
INTRODUCTION
When performing physical activities that include some element of a squat movement, such as barbell squats, deadlifts, or lunges, conventional wisdom dictates that the knee should remain aligned with the hips, ankles, and feet. That is, the knees should make minimal medial or lateral movement in either the descent or ascent phase of the exercise. However, medial displacement of the knee in the frontal plane, known interchangeably as medial knee collapse or knee valgus, has been historically considered one of the most common movement faults when performing squat-based exercises. This is potentially a problem for long-term knee health; considerable evidence has shown that greater knee valgus increases the risk of suffering a knee injury, namely anterior cruciate ligament (ACL) ruptures.1–5 Due to this risk, trainers, clinicians, and researchers have been motivated to find effective ways of correcting this movement pattern when it presents.6
It has been proposed that the use of an elastic band wrapped around the distal thighs might be such a method.7,8 It was argued that, by pushing the knees into further medial knee collapse (valgus), and providing the individual with enhanced proprioceptive input at the distal thigh, an elastic band might encourage greater muscle activation of the hip external rotators, which in turn assist in returning the knees back into a more neutral alignment. An elastic band would also hold the distinct advantage over other corrective options in that minimal instruction or feedback would be needed from a trainer or clinician. If the trainee is responding to the elastic band, and pushing their knees outwards against the external force, individuals could theoretically make corrective improvements in their technique with no additional supervision.
A number of investigations have reported seemingly conflicting findings on the usefulness of elastic bands during squat training, making it difficult to propose best practices for exercise prescription. On one hand, elastic bands wrapped around the thighs have become common within the fitness/strength training community in recent years for their perceived benefits, despite a lack of scientific findings showing clear and promising results. On the other hand, certain members of the research community have opposed the use of elastic bands in correcting medial knee collapse,9,10 given that some findings show elastic bands might actually increase knee valgus while performing squat-based movements.7–9,11,12 For example, Reece and colleagues9(p1) recently claimed, “Squatting with resistance bands is likely to increase the risk of knee injury. Coaches and clinicians who already implement this technique are advised to remove resistance band squats from training and rehabilitation programmes,” which is also unsupported (at least without considerable context) by current research.
Thus, the purpose of this narrative review is to examine current literature that has assessed lower limb muscle activity and/or lower limb kinematics performance on squat-based movements with or without an elastic band(s). The risks of medial knee collapse will be briefly discussed, as will the rationale for employing elastic bands as a corrective intervention. Most of this review’s attention will be directed to those studies which have directly examined the influence that elastic bands have on the lower limbs while performing squat-based movements, focusing primarily on measures of lower limb muscle activity and kinematics and the possible benefits and risks that utilizing elastic bands might have. Finally, recommendations for trainers/clinicians regarding elastic band usage and suggestions for future research directions will be discussed.
