
INTRODUCTION
Dry needling is a common technique used by physical therapists to treat musculoskeletal pain,1 and needling the muscles around the lumbar spine has been shown to decrease low back pain in patients post-intervention.2–4 Significant and serious adverse events with dry needling have been published5–7; however, they are likely underreported.8 Documented adverse events from needling interventions in areas around the spine include: acute epidural hematoma,5,6,9 post-dural puncture headache,10,11 infection,12,13 lower extremity weakness,14 and numbness into an extremity.14 Other documented adverse events include bleeding, bruising, pain, aggravation of symptoms, nausea, feeling faint, and headaches.14 Currently, no national or international system is available for tracking data on adverse events related to dry needling.15 While significant and serious events from dry needling are not common, therapists should be aware of all potential risks to improve procedures, safety for the individual patients, and the overall standard of practice.
One potential factor that may contribute to the occurrence of adverse events with dry needling is the lack of a universally accepted intervention methodology. Multiple approaches are used in research and instruction of dry needling techniques, which leads to variability in practice and difficulty determining if adverse events are tied to a specific approach.8,16–18 For example, there are a variety of methods described to dry needle the lumbar multifidi, which include variations in both the location of needle placement as well as the angulation of the needle as it is directed toward the targeted tissue.
When targeting the lumbar multifidi, Rainey describes a needle placement within one finger breadth lateral to the spinous process and a needle direction that is just medial to the vertical axis.19 Wang-Price et al. used a needle placement 2.0 cm lateral to the spinous process and angled 20° medially toward the spinous process, as well as a needle placement 4.0 cm lateral to the spinous process with a 45° medial angulation, with both techniques resulting in successful placement of the needle in the lumbar multifidi confirmed on ultrasound imaging.20
Other authors report an inferomedial needle angulation when targeting the lumbar multifidi but are not consistent with all parameters. Variations in parameters include needle placements at 1.0 cm lateral to the spinous process with a 15° inferomedial angulation21 as well as 1.0 cm, or 1 finger breadth lateral placement with an inferomedial angulation without specific information related to the degree of angulation, thereby leaving the technique open to interpretation.18,22 Hannah et al. describe a 1.5 cm needle placement lateral to the spinous process with a 45° inferior and 45° medial angulation of the needle.23 In addition to the medial and inferomedial needle angulation techniques, other techniques include placing the needle 1.0-1.5 cm lateral to the spinous process with no angulation, but rather a straight posterior to anterior direction.23,24 Table 1 outlines the variability that exists related to needle position, needle length, needle angulation, depth of penetration, and patient position for dry needling the lumbar multifidus.
Despite the variability that exists in needling technique, dry needling of the multifidi has been considered a safe technique due to the ability of the vertebral lamina to serve as a protective barrier for the spinal canal, preventing inadvertent needling into the spinal canal. Several studies have examined the accuracy of needle placement in the lumbar multifidi at L4-518,21 and the safety considerations related to nearby structures, such as the kidneys and lungs,24 but none have investigated the possibility of entering the spinal canal in the upper lumbar region. Spinal canal perforation is a risk and has been demonstrated in the upper cervical spine.27 Additionally, acute cervical epidural hematoma has occurred following dry needling5,6 and may occur in other areas as well. The cadaveric dry needling technique described in this commentary highlights one of the multiple, documented approaches for the lumbar multifidi and sought to determine if a significant safety vulnerability exists.
The idea for this collaboration between physical therapy and certified registered nurse anesthetist (CRNA) faculty originated during a discussion on the distinctions between lumbar punctures performed by anesthesia providers and dry needling techniques executed by physical therapists on the multifidi. While the classic approaches and needle types for these two procedures differ, it raises the question of whether a dry needling procedure, when conducted in a manner described as safe and effective, can potentially breach the spinal canal.19,20 Table 2 compares a lumbar puncture technique and dry needling techniques targeting the lumbar multifidi.
The purpose of this collaborative cadaveric ultrasound-guided examination of dry needling was to determine if a dry needle can penetrate the ligamentum flavum at T12/L1 interspace and enter the spinal canal using a paramedian approach in a fresh-frozen, lightly fixed cadaver in the prone position.
METHODS
The procedure was performed at Middle Tennessee School of Anesthesia on an 88 y/o female donor by a certified registered nurse anesthetist with over 20 years of diagnostic ultrasound imaging experience and 15 years performing and teaching regional anesthesia. The fresh/lightly embalmed donor was received via the Willed Body Program at The University of North Texas Health Science Center. Exemption from Institutional Review Board approval was granted by Advarra IRB (Pro00070509).
