
INTRODUCTION
Range of motion (ROM) assessments are commonly performed by healthcare professionals including physical therapists, occupational therapists, chiropractors, physicians, and other medical professionals when the focus of rehabilitation is related to the musculoskeletal and neuromuscular systems. Range of motion measurements assist healthcare professionals in monitoring progress during the rehabilitation process.1 These assessments are also important for establishing baselines, functional limitations, or dysfunction in ROM due to injury or disease. They are also often used in sports performance evaluations for athletes who want to increase strength and joint mobility, regardless of injury status.2 Prior authors have reported that adequate ROM is fundamental to perform functional activities of daily living and meet vocational demands.3–5 Thus, it is important for healthcare providers to assess and reassess ROM during the physical rehabilitation process to ensure sufficient progress towards return to function.
Physical therapists and other healthcare professionals use various methodologies and tools to assess ROM. Some healthcare professionals utilize standardized objective tools such as a goniometer, inclinometer, or a smartphone while other healthcare professionals implement more subjective techniques such as a visual estimation or by observing functional movement patterns.1,6–8 The goniometer is a gold standard tool commonly used by healthcare professionals to assess joint ROM, and also is a primary instrument used in higher education to teach future healthcare professionals how to assess joint ROM. Goniometry has been used widely due to its portability and low cost.9,10 However, a limitation of goniometry is that it requires the clinician to use both hands, making stabilization of the extremity difficult, and thus increasing the risk of error in reading the instrument.9
In recent years, digital tools ranging from electrogoniometers with simple flex sensors, to more complex machine learning-based systems are becoming more widely utilized in clinical practice. Motion capture systems are a subset of these digital tools that have shown great promise for accurate and timely measurements in the domain of human movement analysis, including ROM assessment.11–15 Two-dimensional (2D) motion capture systems such as smartphones utilize readily accessible technology but are limited in their ability to assess ROM, when a picture or video is captured it does not account for depth and the perceived angles of the objects, thus the frame is largely dependent on the perspective of the lens.16 This is referred to as parallax error. Therefore, if a person is not positioned precisely in front of the camera their joint angle measurements may be skewed.
