to reach as far as possible while satisfying the following rules: (1) maintain hands on hips; (2) maintain the heel of the test/stance limb on the floor at all times; (3) complete contralateral limb maximum reach in three seconds; (4) avoid kicking, slinging, or putting too much weight onto the push box; and (5) return the reach limb to the starting position without losing their balance.

MAXIMUM VOLUNTARY ISOMETRIC CONTRACTION TESTING
The Biodex System 4 Dynamometer (Biodex Medical Systems Inc, Shirley, NY) was used to determine the isometric peak torque value for both dorsiflexion (DF-MVIC) and plantarflexion (PF-MVIC) muscle torque. The subjects were secured at the trunk, thigh, and foot with a belt and seated on the chair with 45◦ of seatback tilt, the hip in 80◦ flexion, and the tibia parallel to the floor. The ankle was in 0◦ for plantarflexion isometric torque testing and 10◦ of plantar flexion for dorsiflexion torque testing (Figure 2). Surface electromyography (EMG) data were simultaneously recorded for the tibialis anterior (TA) and soleus (SOL) muscles using wireless electrodes (Ultium EMG, Noraxon, Scottsdale, AZ, USA) placed according to SENIAM guidelines. Before affixing the electrodes, the skin was cleaned with alcohol. Bipolar surface electrodes (Ag/AgCl, 35 mm interelectrode center-to-center distance) were attached to the skin overlying the TA and SOL muscles. EMG signals collected at a sampling frequency of 2,000 Hz were synchronized with the data obtained from the dynamometer.

TORQUE CONTROL TESTING
The subjects performed the torque control testing in the same setup as the MVIC testing (Figure 2). The dynamometer provided five continuous ankle rotations through the defined range from 15° of dorsiflexion to 30° of plantar flexion (45° range) at 10°/s.19 Torque control was defined as the ability to match eccentric torque output to a target torque level. As the dynamometer moved the ankle into dorsiflexion, the subjects were instructed to eccentrically contract the plantar flexors to 50% of their maximum isometric plantarflexion torque, which was determined after pilot testing. As the dynamometer moved the ankle into plantarflexion, the subjects were instructed to eccentrically contract the dorsiflexors to 30% of their maximum isometric dorsiflexion torque. The target torque level and the subject’s generated torque were displayed on a computer monitor (size: 27 inch) for visual feedback. The torque produced by the subject, the target torque, and the joint angle were collected at a sampling frequency of 100 Hz. Muscle activities of TA and Sol were simultaneously recorded during the torque control testing and synchronized with the data from the dynamometer using an analog to digital data acquisition (DAQ) board (2400 ISO, Noraxon, Scottsdale, AZ, USA). Prior to the testing, the subjects were allowed to practice five continuous ankle rotations in the sagittal plane for both plantarflexion and dorsiflexion. Each testing trial took approximately 22.5 second (10°/s, five rotations though 15° of dorsiflexion to 30° of plantar flexion).
DATA PROCESSING
Maximum reach distances of the YBT were recorded in centimeters, normalized to leg length, and multiplied by 100 (PM-MRD, %). Three scores from successful trials of the PM-YBT were recorded. The mean value of the three PM-MRD was used for data analysis. The isometric peak torque value for both DF-MVIC and PF-MVIC was normalized by subjects’ body mass (Nm/kg). Accuracy of eccentric torque control was calculated as the absolute error between the target torque and the produced torque (AE, Nm). While the torque control assessment occurred from 15° of dorsiflexion to 30° of plantarflexion (45° range), AE was analyzed from 10° of the dorsiflexion to10° plantarflexion (20° range) during the ankle rotation.19 For both torque accuracy of dorsiflexion (AE-DF) and plantarflexion (AE-PF), the area between the target torque and the produced torque within the analysis range was used to assess the performance of torque control (Figure 3). Out of the five torque control trials, the mean AE-DF/AE-PF from the middle three trials (trials 2,3,4) was used for data analysis. Muscle activity during the torque control task was measured as the mean EMG within the analysis range which was normalized and expressed as a percentage of muscle activity obtained from the MVIC (EMG-TA; EMG-SOL, %MVIC). All EMG signals were subsequently bandpass filtered (between 20 and 500 Hz) with a 2nd order filter on the high-pass and a 4th order filter on the low-pass. All the data were analyzed offline using a custom-written program in MATLAB (The MathWorks, Natick, MA, USA) and confirmed visually for each trial. Figure 3 depicts a representative example of a subject’s produced torque, target torque, and EMG recorded during eccentric dorsiflexion torque control testing.