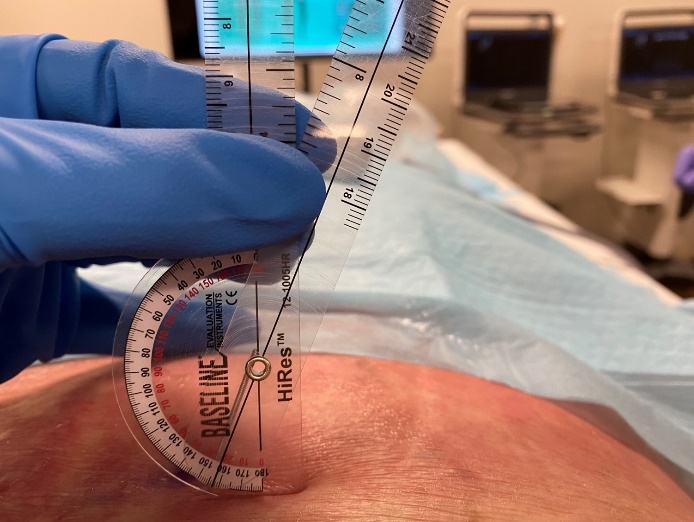
The cadaver was placed in a prone position. A Sonosite Edge II ultrasound system with an rC60xi 5-2 MHz curvilinear array transducer (Bothell, WA) was placed in a parasagittal orientation with the orientation indicator facing cephalad. The sacrum, L5-S1 interspace, and L5 spinous process were identified. The transducer was slid cephalad until the interspace between T12 and L1 was identified. An AGUPUNT APS 0.30 x 50 mm dry needle was inserted approximately 1.0 cm lateral to the spinous process of T12 (Figure 1) and was directed medially at a 22-degree angle (Figure 2). The needle was advanced under ultrasound guidance to determine if it could penetrate the ligamentum flavum to enter the spinal canal.


RESULTS
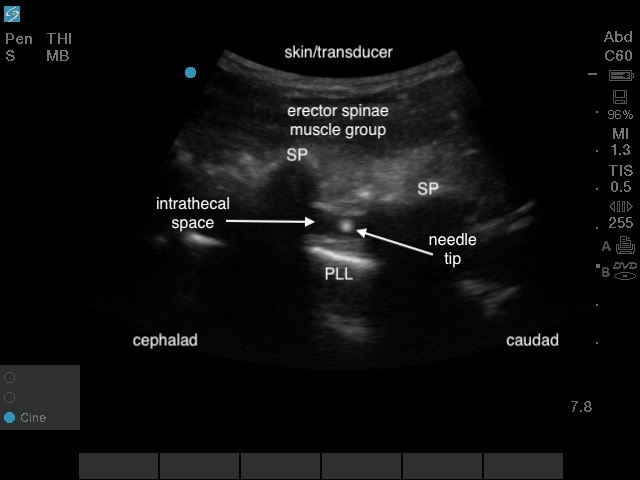
As Figure 3 and Figure 4 illustrate, a 0.30 x 50 mm dry needle inserted approximately 1.0 cm lateral to the spinous process of T12 and directed medially at a 22-degree angle can pass between adjacent vertebral laminae and penetrate the ligamentum flavum to enter the spinal canal. Please reference Supplemental File 1 for video evidence.

CONCLUSION
While adverse effects resulting from entering the spinal canal during a dry needling procedure are rare, this interprofessional collaboration demonstrates some important considerations for the clinician when performing dry needling. First, there is significant variability in the techniques described for dry needling the multifidus with no clear consensus regarding which technique is most effective and safe. Many techniques described also lack specific information regarding needle angulation, thereby leaving the exact technique open to interpretation, and this ambiguity has the potential to lead to variations in clinician needling technique and a resulting decrease in the certainty of a safe needle path and placement. This cadaveric study demonstrates that a 0.30 x 50 mm dry needle is able to penetrate the ligamentum flavum and enter the spinal canal at T12/L1 using a dry needling technique described for the multifidus, and therefore, either purposeful or inadvertent deviations in needle placement in this area of the spine have the potential to cause neurologic injury. While a comprehensive understanding of human anatomy is crucial for dry needling, the utilization of ultrasound has the potential to enhance the precision of dry needling techniques in vulnerable areas, such as the thoracolumbar junction, and may contribute to further risk reduction. The authors recommend that future studies explore various needle lengths and positions, as well as other regions of the spine and patient positions to explore the risk of a dry needle entering the spinal canal under these conditions.
Conflicts of interest
The authors declare no conflicts of interest.