Three-dimensional (3D) motion capture systems that implement Light Detection and Ranging (LiDAR) technology use light emitted from a pulsed laser to measure distance. LiDAR and other depth sensing technology afford clinicians high fidelity data models and more accurate spatiotemporal representations of body movements, which result in greater reliability and validity of ROM assessments when compared to 2D motion capture tools.17 Unfortunately, many 3D motion analysis systems are complex to set up, require multiple cameras, are costly, and not portable, making them inaccessible to healthcare providers.18
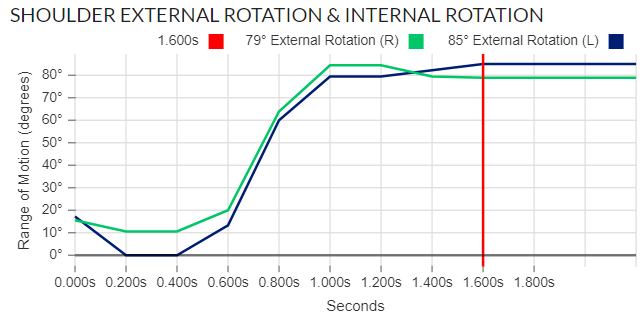
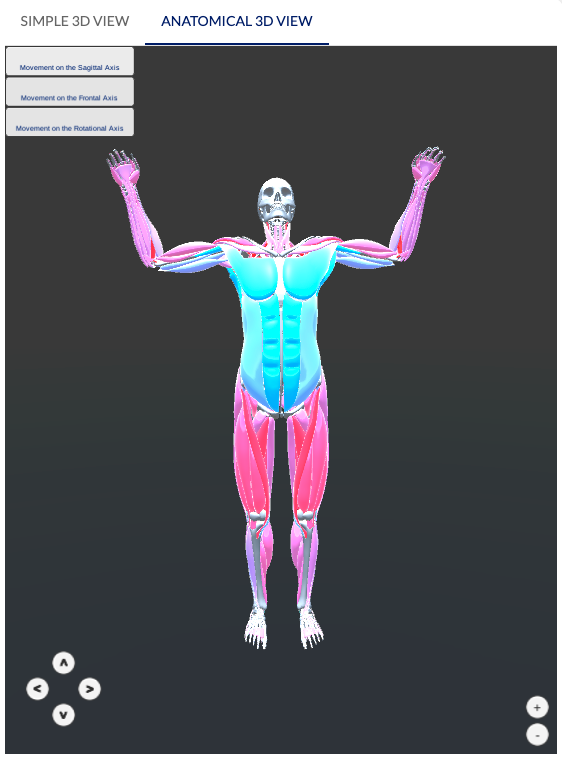
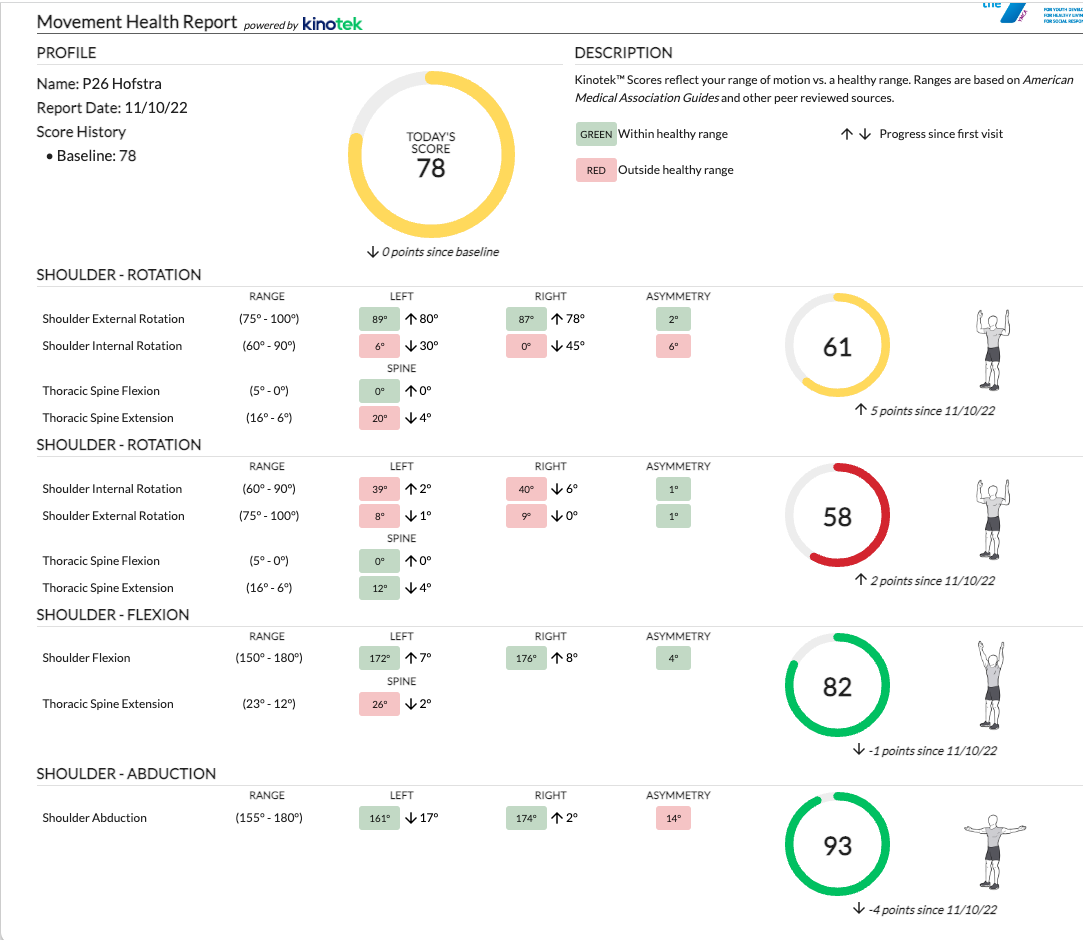
With recent advancements in technology, new digital tools have been introduced that assist medical, sport, and fitness professionals in performing examinations and screenings. One recent advancement introduced was a 3D motion capture system that uses a single camera, is markerless, and portable (Kinotek, Inc., Portland ME). This system was designed to obtain ROM measurements for multiple body parts simultaneously. The system is capable of measuring 64 distinct movements and 750 data points per visual analysis using 30fps.19 For each analysis, the software outputs objective data on ROM, asymmetries present between right and left, and a quality movement graph that provides metric analysis for motion tracking for the entirety of the movement (Figure 1A-C). The software provides pre- and post-movement comparisons, progress charts, and other data that can be easily translated to written documentation. In addition, this system generates an avatar of the individual for 3D visuals which can rotate 360° enabling the user to focus on specific areas during motion tracking for optimal visualization. This system uses Microsoft’s Azure Kinect camera, which is commercially available, and relatively inexpensive compared to other 3D motion capture systems on the market. The setup is simple and can be completed by a single user without assistance. The system is portable, cost effective, and works via a WiFi connection to any compatible device, such as a laptop. However, the reliability and validity of a markerless 3D motion capture system that uses a single camera has not been established. The purpose of this study was to investigate the reliability and concurrent validity of a markerless, single camera, portable 3D motion capture system compared to goniometer in assessing ROM of the glenohumeral joint.
MATERIALS AND METHODS
Participants
Healthy individuals were recruited on a voluntary basis by distribution of flyers at a local university. Participants were eligible to participate in the study if they were at least 18 years of age, had the ability to perform movements bilaterally, and had the ability to demonstrate the specified movements without loss of balance. Participants were excluded from this study if they were taking any medications that impair balance or ability to think, had any recent injuries that are still being treated by a healthcare provider, if they had active pain or tingling/numbness during the time of data collection, or were not able to provide consent.