THE PROBLEM: DYNAMIC MEDIAL KNEE COLLAPSE
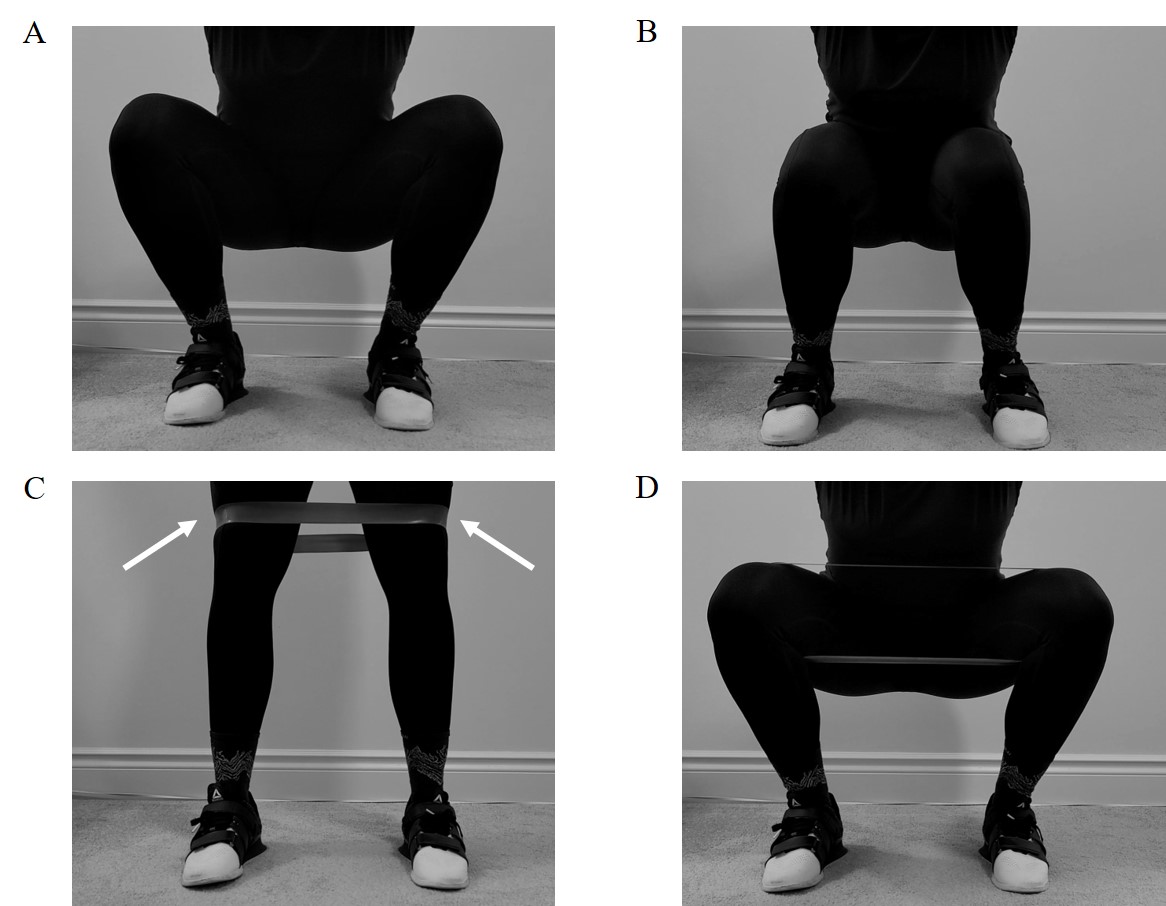
Dynamic medial knee collapse (knee valgus) occurs when an individual’s knee(s) move towards their body’s mid-line in the frontal plane13–15 (Figure 1B). In such an event, the knees are no longer aligned with the hips, ankles, and feet. This can place increased compression loads on the lateral compartment of the knee, and increased distraction loads on the medial compartment of the knee,4,5,16 which may increase the risk of developing lower extremity injuries, including anterior cruciate ligament (ACL) ruptures,2,17 patellofemoral pain,18–20 knee osteoarthritis,21 and knee cartilage and meniscus damage.14,22 For example, in a study that pre-screened 205 female athletes ahead of their competitive season by quantifying knee valgus angles while performing drop jumps, those who sustained ACL ruptures exhibited significantly larger knee valgus angles than those who were uninjured.2 Research has also demonstrated that preventative training measures, aimed at reducing knee valgus moments in individuals who exhibit poor knee alignment, can lower the risk of an ACL injury.1,23–25 Collectively, this research has led to the notion that knee abduction is an undesirable movement pattern and should be corrected if observed.3,26
_depiction_of_what_has_traditionally_been_considered_proper_knee_alignment_while_perform.jpeg)
Conversely, there is some evidence illustrating that medial knee collapse may not be a risk factor for knee injuries. Regarding ACL injuries specifically, Cronström and colleagues27 performed a meta-analysis of longitudinal studies that had performed various baseline knee kinematic and/or kinetic assessments during weight-bearing activities; injury metrics were collected from participants at a later date. Contrary to current clinical opinions, no kinematic or kinetic measure accurately predicted future ACL injury.27 However, the authors point out that this may in fact be the result of reduced prevalence of medial knee collapse in today’s young athletic populations. Following the work of Hewett and colleagues,2 in addition to earlier findings on cadaver knees that examined valgus torques on ACL loading,28–30 preventative training measures were rapidly adopted by sporting organizations3,31 and incorporated into clinical guidelines,32 well before a large body of literature on this topic could be properly generated. As a result, most of the studies in this meta-analysis27 reported very low knee abduction angles in their baseline measurements. For example, Hewett and colleagues2 reported peak knee abduction angles as high as 9°, while all subsequent work has been around 2°.33–35 One study even reported that approximately 40% of included study participants had already adopted some form of preventative ACL injury training prior to their involvement in the study.34 Therefore, the results of this meta-analysis27 may not be that medial knee collapse is not correlated with an increased risk of ACL injury, but rather, recent preventative training measures have been largely successful at reducing this risk. It is also worth noting that there is currently no agreed upon consensus on which medial knee collapse magnitudes are acceptable and which are undesirable, making it difficult to know when preventative training measures should and should not be prescribed. For instance, of the limited normative data available, a peak of 2° knee abduction reported in recent studies is well within the typical range seen at initial contact following a vertical drop jump (8.71 ± 9.1°).36
Most importantly for this review, however, is that whether medial knee collapse increases the risk of knee injury or not, many coaches, trainers, clinicians, and rehabilitation specialists continue to screen for and correct this movement pattern whenever it is present. This review will focus on how effective one such corrective method (elastic bands) is at addressing this potential problem.
