



INTRODUCTION
The number of injuries to the ulnar collateral ligament (UCL) of the elbow are rising every year. Several studies1,2 have reported increasing numbers of injuries, associated surgeries, and that patients affected by UCL pathology are gradually becoming younger. Erickson reported the average age of patients undergoing UCL surgery was between 16 and 19 years of age.3 In another recent study, Matsuura et al. showed that 30% of youth baseball players up to the age of 12 reported episodes of shoulder or elbow pain.4 Hodgins et al. reported a 200% increase in UCL surgeries in the state of New York over a 10-year period.2 Furthermore, 25% of all pitchers in Major League Baseball have undergone UCL surgery, as well as 16% of minor league pitchers.1 In a follow-up study, Conte et al.5 noted the number of minor league pitchers reporting prior UCL surgery increased by 5% and the number of major league pitchers affected increased to 26%. In a fifteen year span, Conte et al. has described a gradual increase in elbow injuries and a gradual decrease in shoulder injuries in Major League Baseball pitchers.6
The cause of these unacceptably high injury rates in overhead athletes, specifically the younger athletes, has been attributed to several factors. Reinjury rates of UE athletes, both contact and non-contact, has also been a concern with rates reported as high as 64%.7 First, there is a surprising overall lack of return to play (RTP) testing generally utilized in making RTP decisions. In a recent systematic review, Fried et al. demonstrated that only 60% of the included studies reported using some sort of RTP criteria in athletes following a shoulder stabilization procedure.8 Another systematic review of 52 articles found no consensus on RTP criteria following upper extremity (UE) surgery in athletes, with 71% reporting utilization of time from surgery as the most common.9 Time from the injury itself is not the primary element that will determine readiness to RTP or competition. The recovery and RTP of an athlete after injury is a multifaceted clinical decision. This lack of testing is disappointing when one considers a reduction in reinjury rates has been demonstrated by utilizing objective RTP testing in the decision-making process in patients with ACL injuries.10 Second, athletes are returning to participate in sports without completing the entire rehabilitation process, often due to insurance plan limitations, an inability to afford rehabilitation following the exhaustion of benefits, or self-discharge. Each of these factors results in incomplete rehabilitation, placing the athlete at risk of reinjury. Aboalota et al. found those who performed rehabilitation for less than six months following arthroscopic Bankart repair for anterior-inferior shoulder instability had a significant reinjury rate compared to those who performed physical therapy greater than six months, 23.1% and 9.6% respectively.11 Third, is the frequent lack of high-level activities and functional sport-specific challenges during the rehabilitation process. Rehabilitation specialists must challenge athletes in a similar manner to that which they will experience on the field, replicating the demands of their sport. Without this, athletes are often returning to their sport inadequately prepared and therefore at a potentially higher risk of re-injury.
Researchers have identified several factors that can predispose overhead athletes to an increased risk of injury. In studies performed at the American Sports Medicine Institute (ASMI), Fleisig et al.12,13 has demonstrated the following risk factors for the development of injury in pitchers:
-
Pitching > 100 innings in one year = 3x greater risk of injury
-
Averaging > 80 pitches per game = 4x greater risk of injury
-
Pitching > 8 months per year = 5x greater risk of injury
-
Regularly pitching with arm fatigue = 36x greater risk of injury
-
Specialization – playing one sport (i.e. baseball and only pitching)
Early sports specialization may also play a role in increasing injury rates in youth athletes simply due to increased exposure. In a recent survey including over 3,000 high school, college and professional athletes, current high school athletes specialized an average of 2 years earlier than current collegiate and professional athletes.14 The results of this survey challenge the notion that success at an elite level requires athletes to specialize in one sport at a very young age. The thought is that specialization in one sport earlier will result in enhanced performance and progression to an elite level; however, there is no evidence to indicate early sport specialization enhances performance and/or progression to an elite level. Instead, early specialization can lead to burnout, overuse injuries, and reduced athletic development in youth athletes.12,13
Numerous studies have shown with an increase in maximum velocity there is increased stress on the medial elbow and increased risk for injury.15–17 There is a trend towards velocity-based training in baseball pitchers. While increased stress on the UCL does not necessarily mean an athlete will get injured, numerous studies have demonstrated a relationship between the upward trend in velocity over time and an increase in UCL injuries.15–17 The UCL ligament can adapt to the stress of throwing over a single season. Chalmers et al. showed that within a single season, the UCL thickens and increases in laxity due to the stresses of throwing, and that these effects are slightly reversed during the offseason.18
Another factor that can predispose an overhead athlete to injury is shoulder mobility and range of motion (ROM). Wilk et al. demonstrated that a deficit of greater than 5 degrees in total rotation motion (TRM) (shoulder external rotation + shoulder internal rotation) in professional baseball pitchers, led to a 2.5x increased risk of injury.19 In another study, Wilk et al. demonstrated the importance of shoulder flexion mobility noting that a decrease in shoulder flexion ROM greater than 5 degrees led to a 3-fold increased risk of injury.20