Ethical Approval
Ethical approval for this study was granted by Hofstra University Institutional Review Board. Prior to data collection, participants reviewed and signed an informed consent.
Instruments
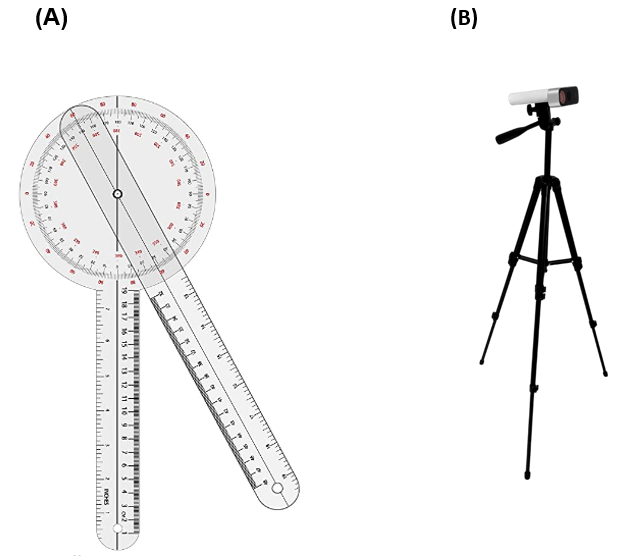
The instruments utilized for data collection are represented in Figure 2 (A-B), which included one (A) Full-circle standard 12-inch plastic goniometer and (B) 3D motion capture system (Kinotek Inc., Portland ME). The goniometer is as a commonly used tool by healthcare providers for assessing joint ROM and identifying body asymmetries, and previous studies reported this tool to be a reliable and valid option for measuring ROM in various joints of the body.3,12,20–24 Thus, for data collection the goniometer was used in this study to compare measurements between the 3D motion capture system and a standard tool commonly utilized by healthcare professionals.
_full-circle_standard_12-inch_plastic_goniometer__b)_3d_motion_capture_system_(kinotek_.png)
Tester Selection and Procedure
The tester selected for this study was a licensed physical therapist with 15 years of clinical experience that commonly uses a goniometer in clinical practice. In addition, the tester had experience as an educator in a class that taught goniometry to physical therapy students. To assess the reliability of the tester, five repeated goniometric measures were taken by the tester and statistically analyzed for intrarater reliability. For data collection, the same tester took all measurements with the goniometer. The tester was blinded to the displayed readings while positioning the goniometer on the participant and a second person recorded the readings. For this study, active ROM of the glenohumeral joint was measured (abduction, flexion, external rotation, internal rotation). Each of the movements were performed with the participant positioned in a standing position and seven feet from the camera, as demonstrated in Figure 3. The room was set up with the floor marked at seven feet from the center of the camera, forward facing towards the camera. The camera was positioned with a 6º tilt upwards at a height aligned to the mid-pelvic region. Each participant was given a verbal cue to start active ROM for each of the shoulder movements while the camera was recording, and instructed to stop at the end of the available range and hold the position while the testers recorded the goniometric measurement. Verbal instructions were standardized so that all participants received the same verbal cueing. Prior to each movement, participants were shown a visual demonstration of the movement and were also instructed on potential body substitutions with each movement. Then, one practice trial was performed. After the trial, the tester provided feedback to the participant to mitigate any further extraneous variables that were identified pertaining to the movement such as body substitutions and speed of movement. Two additional trials for each movement were then recorded that were used for data analysis, following the procedure described above.

Statistical Analysis
Data were analyzed using SPSS Statistics v28 (Armonk, NY). Intrarater reliability was determined using the Intraclass Correlation Coefficient (2,k) with a 95% Confidence Interval. Descriptive statistical analysis was also performed to analyze the demographic information collected from the sample of participants. Concurrent validity was determined using the Pearson Correlation Coefficient (r) by comparison of the averaged readings from the two trials using both instruments.
RESULTS
The total sample size of participants meeting inclusion criteria was 40; 29 who identified as female and 11 who identified as male. The average age for participants was 27.4 ± 12.4 years with age ranging from 18 to 62 years old. The average height and weight for participants was 173.4 ± 11.1 cm and 72.1 ± 16.2 kg, with a range of 152.4 to 193.0 cm and 47.2 to 116.6 kg respectively. A total of 80 shoulders were measured.
Measured Values
The mean and Standard Deviation for each shoulder movement recorded by both instruments is reported in Table 1.
Reliability
The intrarater reliability between the Goniometer and 3D motion capture system for shoulder abduction, flexion, external rotation, and internal rotation is reported in Table 2 with ICC(2,k) values and a 95% CI along with the Standard Error of Measurement (SEM). The analysis yielded an overall ICC of 0.82 (0.74 - 0.88) indicating good reliability for both instruments.
