INTRODUCTION
Though core stability may be an important risk factor to address in females, it is inherently difficult to measure: no standardized definition of core stability currently exists, therefore no standard measurement exists. Examples of core stability measures include isometric strength tests of the trunk and hip,1,2 trunk endurance holds,3 and planking or bridging activity.4 Due to the variability in definitions, it may be more economical to utilize a measurement that captures all of these factors simultaneously.
The Trunk Stability Push Up (TSPU) is a component of the Functional Movement Screen (FMSTM). The FMSTM is a battery of seven fundamental movement patterns designed to quickly screen for quality and symmetry of movement. In a recent meta-analysis, composite scores on the FMSTM have been shown to have an association with future injury risk, and poor performance on any individual component, including the TSPU, has been shown to increase risk for future injury.5,6 The association between FMSTM performance and injury may also be impacted by sex as demonstrated by Moore et al., with a larger effect observed for females.7 To perform the TSPU competently (i.e. scoring a 2 or higher), adequate muscle activation of the upper extremities, trunk, and hip/pelvis is required. Thus, the TSPU may be a functional, field-expedient alternative to comprehensively capture the construct of core stability.
It is well-established in the literature that females perform worse on the TSPU than their male counterparts. In adolescents, a significant difference (p<0.000) in TSPU performance was noted by Abraham et al.8 Lower scores in adolescents on the TSPU have been noted in female hockey players (1.20 +/-.45) and non-active females (1.18 +/- .40).9 Anderson et al reported a 69% failure rate on the TSPU in high school females, compared to only 13% in males.10 This gender difference has been observed in collegiate athletes as well, with females scoring significantly lower than males (p<0.001).11 The gender difference persists into adulthood, with more than 60% of active females failing the TSPU compared to less than 10% of active males.12 Currently, the highest pass rate for females on the TSPU in empirical evidence is 42% without previous intervention, with 45 of 108 active, healthy females scoring a 2 or 3 in a cross-sectional study.12 Additionally, a low number of females are included in corrective programs focusing on improving fundamental movements like the TSPU, further contributing to a lack of improvement. The highest proportion of female subjects in a program like this is 11%.11 Taken collectively, evidence suggests that poor performance on the TSPU develops early and persists into adulthood for females; though they are most likely to benefit from corrective programming, they are least likely to be included.
One commonly researched program to improve core stability for females is Pilates. Pilates focuses on movement, postural control, and breathing, while increasing the endurance of trunk musculature. Many systematic reviews exist in the literature, with populations studied including women,13 older adults,14 dancers,15 and individuals with low back pain.16 Like most of the core or trunk stability literature, outcome measures vary between studies. However, Pilates has demonstrated effectiveness in improving trunk muscular endurance, as well as other core stability measures, in older women,17 in healthy populations,18 and females with low back pain.19 Therefore, Pilates is a well-researched program across populations and across the lifespan, and it represents the standard of care for many conditions.
Development of a comprehensive program to improve performance on the TSPU that focuses on the population most likely to benefit from programming will provide necessary information for clinicians struggling to improve TSPU performance in active female populations. A pilot study exploring a novel exercise approach to improve trunk stability (NEATS program) outcomes in active females, which included multi-planar and closed kinetic chain exercises, yielded a 45% pass rate (9 of 20) in a recent pilot study.20 What remains unknown is how the novel program improvements in TSPU performance compare to the current standard of care (Pilates). The purpose of this study was to evaluate the effectiveness of a novel exercise approach to a trunk stability (NEATS) program compared to a standard Pilates program on TSPU performance in active females aged 18-45 years. It was hypothesized that subjects in the NEATS program would have greater improvements on outcomes related to trunk stability than subjects in the Pilates program. The primary hypothesis was that higher pass rates on the TSPU would be observed in the NEATS program compared to the Pilates program. Secondary hypotheses included greater improvements in the NEATS program compared to the Pilates program on scores of grip strength, dynamic stability, and fundamental movements.