STATISTICAL ANALYSIS
A simple linear regression was used to test whether eccentric dorsiflexion/plantarflexion torque accuracy predicted the PM-MRD performance. A stepwise linear regression model with all of the assessed variables (DF-MVIC, PF-MVIC, AE-DF, AE-PF, EMG-TA, EMG-SOL) was then run to determine whether isometric strength or muscle activity during the torque control task contributed to the prediction of dynamic postural control. Pearson product-moment correlation coefficients (r) were calculated during the process of computing the regression analysis. At each step, if a probability of F value satisfied the entry criterion (p-value ≦ 0.05) or elimination criterion (p-value ≧ 0.1), the variable was entered in the model or removed from the model, respectively. Standardized partial regression coefficients (β) were calculated to compare the degree that the independent variable influenced the dependent variable. Coefficients of determination (R2) were used to interpret the meaningfulness of the relationships. As a secondary analysis, a simple linear regression was used to examine whether muscle activity during the torque control task explained eccentric dorsiflexion/plantarflexion torque accuracy. Mean and standard deviations (SD) of all values were calculated. These analyses were completed using SPSS software (Version 28; SPSS Inc, Chicago, IL). The significance level was set at 0.05.
Results
The characteristics of the study participants were following: five females and seven males; age: 22.4 ± 2.2; weight: 63.6 ± 9.4 kg; height: 167.1 ± 8.0 cm. Simple linear regression revealed that the accuracy of torque control during eccentric dorsiflexion predicted a higher PM-MRD score (R2 = 44%, F1,10 = 7.94, β = -0.67, p = 0.02, Figure 4).

The accuracy of torque control during eccentric plantarflexion did not predict PM-MRD performance (β of AE-PF = 0.02, p = 0.94). Also, isometric strength and muscle activity during the torque control task did not contribute to the PM-MRD (β of DF-MVIC = -0.08, p = 0.82; β of PF-MVIC = 0.05, p = 0.87; β of EMG-TA = -0.29, p = 0.4; β of EMG-SOL = -0.02, p = 0.99). A step-wise linear regression model using all of the assessed variables revealed that only eccentric dorsiflexion torque control remained in the model. All relationships between the PM-MRD and independent variables are described in Table 1.
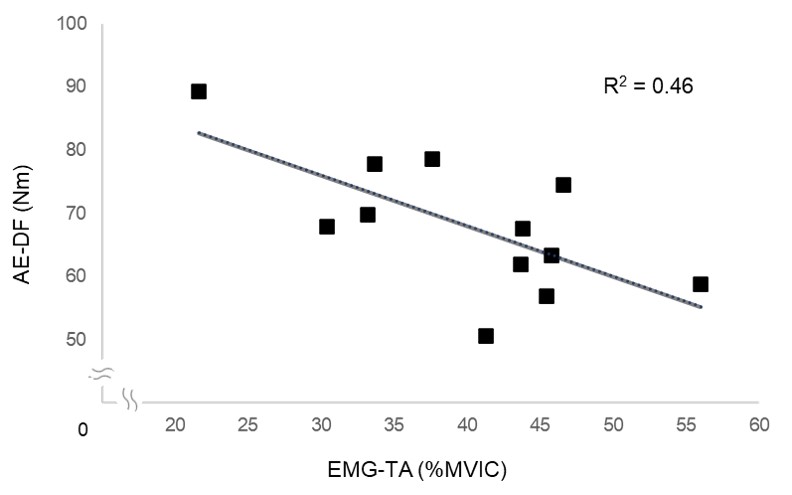
Simple linear regression for the secondary analysis revealed that higher muscle activity in tibialis anterior during the torque control testing predicted greater accuracy of torque control during eccentric dorsiflexion (R2 = 0.46, F1,10 = 8.4, β = -0.68, p = 0.02, Figure 5). The SOL muscle activity during the torque control testing did not explain the accuracy of torque control during eccentric plantarflexion (R2 = 0.002, F1,10 = 0.02, β = 0.04, p = 0.89). All mean and SD of each outcome measure are described in Table 2.