THE PROPOSED SOLUTION: ELASTIC BANDS ENCOURAGE PROPER KNEE ALIGNMENT
The idea of using elastic bands to correct medial knee collapse is essentially a modern-day form of Reactive Neuromuscular Training (RNT). First proposed by Michael L. Voight in the 90s,37 RNT is a rehabilitation technique that heavily utilizes reactive exercises (exercises that provide the individual with some sort of external cue to respond to while they strive to achieve a simple movement or goal), thus limiting the need for verbal and/or visual instruction from a therapist or trainer.
One way in which RNT is utilized today, and the most important as it relates to this review, is to take an individual who presents with an undesirable movement/posture and exaggerate said movement/posture using external force. For example, if an individual presents with dynamic knee valgus while squatting, it is possible that verbal and/or visual instruction from a trainer or coach may be ineffective at fully changing the movement. However, if an elastic band wrapped around the individual’s distal thighs were to pull them into even further knee valgus, the individual might then be forced into reacting to the larger displacement. If utilized chronically, RNT may change the movement pattern, as has been shown in other applications of RNT.38–42
To the authors’ knowledge, Gooyers and colleagues8 were the first to examine elastic bands wrapped around the distal thighs for the purpose of correcting medial knee collapse. In their paper, the authors suggested that, because lower extremity joint motions are coupled during closed-kinetic-chain activities, medial movement in the frontal plane might represent a deficiency of the hips, and not the knees (insufficient hip abduction and external rotation strength seems to increase knee valgus43,44). More specifically, they8 argue that medial knee collapse might result from an inability to properly activate the external rotators of the hips, causing internal rotation to occur during weight-bearing activities. Elastic bands wrapped around the distal thighs, which function to pull the knees into even further medial movement, might induce movement compensations on the part of the participant. From a mechanistic perspective, Gooyers and colleagues8 suggest that the elastic band may invoke a proprioceptive response in the lower limbs (citing previous case study work using RNT to rehabilitate an ACL rupture38) thereby restoring proper activation of the external rotators of the hip and improving knee alignment. This suggestion seems plausible, given evidence that enhanced tactile stimulation can improve body sway and balance.45,46
THE EVIDENCE: ELASTIC BANDS ON MUSCLE ACTIVITY AND KNEE ALIGNMENT
To the best of the authors’ knowledge, a total of nine original studies have examined the use of elastic bands wrapped around the distal thigh and their effects on either hip external rotator muscle activity, lower limb kinematics, or both while performing squat movements. These studies, along with their key methods and outcomes, are summarized in Table 1. Although many of these investigations have been performed exclusively on barbell back squats,9,12,47,48 the literature as a whole has assessed a considerable range of exercises with elastic bands, including bodyweight squats,7,8,49 overhead barbell squats,11 countermovement jumps,8 squat jumps,8 and drop jumps.50 The intensity at which these exercises were performed at varied widely, from as low as bodyweight to as high as 85% of 1RM. The abovementioned studies were performed on participants who were at least recreationally active, while most were performed on chronically resistance trained individuals; Foley and colleagues48 remain the only researchers to have examined inexperienced participants. Although the literature slightly favors males in terms of recruitment, five of