METHODS
Active women, ages 18-45 years, were recruited from the Stone Family Center for Health Sciences and the University of Evansville campus via email, university-approved flyers, and in-person presentations to participate in the study. Individuals that self-identified as female and met the weekly activity guidelines according to the American Heart Association were included in the study. Exclusion criteria included the following: pain with lumbar or shoulder clearing tests; limitations in the active straight leg raise or shoulder mobility; history of lumbar or shoulder surgery; lumbar or upper extremity pain within the prior three months; history of anterior shoulder instability (or recurrent shoulder dislocations); current pregnancy; other non-musculoskeletal issue resulting in exercise restrictions from a healthcare provider; successful performance (score of 3) on the TSPU. All data collection procedures were approved by the Institutional Review Board at the University of Evansville.
Data Collection Procedures
After reading and signing consent forms, subjects were asked to complete a demographic form, which included injury history, age, and current activity levels. Height and weight were collected after completion of the demographic form. Next, subjects were screened for pain with the lumbar clearing test (performing a prone press up) and shoulder clearing tests (reaching across the body and lifting the elbow). Limitations in shoulder mobility (reaching over and behind the head with one hand while reaching under and behind the lower back i.e. “scratch test”) and active straight leg raising (lying supine, raising one leg toward the ceiling) were assessed.
Subjects also completed the following tests/assessments: Beighton criteria, the FMSTM (as described by Cook et al21), the upper (YBT-UQ) and lower quarter (YBT-LQ) Y-Balance Test, and a grip strength assessment. Beighton criteria, a commonly used clinical screen for generalized hypermobility, screens for hypermobility in the following joints: fifth metacarpal-phalangeals, thumbs, knees, elbows, and spine/hips through forward flexion. All movements, except forward flexion, are assessed bilaterally, and the total number of hypermobile joints is recorded. Scoring for the Beighton criteria has demonstrated good reliability in adult women.22 Next, the FMSTM was performed using previously established procedures for conducting and scoring the screen.5 Next, the Y-Balance tests for the upper and lower body were performed per established procedures suing the YBT kit. Reliability of both the YBT-UQ23 and the YBT-LQ are excellent.24 Subjects performed the reaching task for the YBT-UQ and YBT-LQ on both sides, three times each. Finally, grip strength was assessed using a handheld grip dynamometer. Grip strength testing using a Jamar dynamometer has excellent reliability.25 Subjects completed three trials of maximal gripping in three positions: elbow extended at the side, elbow flexed to 90°, and elbow extended overhead. Subjects had 30 seconds of rest between each trial, and the best trial was used for analysis.
All data collection procedures were completed by the primary investigator, three additional physical therapy faculty members, and one staff physical therapist. All data collectors were blinded to group allocation and participated in pretest and posttest data collection only. All faculty members have more than 10 years of experience delivering care in the outpatient physical therapy setting, are currently or had previously been certified clinical specialists through the American Board of Physical Therapy Specialities, and they have been faculty members for two to six years. The staff physical therapist has six years of experience in an outpatient physical therapy setting.
Interventions
Subjects that were unsuccessful on the TSPU were randomized to receive either instruction in the NEATS program or a Pilates program using demonstrations, return-demonstrations, and written handouts from one of the student physical therapists. In both the NEATS and Pilates programs, student physical therapists used standardized checklists to ensure proper instruction and performance of exercises.
The NEATS program was investigated in a pilot study to determine effectiveness in active females; based on previous results, it was modified to include an additional two weeks of higher intensity and resistance exercises. In brief, the program is a dynamic, multiplanar program that progressed through neurodevelopmental postures to increase stability demands. External loads, through a variety of equipment, were also added throughout the progression of the program. All participants in the NEATS program were issued a medium resistance band, 8kg kettlebell, and 10lb medicine ball at data collection for use throughout the intervention period. For detailed descriptions of exercises, see Appendix A.