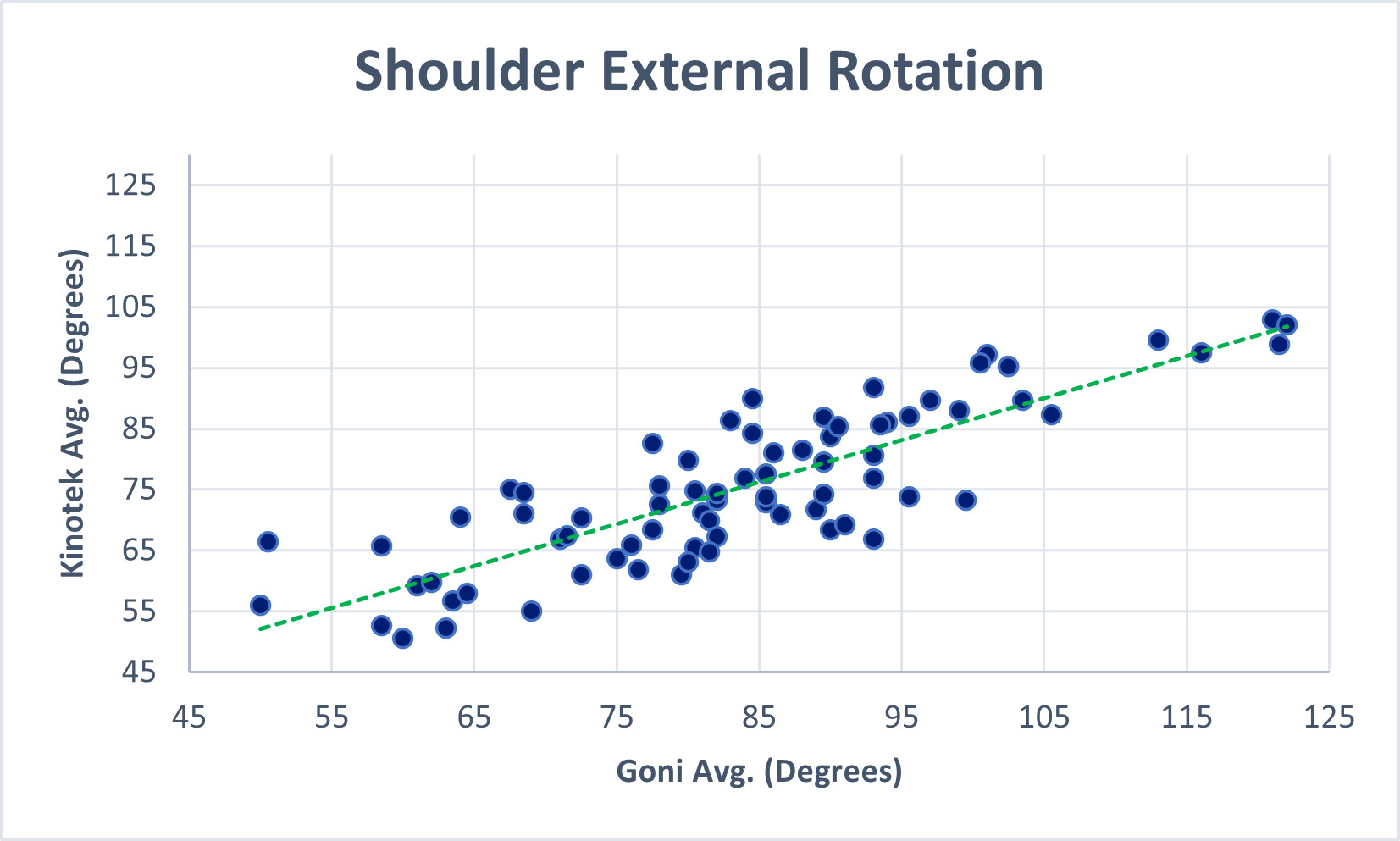
Validity
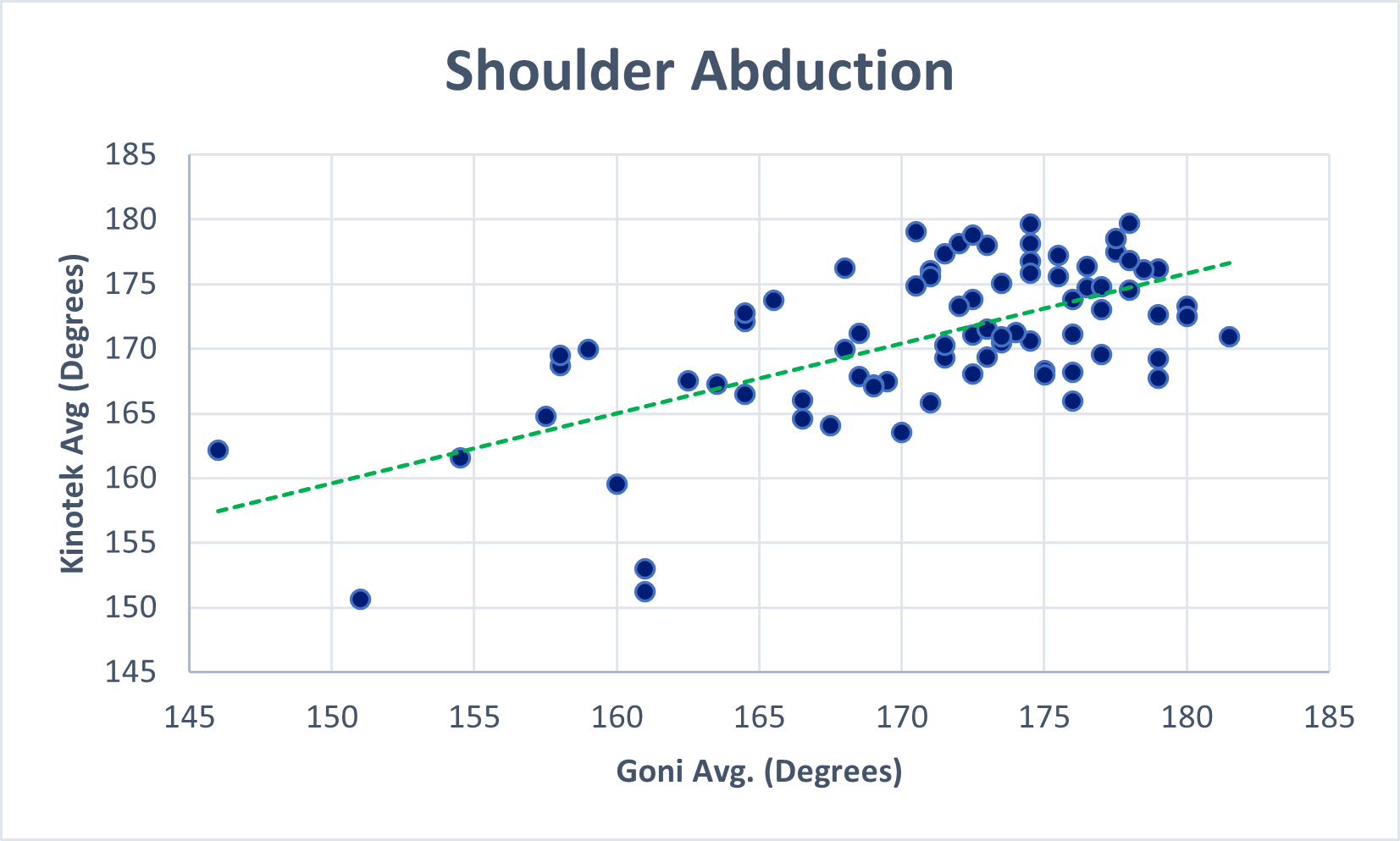
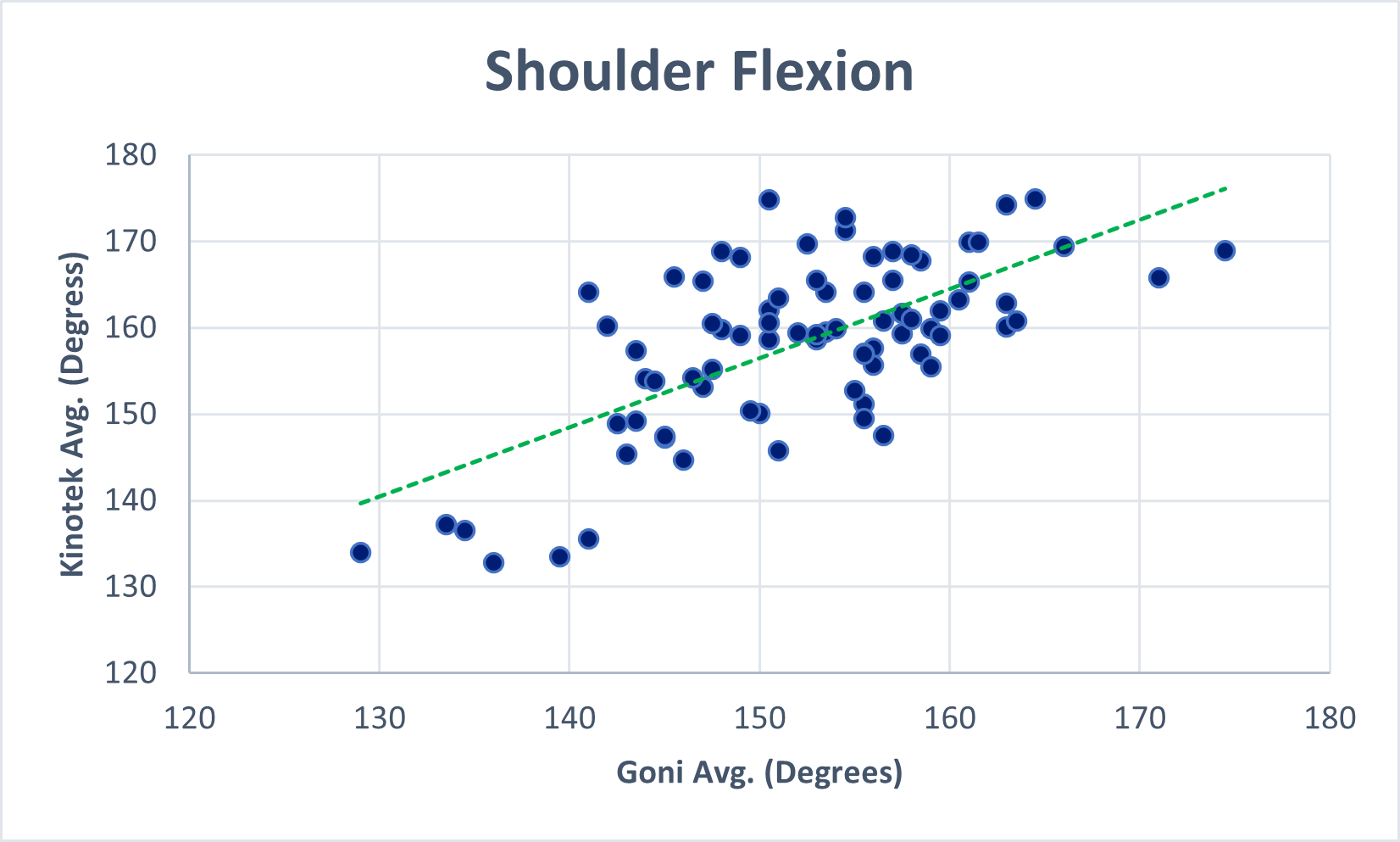
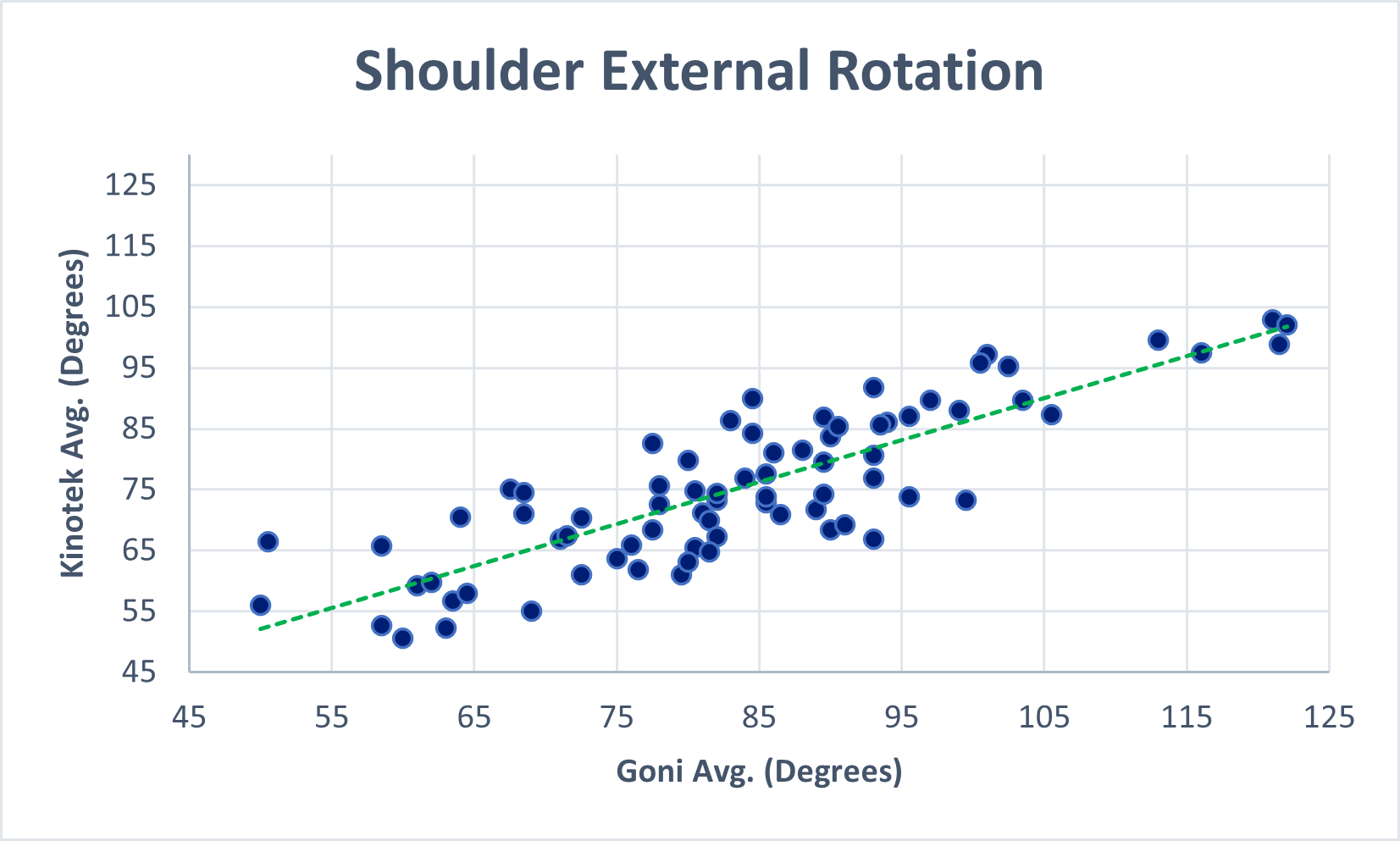
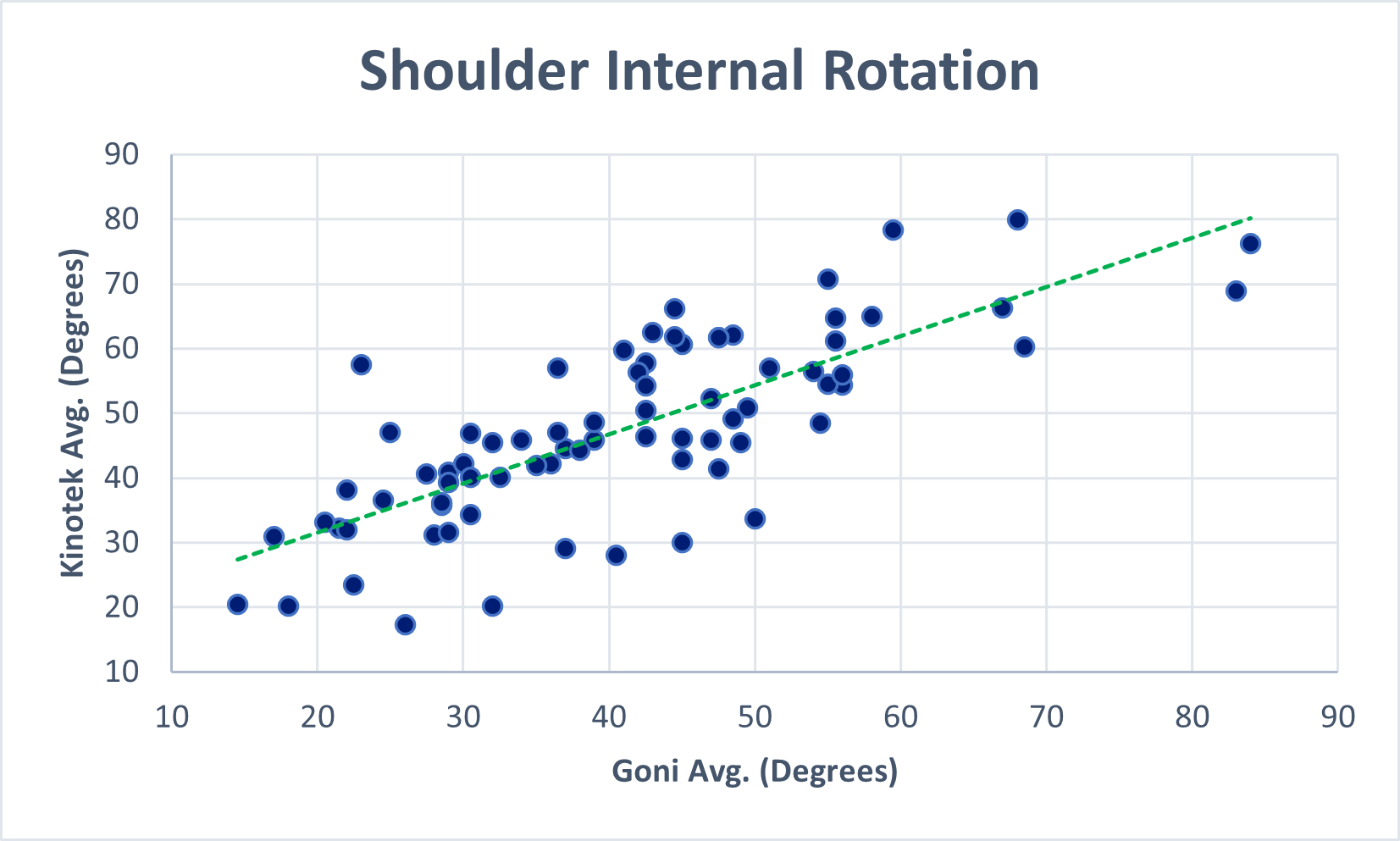
The Pearson Correlation Coefficient (r) was analyzed to establish concurrent validity. Figure 4 (A-D) illustrates the relationships between the goniometer and 3D motion capture system for glenohumeral abduction (r = 0.63, p <0 .001), flexion (r = 0.67, p < 0.001.), external rotation (r = 0.76, p <0 .001), and internal rotation (r = 0.84, p < 0.001)



DISCUSSION
The purpose of this study was to investigate the reliability and concurrent validity of a markerless, single camera, portable 3D motion capture system compared to a goniometer in assessing active ROM of the glenohumeral joint. While other studies have investigated the reliability and validity of multi-camera 3D motion capture systems, the reliability and validity of a markerless 3D motion capture system that uses a single camera has not been established.