the nine studies were conducted on both male and female participants. The resistance imposed by the elastic bands is perhaps the most inconsistent variable across these studies, and, unfortunately, the units of resistance differ from study to study. For instance, the most common elastic bands utilized in this body of work are those sold by TheraBand®, which communicates resistance based on the strength (in kg) needed to stretch the band to 100% elongation (twice the band’s resting length). Of the studies that have used TheraBand®, resistance at 100% elongation ranged from 1.7 to 6.5 kg. Of the remaining work, most reported the resistance of their bands based on the mostly linear relationship between applied force and band stretch, with resistance ranging from 0.6 to 6.8 N/cm.
Muscle Activity
According to the hypothesis put forward by Gooyers and colleagues,8 an increase in hip external rotator muscle activity should lead to improvements in knee alignment. Of the nine studies summarized in Table 1, all but one8 included measures of muscle activity in their experimental design, and of these eight, all but one11 showed that the use of an elastic band increased muscle activity in at least one lower limb muscle. Although not all studies collected EMG from the same muscles, an increase in gluteus maximus muscle activity was reported by five different studies,7,9,47–49 lending support to the notion that band usage may indeed promote external rotation of the hip (Figure 2). The only studies that did not find an increase in gluteus maximus activity were Dai and colleagues,50 who exclusively examined gluteus medius in their investigation, and the aforementioned work by Forman and colleagues11 and Alizadeh and colleagues.12

Regarding the work by Forman and colleagues,11 the use of an elastic band wrapped around the distal thighs had no effect on muscle activity while squatting for any of the muscles examined, including the gluteus maximus, gluteus medius, plantar flexors, and the knee extensors. This finding can likely be explained by one, or both, of the following reasons: 1) The exercise used in this study was an overhead barbell squat, which is the most technically-challenging movement examined thus far in this body of work. While participants were chronically resistance trained, none had extensive experience performing overhead barbell squats, and thus, the novelty of the movement may have overshadowed the novelty of using an elastic band. 2) It was also reported that band usage significantly decreased peak knee flexion angle, indicating that overall squat range of motion may have been reduced. Since repetition cadence was controlled in this study,11 a squat performed with a shorter range of motion is a squat performed more slowly, which may have reduced muscle activity51–54 and offset any potential increase induced by the use of an elastic band.
The work of Alizadeh and colleagues,12 on the other hand, is perhaps the most inconsistent with comparative literature. In this study, males and females performed barbell back squats either without the use of an elastic band or while using one of three elastic bands of varying resistance. A total of three repetitions were performed for each experimental condition at 85% of 1RM. Although gluteus medius muscle activity did increase with increasing band resistance, gluteus maximus activity was not significantly different between the band conditions. One possibility for this lack of change could be the intensity these squats were performed at; at 85% of 1RM, this is the heaviest workload of all studies in this narrative review. However, this intensity is not substantially higher than those used by similar work. Of the four studies that showed gluteus maximus muscle activity to increase with band usage, three also used barbell back squats, and all three utilized an intensity of ~80% of 1RM in at least some portion of their protocol.