Discussion
This is the first study to show that accurate control of dorsiflexion torque relates to dynamic postural control as measured by the PM-YBT. As mentioned above, few studies have shown the relationship between sensorimotor function at the ankle and dynamic postural control as measured by the PM-MRD.3 The results of this study showed that the PM-MRD can be estimated by the accuracy of eccentric dorsiflexion torque control. In addition, it determined that greater accuracy of eccentric dorsiflexion torque control was predicted by greater activity of the tibialis anterior. Taken together, these findings indicate that the ability to activate and control ankle musculature as it is lengthening is important for dynamic balance.
The ability to control eccentric torque requires not only sufficient motor output but also adequate sensory processing. During the torque control test developed for this study, the subjects likely relied on sensory information from visual input (target torque and produced torque displayed on the screen) and somatosensory input (muscle spindles, Golgi tendon organs, cutaneous receptors).20 Thus, greater ability to control ankle torque output during an eccentric contraction, or lower AE as measured in this task, likely reflects accuracy in muscle recruitment and joint position sense.21–23
The current findings suggest that the ability to accurately control eccentric ankle dorsiflexion may play an important role in stabilizing the body during dynamic movement. The findings of Fournier Belley et al24 support the importance of precision sensorimotor function in the ankle dorsiflexors for maintaining dynamic postural control. They showed that the ability to detect a torque perturbation applied to the ankle dorsiflexors while they were passively lengthening was strongly associated with the PM-MRD score. Also, a recent systematic review25 revealed that during performance of the PM-YBT people with ankle instability do not activate tibialis anterior as much as healthy people, again highlighting the importance of this muscle in postural stability. In light of the findings, the detection and production of eccentric dorsiflexion may be an important indicator of one’s ability to control posture during dynamic movement.
Interestingly, the ability to accurately control eccentric plantarflexion did not predict the PM-MRD. The association between the posteromedial reaching task to eccentric torque control in dorsiflexion but not plantarflexion may be explained by differential actions of these muscle groups as the dorsiflexor muscles act in multiple planes but the plantar flexor muscles act in a single plane. This finding may be expected as ankle plantar flexors are activated similarly by healthy people and people with ankle instability during the PM-YBT.26 The lack of an association between soleus muscle activity and eccentric plantarflexion torque control may be due to contributions from other plantar flexor muscles. Also, this result suggests that the ability to accurately control eccentric plantarflexion torque (AE-PF) may not merely be influenced by soleus muscle activity.
Maximal isometric dorsiflexion and plantarflexion torques were not related to PM-YBT performance. Even more, the data suggests greater dorsiflexion torque was associated with worse PM-YBT performance although this did not reach the metric for significance (p=0.06, Table 1). These findings are contrary to those of Chtara et al.13 who showed moderate relationships between isometric dorsiflexion and isometric plantarflexion torques with the PM-MRD. This discrepancy is likely due to the differences in participant demographics and methodology as they assessed isometric torque of elite soccer players using a handheld dynamometer.13 The lack of relationships between isometric ankle torque and PM-YBT performance supports the premise of this study that when predicting postural control the ability to control muscle torque through a lengthening motion may be more important than other commonly assessed factors (isometric or concentric muscle strength).
One of the strengths of this study was that ankle torque was measured by an isokinetic dynamometer which is considered the “gold standard” device in the field of sports medicine.27 Previous studies that examined the accuracy of ankle torque control used a custom-built or robotic device,28,29 which are difficult to replicate by other researchers or clinicians. By using an isokinetic dynamometer, it can be confident in the reliability of the findings and this methodology may be more accessible for others to replicate.
Future studies investigating torque control capabilities in people with ankle instability will help to clarify the importance of this finding for predicting dynamic postural control in populations who are at risk for injury. These findings also raise the question as to whether eccentric torque control training improves postural control. Torque control testing relies on visual feedback, muscle sensory feedback, and neuromuscular excitability, all potential areas that may contribute to motor learning.30,31 To apply this idea in clinical practice, future studies need to examine the effectiveness of this approach as a sensorimotor control exercise to improve dynamic postural control for those who have ankle instability.32,33
LIMITATIONS
There are several limitations that need to be considered in the findings. The current study had a small sample size that limited the ability to establish correlations among all the assessed sensorimotor factors. However, this study was able to establish the relationship between eccentric ankle dorsiflexion torque control and PM-MRD which was the primary aim. Given that the model explained 44% of the variance in PM-MRD score, there are other variables that also need to be considered such as the vestibular system, cutaneous receptors, joint mechanoreceptors, or other measures of joint stability for future study. This study is specific to healthy people without neurological impairment which may limit the generalizability of these findings to people with balance disorders. A more comprehensive assessment of multiple sensorimotor factors with a larger sample size will further improve an understanding of factors contributing to dynamic postural control during the YBT. This study focused on ankle musculature, the primary area affected after ankle sprain, but knee and hip functions are also considered key contributors to the PM-MRD.34 Thus, eccentric knee and eccentric hip extension/flexion torque control may also be important to consider.16 Additionally, similar investigations of ankle inversion and eversion torque control may also provide important information regarding dynamic postural control ability.22,35,36 This initial study of eccentric torque control of ankle musculature, though small, provides the groundwork for future investigation that will continue to improve the understanding of contributing factors to postural control.
Conclusion
The accuracy of eccentric dorsiflexion torque control, which is influenced by the magnitude of tibialis anterior muscle activity, predicts better performance in the PM-YBT. The ability to control ankle torque eccentrically may be important for maintaining postural control during dynamic performance.
Disclosures
Shojiro Nozu received a research grant from JSPS KAKENHI (Grant Number: JP 21K21229), andYuji Takazawa received a research grant from The Joint Research Program of Juntendo University, Faculty of Health and Sports Science