The Pilates program is a direct replication of the intervention used by Elmore et al, which demonstrated improvements on similar outcomes in a sample of collegiate dancers. In brief, the Pilates program utilized standard Pilates exercises with an emphasis on breathing technique. All participants in the Pilates program were issued a yoga block, yoga mat, and medium resistance band for use throughout the intervention program. For detailed descriptions of exercises, see Appendix B.
The exercises issued for both programs were performed at least once daily, and compliance was documented by subjects in an exercise journal. Subjects returned for follow-ups at week 2, week 4, and week 6 for further instruction in exercise progression for both programs. All subjects were encouraged to continue their normal daily activities and fitness routines.
Post testing occurred eight weeks after initial data collection, which was performed by the original data collection team and included all original assessments.
STATISTICAL METHODS
With a 2-tailed alpha level of significance equal to 0.05, 32 subjects were needed to have >80% power to detect the primary hypothesis described above based on a chi-square test. All data were analyzed using SPSS (IBM, version 28). Shapiro-Wilk tests were performed on all secondary, continuous outcomes to determine normality of data distributions. Means and standard deviations were calculated for all continuous outcomes, and between-group and within-group analyses included independent and dependent t-tests, respectively. All ordinal data were analyzed using Mann Whitney U and categorical changes were analyzed using Wilcoxon Signed Ranks.
RESULTS
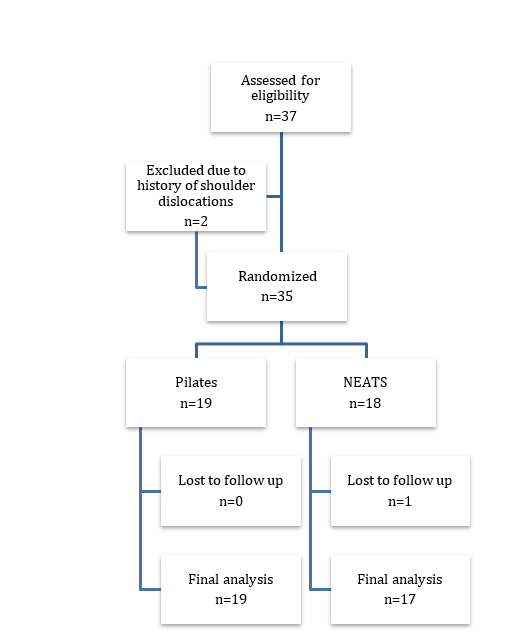
Thirty-seven women (NEATS [n=18]; Pilates [n=19]) were included in the study. One subject from the NEATS group was lost to follow-up, so the remaining 17 subjects were used for the final analysis (Figure 1). Demographics are summarized in Table 1. No significant differences between groups were observed in demographics at pretest. Median Beighton scores were 2 for the NEATS group and 3 for the Pilates group (range=0-9), though no significant differences were observed (p=.39).

The main outcome was between-group pass rates on the TSPU, with a “pass” defined as scoring a 2 or higher. At posttest, 41% (n=7) of the NEATS group and 42% (n=8) of the Pilates group had passing scores on the TSPU, though the between groups difference was not significant (ꭕ2=0.001, p=0.97, Table 2). In the NEATS group, one significant difference was noted in the within-group analysis. Grip strength on the right with the elbow flexed to 90 degrees decreased from 72.82 to 69.82, (p=0.04). No other significant differences were observed in the NEATS group on the remaining continuous variables (p=.10-.96; Table 3). Within-group improvements were noted in the Pilates group as well, though only one (posterolateral reach on the YBT-LQ) reached a statistically significant difference (pre 96.56 [SD 8.26], post 99.03 [SD 8.23]; p=0.03; Table 4). All other differences in continuous outcomes in the Pilates group were not significantly different (p=0.06-0.86). Between-group differences on all posttest continuous measures were not significant (p=0.18-0.95; Table 5), though posttest means were higher in the Pilates group in all but one measure (inferolateral reach of the YBT-UQ on the left).