Despite a lack of statistical significance, the results of the work performed by Alizadeh and colleagues12 were trending towards an increase in gluteus maximus muscle activity with increasing band resistance. Considered alongside the other work presented in this narrative review, it is likely that elastic bands do promote increased external rotation of the hip while performing squat movements, which is not particularly surprising. For most studies, participants were repeatedly given verbal instruction to actively resist the external force provided by the elastic band and to keep the band tight throughout the entire exercise/movement. This forces participants to produce an additional external hip rotation moment on top of the exercise they are already performing, and assuming other aspects of the movement are not sacrificed in the process (such as a loss of knee range of motion11), the overall workload of the exercise is increased. This may explain why other lower limb muscles also exhibit greater muscle activity while using an elastic band. Both gluteus medius (shown in five of eight studies)9,12,47–49 and biceps femoris (shown in two of six studies)48,49 muscle activity increased with band usage. Interestingly, three investigations reported a decrease in vastus lateralis muscle activity with band usage during at least one portion of the squat movement,9,12,48 although one study had an increase in vastus lateralis activity,49 and two had a similar decrease in vastus medialis activity.9,12 Considered collectively, this evidence suggests that elastic bands may not just promote external rotation of the hip, but they may also encourage greater utilization of the hip extensors (shown by increases in gluteus maximus, gluteus medius, and biceps femoris muscle activity), and reduce reliance of the knee extensors (shown by decreases in vastus medialis and vastus lateralis muscle activity) while performing squat-based movements. If so, elastic band usage may represent a promising tool for trainers and rehabilitation specialists in targeting hip musculature and/or offloading the knee, depending on the needs of their athletes.
Kinematics
Given the discussed findings that elastic bands likely promote activation of the hip external rotators, intuition would suggest that elastic bands may also reduce medial knee collapse. Current evidence, however, does not seem to support this (Figure 3). Of the nine studies summarized in this review, seven included at least one or more lower limb kinematic measure(s) in their investigation. These measures include knee-width-index (KWI), knee flexion angle, knee abduction (or valgus) angle, hip abduction angle, and hip flexion angle. The most utilized of these measures is KWI, which is a unitless ratio of the net distance between the right and left distal thigh (or lateral epicondyles) divided by the net distance between the right and left distal shank (or lateral malleoli). Written mathematically, this gives:
KWI = Bilateral Distal Thigh Distance / Bilateral Distal Shank Distance
A KWI of 1.0 would indicate that the distance between the knees and the distance between the ankles are approximately equal, which is frequently interpreted as meaning the knees are in-line with the rest of the lower limb and exhibiting no knee valgus. A value of less than 1.0 suggests that the knees are closer together than the ankles, which in turn points to medial movement in the anterior plane (medial knee collapse has occurred). These conclusions, however, may not be accurate. For instance, if an individual is performing a squat with a very wide stance, their feet, and ankles, are already further apart than their knees even before they have descended into a squat. Their knees could very well be properly aligned with the rest of their lower limb, with no knee valgus occurring, but because of their wide stance, their KWI would be less than 1.0. For this reason, the KWI should be viewed as a limited, surrogate measure of knee valgus.