Reliability and validity are important to establish for tools and technologies, especially when being used by healthcare or sports professionals. Portney and Watkins25(p77) describe that “usefulness of a measurement and decision-making depends on the extent of its reliability and validity, where reliability refers to the extent of consistency in repeated measures and validity refers to the extent of accuracy or if the tool is measuring what it is intended to measure”. They conclude that reliability and validity are fundamental to all aspects of a measurement, because without it one cannot have confidence in the data collected nor draw sound conclusions from those data. The current study found, for concurrent validity measurements with the 3D motion capture system were comparable to those taken with the standard 12-inch plastic goniometer with correlation values ranging from 0.63 - 0.84 indicating high to very high correlation between the instruments, where 0 < r ≤ 0.19 = very low correlation, 0.2 ≤ r ≤ 0.39 = low correlation, 0.4 ≤ r ≤ 0.59 = moderate correlation, 0.6 ≤ r ≤ 0.79 = high correlation, and 0.80 ≤ r ≤ 1.0 = very high correlation.26,27 The measurements obtained using both instruments yielded intrarater reliability in the range of ‘good’ overall.28 These results are comparable to previous research that reported good intrarater reliability when utilizing similar measurement procedures.11–14,29 Macedo and Magee28 reported on passive ROM of peripheral joints, which included the shoulder joint, on healthy adult females. They reported the SEM for the goniometer to be 3.5º while the Minimal Detectable Change (MDC) at a 95% CI ranged from 4º to 21º with a mean of 9.6º. Results from the current study reported results consistent with those previously reported.
Range of motion assessments are important for evaluating the effectiveness of treatment over time, establishing baselines, limitations, or dysfunction in ROM due to injury or disease, and monitoring progress during the rehabilitation process.1,30,31 Advancements in technology have introduction new digital tools that assist medical, sport, and fitness professionals in performing examinations and screenings. Results from this study demonstrated a strong positive correlation between Kinotek and the goniometer. There are several benefits of incorporating 3D motion analysis for ROM assessment. First, 3D motion capture provides motion tracking throughout the entirety of the active ROM, which allows greater insight to the quality of the movement while also allotting the operator to stop the movement at any point during the movement. Another benefit is that this 3D motion capture software generates an avatar of the individual being recorded. The avatar can be rotated and viewed in the frontal, sagittal, and transverse plane allowing the operator to view the individual’s movement at any angle (Figure 1B). However, a standard goniometer costs significantly less than a 3D motion capture system, has greater portability, and is still widely utilized by postsecondary institutions to teach joint ROM assessment.
This research study had limitations in that the data collected were on healthy individuals. It would be advantageous in future studies to consider a sample with mobility impairments or conditions or of different populations such as those with musculoskeletal and neuromuscular disorders, as active ROM of the glenohumeral joint in healthy individuals may not correlate with those who have shoulder pathology. A power analysis was conducted prior to data collection to determine the approximate sample size needed to produce a meaningful effect size, and although 40 participants (80 shoulders) met these criteria, a larger sample size would also be beneficial in future studies to further strengthen the generalizability of any conclusions. While this study found promising results for reliability and validity of glenohumeral active ROM, it is recommended that future studies investigate other joints using this 3D motion capture system to investigate the reliability and validity of this newer technology. Despite these limitations, this study provides a promising future for physical therapists and other healthcare professionals who focus on rehabilitation and sports performance evaluations, as the 3D motion capture system can be a reliable and valid alternative to the goniometer in assessing joint ROM.
CONCLUSIONS
This study found acceptable reliability and validity of the 3D motion capture system in comparison to standard goniometric measurments when assessing glenohumeral joint active ROM. Three-dimension motion capture systems are valuable in rehabilitation related to the musculoskeletal and neuromuscular systems. However, they have not been widely used by healthcare and sports professionals due to its limited portability, large size, use of multiple cameras, high cost, and complexity of operation. A 3D motion capture system that is portable, markerless, and uses a single camera can offer physical therapists and other healthcare professionals alternate time efficient methods to assess mobility of multiple joints simultaneously and provide objective time series data of movement patterns.
Conflict of Interests
Ofra Pottorf is an Independent Consultant and Advisor for Kinotek, Inc.
Kaitlyn Haase is an employee of Kinotek, Inc.