No significant differences in individual FMSTM scores or composite scores were observed between groups at posttest using the Mann Whitney U (p=0.41-0.78, Table 6). Though group comparisons are typical for the study design, individual outcomes were also analyzed using the Wilcoxon Signed Ranks. A frequency count of categorical changes was tracked for each movement of the FMSTM. If a subject made an improvement, defined as a posttest score higher than the pretest score, this categorical change was documented as a “+”. If a subject’s posttest score decreased from baseline, it was documented as a “-”. If no changes from baseline were noted, this was documented as a tie and was dropped from the analysis per standard Wilcoxon Signed Ranks procedures. Within-group improvements on categorical changes in individual scores on the FMSTM were noted in both the TSPU (NEATS, p=0.03; Pilates, p=0.01) and total FMSTM scores (NEATS, p=0.01; Pilates, p=0.01, Table 6).
DISCUSSION
Current literature suggests that poor performance on the TSPU for females begins in early adolescence and persists through adulthood. Though active females have the greatest need for intervention programs targeting trunk stability outcomes, they are often underrepresented in the literature. Subjects in both the NEATS and Pilates programs improved TSPU performance from pretest to posttest, as well as total FMSTM score. Though no significant between-group differences were observed in pass rates for the TSPU, both programs yielded among the highest pass rates for active females in empirical literature.
The purpose of this study was to compare effectiveness of the NEATS to an established trunk stability program (Pilates) on trunk stability outcomes for active females. The primary hypothesis was that subjects in the NEATS program would demonstrate greater pass rates on the TSPU compared to the Pilates program. No significant between-group differences were observed, indicating that this hypothesis was not supported. However, the pass rates observed in this study (NEATS=41%, Pilates=42%) are comparable to our pilot study, which yielded a 45% pass rate with the NEATS program.20 These findings suggest that both programs, though different in approach and external resistance loads, can be effective in improving trunk stability outcomes for a moderate proportion of active females. The ability to match interventions based on the preferences of either the patient or provider has been shown to positively impact patient outcomes.26 This study provides several options for exercise prescription and progression, creating the opportunity to leverage preferences as a means to improve clinical outcomes.
There are a limited number of intervention studies designed to improve FMSTM scores. The interventions vary from individualized correctives to group yoga, and most are effective at improving composite FMSTM scores.27–33 Unfortunately, only four intervention studies include females,27,29,30,33 ranging in sample sizes of four to eighteen, for a total of 45 female subjects between the four studies. As described previously, there are significant differences in performance on the FMSTM between males and females, yet effectiveness of intervention programs has almost exclusively been studied in male populations. The assumption that these programs should be the gold standard for female populations is problematic; anecdotally, many clinicians struggle to improve TSPU performance in active females, and this struggle is supported through empirical literature. Additionally, rigorous designs comparing high quality programs for females are non-existent. Of the three studies using control groups,27,28,33 only two utilized randomization27,33 and only one implemented blinding.33 Not only is the current study the only intervention study to include an all-female sample, but it is also one of the most rigorously-designed.
The NEATS program was modified from its original length of six weeks to eight weeks. Other corrective programs have also utilized eight-week intervention periods,28,32,34 adding more credibility to an extended intervention period. Unfortunately, pass rates from both the NEATS program and the Pilates program did not exceed the pass rates of previously published studies. Though self-reported compliance to both programs was high, the additional time and complexity of exercises did not appear to aid in performance improvements.