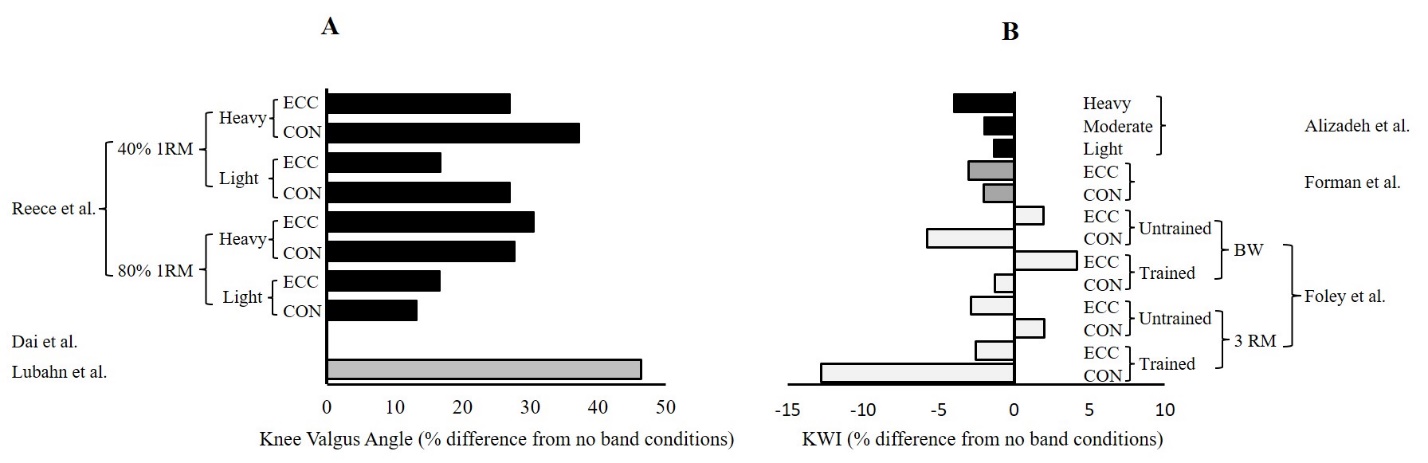
**_knee_valgus_angle_and_**b)**_knee_width_index_(kwi)_while_perfo.jpeg)
With that in mind, the first study to utilize KWI was also the first study to propose the use of elastic bands in correcting medial knee collapse.8 In this study, lower limb kinematics were captured while participants performed one of three exercises: countermovement jumps, bodyweight squats, and squat jumps. All exercises were performed without a band or with a light (1.5 N/cm) or medium (2.0 N/cm) tension elastic band. Although band usage had no effect on KWI during squat jumps, KWI significantly decreased for both countermovement jumps and bodyweight squats while using elastic bands. Similar findings have been reproduced during overhead barbell squats,11 whereby peak and mean KWI decreased with band usage in both the eccentric and concentric phases, and during barbell back squats.12 The only other study which has utilized this measure found no differences in KWI when performing barbell back squats with or without an elastic band.48 Beyond KWI, knee valgus angles have also been directly quantified in participants performing bodyweight squats, drop jumps, and barbell back squats. While no change in knee valgus angle was observed when performing drop jumps with or without an elastic band,50 band usage significantly increased knee valgus angle during bodyweight squats7 and barbell back squats.9
Considered collectively, these findings suggest that the use of an elastic band while performing squat-based movements does not acutely reduce knee valgus. In fact, it either has no effect,48,50 or it may actually increase knee valgus.7–9,11,12 This may seem at odds with the previously discussed increases in gluteal muscle activity, which should have led to an increase in hip external rotation. What may be happening is that, while elastic bands do successfully promote activation of the hip external rotators, the ensuing increase in external rotation torque is either equal to or less than the external force provided by the bands themselves, resulting in either no change in knee alignment or an increase in knee valgus.
On a surface level, an elastic band-induced increase in knee valgus may seem like a problem. In fact, some researchers have interpreted this finding as a clear warning that elastic band usage may increase injury risk during squat-based activities and have recommended trainers and clinicians to immediately remove them from training programs.9,10 In reality, though, the risk is likely minimal. While five studies have shown knee valgus to increase with band usage (or assumed an increase based on KWI interpretations), these increases have all been very small and may not be clinically significant. For instance, when squatting with an elastic band, knee valgus angle increased from 4.1° to 6.2°7 and from to 3.01° to 3.92°.9 KWI has also been shown to decrease by ~0.02,11 ~0.038,8 and ~4%,12 all while using the strongest bands utilized in these studies. Again, there is currently no agreed upon consensus on which medial knee collapse magnitudes, if any, represent an increased injury risk, and of the available normative data, the knee valgus angles shown by both Lubahn and colleagues7 and Reece and colleagues,9 both with and without a band, are well within these ranges.36 Based on these findings, it is unlikely the small increases in knee valgus due to elastic bands will increase the risk of lower limb injury.
While most of the present literature has exclusively focused on quantifying medial knee collapse, a few investigations have examined other kinematic measures that are likely important to consider. For example, maximum knee flexion angle11,50 and maximum hip flexion angle50 have been shown to decrease while using an elastic band. Although Alizadeh et al.12 observed no change in peak knee flexion angle in their own study, these collective findings suggest that elastic bands might reduce range of motion when used. However, band usage may not be directly responsible for this reduction. Rather, the process of adapting to the novel use of an elastic band (none of the above studies collected from participants with previous band experience) may have resulted in a decreased range of motion. This explanation is currently speculative but should be considered in future investigations seeking to examine chronic elastic band usage.
Importance of Band Resistance Dosage
If elastic bands are to be prescribed for the sake of correcting medial knee collapse, then the resistance of the band chosen is likely of major importance. This is primarily because greater band resistance may increase knee valgus. On the other hand, elastic bands of even light resistance seem capable of increasing lower limb muscle activity. To elaborate, in the work by Gooyers and colleagues,8 while the light resistance elastic band of 1.5 N/cm did decrease KWI at various portions of countermovement jumps, reductions in KWI occurred more frequently with the medium resistance band of 2.0 N/cm. Similar findings have been noted between studies utilizing elastic bands of only one resistance level. Using one of the lightest bands offered by Theraband®, specifically 1.7 kg of resistance at 100% elongation, muscle activity from multiple muscles of the lower limb increased, all while KWI remained unchanged between conditions.48 In contrast, the strongest band of 6.5 kg has been shown to decrease KWI, with no subsequent changes in lower limb muscle activity.11
Given these findings, some of the most recent literature on this topic has made a point of specifically focusing on elastic band resistance in their investigations, and the findings across these studies have been largely consistent. In the muscles that demonstrated an effect of elastic band usage, the relationship between muscle activity and elastic band resistance was almost linear, with muscle activity highest while performing squats with the strongest elastic bands.9,12,49 Similarly, medial knee collapse (measured indirectly with KWI12 and directly with knee valgus joint angles9) increased with increasing band resistance. Thus, while stronger bands likely yield greater levels of lower limb muscle activity, which may be beneficial in training the external rotators of the hip for squat-based movements, they also result in greater medial knee collapse. Perhaps the obvious application of these findings is that trainees should simply use the lightest elastic band possible if attempting to reduce knee valgus. This will be discussed at greater length in the following sections.
CURRENT RESEARCH GAPS AND LIMITATIONS
The primary reason for conducting this review was to help provide context on a topic that is relatively poorly studied and one with sometimes contradictory findings. For those in the fitness world, it is often unclear why or for what purpose athletes are using elastic bands while performing squat-based movements, while in the academic world, there are some research circles that strongly recommend against the use of these bands over injury risk concerns.9,10 However, even now, neither the benefits nor the risks of elastic band usage are well understood. Not only is the topic limited by a small number of studies (only nine), there are also limitations in the research.
Participant Screening for Medial Knee Collapse
To date, no studies have first pre-screened their participants for medial knee collapse. To illustrate this problem, Forman and colleagues11 reported KWI group averages of approximately 0.99 and 1.0 in the concentric and eccentric phases, respectively, while squatting without an elastic band. This may indicate that knee alignment was already close to perfect at study onset, meaning that it is impossible to conclude that elastic band usage is ineffective at reducing medial knee collapse, given that medial knee collapse was not likely present to begin with.