The Pilates program used in this study was replicated from a previous study by Elmore et al., which aimed to improve functional outcomes in collegiate dancers.35 Though typical Pilates-based exercises were used in this program, the biweekly progression of exercises utilized a neurodevelopmental approach, which increased stability demands through postural changes. Initial Pilates exercises were performed in low level postures, such as supine neutral spine dynamic stabilization, and eventually progressed to standing exercises like a resisted horizontal press. This neurodevelopmental approach was also utilized in the NEATS program, where initial exercises included quadruped lumbar flexion and extension before progressing to higher level postures like standing med ball throws. Increasing postural demands through a developmental sequence is thought to improve coordination of trunk musculature,36 which is necessary for active populations. Mahdieh et al37 compared a neurodevelopmental approach to a routine physical fitness program and observed significant improvements in scores on the FMSTM and YBT-LQ in a sample of adult females. Improvements in outcomes utilizing neurodevelopmental postures have been noted in other populations as well. Increased diaphragmatic activity and thickness of the transversus abdominis and internal oblique were observed in patients following stroke.38 Taken collectively, these findings suggest that it is possible that the similarity in postural progressions, rather than the exercises themselves, played an important role in the positive findings, leading to similarities in pass rates as well.
Secondary hypotheses included changes in grip strength, dynamic balance, and fundamental movements. Despite the inclusion of several continuous secondary outcomes, no between-group differences were observed. The exclusion criteria in this study included limitations in shoulder mobility and active straight leg raise—two of the seven movements of the FMSTM —to ensure that improvements in primary or secondary outcomes would not be prohibited by major mobility limitations. Therefore, significant improvements in some movements were not anticipated. However, within-group differences were noted in the right posterolateral reach of the YBT-LQ in the Pilates group, and right grip strength with the elbow flexed in the NEATS group. Given that no other differences were noted, the cause of these differences is not well-understood. However, research has demonstrated that the secondary outcomes selected for this study measure different constructs related to trunk musculature.39 The authors believe that this inconsistent response in the current findings further supports that these tests are measuring different things, and should be considered in comprehensive assessments of trunk stability outcomes.
One major difference between programs was the emphasis on breathing patterns. In the Pilates group, subjects were instructed to pair inhalation and exhalation with specific portions of the exercise. In the NEATS group, no specific instructions on breathing were provided. This manipulation of breath with activity, such as in hypopressive exercises, is becoming common in pelvic health physical therapy. Hypopressive exercises, where a full exhalation is utilized to recruit deep core musculature, have shown some promise in the literature. In healthy females, surface electromyography captured increased activation of pelvic floor muscles during hypopressive exercise.40 Utilizing surface electromyography and vaginal dynamometry, hypopressive exercises were shown to increase activation of pelvic floor and abdominal muscles in a sample of multiparous women.41 Given the important role that these muscles play in trunk stability, emphasizing conscious recruitment through emphasis on structured breathing may lead to improved trunk stability outcomes.
Limitations
The study findings should be interpreted with caution, as limitations were noted. First, subjects were recruited through multiple sites using digital and physical flyers as well as word of mouth. However, 66% (n=24) were physical therapy students from the local health sciences center where the study took place. Though it was intended to recruit women aged 18-45 years, only five subjects were over the age of 30, limiting generalizability. Second, all subjects were free of musculoskeletal pain prior to beginning and throughout the duration of the study, which limits applicability of these findings to patients seeking orthopedic care for musculoskeletal symptoms like low back pain. Finally, though subjects were considered healthy, information regarding subjects’ history of pregnancies, childbirth, and pelvic floor dysfunction was not collected. These additional details may have provided valuable insight into individual variability in outcomes. Therefore, clinicians should utilize clinical reasoning before implementing either program in patients currently experiencing or recovering from musculoskeletal symptoms.
CONCLUSION
Though poor trunk stability in females develops at a young age and appears to persist through adulthood, a disparity exists in the inclusion of females in intervention programs. Given the link between poor trunk stability and musculoskeletal injury, as well as sex difference in performance on trunk stability measures, there is a critical need to develop effective programs for females to address trunk stability deficits. Improvements in trunk stability were comparable between the multi-planar NEATS program and a Pilates program, providing two options for clinicians to utilize in active female populations.
Conflicts of Interest
The authors report no conflicts of interest.
Acknowledgements
The authors would like to acknowledge the following people for their contributions to this project: Sarah Gehres, McKenzi Goebel, Lauren Rennie, Parker Rose, Andrew Patton, Kyle Patton, Jamie Vance, and Kourtney West.