Chronic Elastic Band Usage
It is crucial to understand that elastic band usage throughout this literature has only been examined acutely (single session studies). Thus, even if participants throughout the literature had presented with medial knee collapse at study onset (which they likely did not, as per the previous paragraph), the possible effects of elastic band usage were only quantified within a single acute session. To properly assess the validity of this potentially corrective training aid, elastic bands and their effect on medial knee collapse should be examined after chronic elastic band usage.
RNT Exaggerates Movement Errors
Researchers pursuing this topic should be reminded that the very nature of RNT is not to have trainees performing the exercise correctly while the external force is being applied (which should be exaggerating the undesirable movement pattern), but to see improvements in their technique after the external force has been removed.37 The findings that elastic bands increase knee valgus8–10,12,13 may actually be a promising outcome from the perspective of RNT as it means elastic bands are capable of exaggerating medial knee collapse.
Influence of Sex on Band Usage
Although research has demonstrated that females tend to exhibit greater knee valgus than males,3,55–57 the possibility that elastic band usage may influence either hip external rotator muscle activity, knee alignment, or both uniquely based on sex has been infrequently explored in current literature. For effective prescription, it is vitally important for future research to account for sex differences in their study design and statistical analyses.
FUTURE RESEARCH DIRECTIONS
If understanding of both the benefits and the risks of elastic band usage during squat-based movements (specifically for the purpose of correcting medial knee collapse) is to be improved, it is essential for future research to address the aforementioned limitations. First, studies should shift focus away from individuals with extensive training experience, or those with adequate knee alignment, and instead intervene with individuals who exhibit clear signs of medial knee collapse. Only by assessing this demographic can researchers make stronger conclusions regarding the effectiveness, or lack thereof, of elastic bands as corrective aids. Second, for those who do present with medial knee collapse, it is unlikely that a single session of elastic band usage will lead to noticeable improvements. It is even less likely that a single session will fully correct the problem. For elastic band usage to be fairly assessed, researchers should consider longitudinal investigations, where participants presenting with medial knee collapse utilize elastic bands chronically over multiple sessions and weeks. Such investigations would more accurately reflect both how elastic bands are applied in practice and the length of time it might take for the technique error to improve. Lastly, if elastic bands are to be an effective RNT aid, researchers may anticipate a temporary worsening of knee valgus during elastic band usage which subsides once the bands are removed. The success or failure of elastic bands should also be assessed not during their direct usage, but while participants perform squat-based movement free of elastic bands after a prolonged period of chronic elastic band training.
RECOMMENDATIONS AND CONCLUSION
Of the evidence that is presently available, elastic band usage while performing squat-based movements appears capable of enhancing hip external rotator muscle activity, which may be of benefit to individuals who exhibit medial knee collapse as a result of insufficient hip external rotation. Over time, chronic elastic band usage could potentially strengthen this musculature and/or lead to permanent neuromuscular adaptations, which would result in improved knee alignment. This, however, is currently speculative; no longitudinal studies, focused primarily on individuals who clearly demonstrate medial knee collapse, have yet to be conducted. It is also clear that the use of elastic bands does not acutely reduce knee valgus. They either have no effect, in the case of low resistance elastic bands, or increase knee valgus, in the case of high resistance bands.
For coaches, trainers, and rehabilitation specialists considering the use of this technique either for athlete training or patient treatment, the substantial limitations present throughout the current literature make best practice recommendations difficult. If an individual chooses to use this technique, they may wish to utilize a lighter resistance elastic band. Even light elastic bands have shown the capacity to enhance hip external rotation muscle activity, and the chances of inducing a potentially undesirable increase in medial knee collapse are reduced. Even if utilizing light elastic bands, careful monitoring of a trainee’s knee alignment throughout the entire squat-based movement is indicated, and if a noticeable increase in knee valgus is observed, switch to a lighter band. Only by addressing the gaps that exist in current research can more confident conclusions be offered about the benefits and risks of using elastic bands to correct medial knee collapse during squat-based movements.
Conflicts of Interest
The authors report there are no competing interests to declare
Disclosure of Funding
No funding sources were utilized in the preparation of this manuscript.