Return to play testing for the lower extremity has been discussed extensively with more than 500 articles written on RTP guidelines, criteria, and suggestions following knee injuries; however, articles addressing RTP following shoulder injury are lacking. Thorsness et al. have illustrated that RTP outcomes are often poorly described when evaluating overhead athletes.21 Alentorn-Geli et al. suggested RTP after arthroscopic shoulder capsulolabral repair once patients have pain free ROM and greater than 80% strength compared with the contralateral side.22 Similarly, researchers assessing RTP after arthroscopic shoulder plication for multidirectional instability determined RTP by range of motion, time from surgery (three months for non-contact and six months contact sports), and the Oxford Instability scores pre- and post-operatively.23
Most RTP decisions are made in the physician’s office, based solely on physical examination and subjective reporting. Davies and Riemann published an article comparing a PRO (Quick-DASH) and an UE functional performance test (seated single arm shot put test).24 Their original hypothesis was that there would be a high correlation between the two measurements; surprisingly, there was a low correlation. This suggests the tests are measuring different constructs and cannot be used as a substitute for one another for clinical decision-making for return to sport.24 When RTP testing is performed, it is important to consider the ecological validity of the testing that is being performed to be respresent the demands of each athletes’ sport. Testing is typically not done in the same environment or with sport specificity, therefore, using specific objective functional tests and predetermined criteria minimizes the reliance on the subjective element alone during athlete progression.
In 2020, Wilk et al. published a clinical commentary reviewing the current RTP criteria following shoulder injuries and the current tests they utilize.25 Additionally, Riemann et al. provided the psychometric properties of some of the more traditional functional performance tests of the UE for overhead athletes.26 Some of these tests which may be used as a preliminary assessment for the patient to advance to the more demanding reactive neurocognitive (RNC) testing can be found in Table 1. Neurocognitive aspects of RTP have recently been included in functional testing for overhead athletes in order to better access atheltes reactive and unanticapatory control consistent with the demands of sport.
Moreover, as patients progress to performing the more demanding and ecologically valid neurocognitive reactive testing, it’s important to establish some of the psychometric properties of the fundamental tests. Lewis et al. recently completed the initial reliability testing on the closed kinetic chain (CKC) neurocognitive reactive testing (ICCs ranged from 0.573-0.816)27 and OKC neurocognitive reactive testing (ICCs ranged from 0.573-0.825)28 using the Blaze Pods (Tel Aviv, Israel).
Therefore, the purpose of this clinical commentary was to describe the utilization of a series of UE reactive neurocognitive (RNC) tests for RTP for overhead athletes(baseball and softball) utilizing the Blaze Pod light system
NEUROCOGNITIVE TESTING
Appropriate testing of RTP readiness following UE injury should not only assess if the athlete appears ready to resume play but also be directed toward minimizing the risk of reinjury. To accomplish this, testing must be more dynamic, sport oriented, and unpredictable in nature. A neurocognitive testing battery must include measures of reactive response and incorporate sport-type reactions and movements. Neurocognitive testing can measure various aspects of cognitive function non-invasively; these cognitive functions include reaction time, multitasking, attention, memory, and perception. Short tests designed to assess these functions produce objective measures that can be compared to standard scores or to an individual’s baseline scores when available.
Readiness to return to sport involves more than just the readiness of the musculoskeletal system. Musculoskeletal injuries affect the neurocognitive system as well; therefore, assessing and training this system may lead to better outcomes when determining readiness to return to play. The neurocognitive system is a vital aspect of sport due to the constant use of cognitive functions such as reaction time and multi-tasking. Spiteri et al. demonstrated that reaction time testing has been shown to be highly reliable and can be used to assess an athlete’s cognitive and athletic ability.29 Shitara and colleagues found that when comparing individuals with recurrent shoulder instability (RSI) to healthy individuals, those with RSI demonstrate abnormal motor control during voluntary shoulder contraction as well as a decline in proprioception during shoulder passive range of motion.30 This neuroplastic change as a result of injury has also been shown to occur in both LEs after an anterior cruciate ligament (ACL) injury.31 Simon et al. demonstrated that adding a neurocognitive and anticipatory component to the traditional hop test series in athletes recovering from LE injuries resulted in a statistical difference in performance and may improve functional return to sport testing.32 When comparing reactive versus preplanned agility testing, Serpell et al. reported a statistical significant difference in mean reaction time between elite and subelite groups in the way in which they contributed to perceptual skills and/or reaction ability.33 These factors combine to make the incorporation of neurocognitive training and testing elements crucial to advancing the effectiveness of RTP testing following UE injuries and may help to minimize the risk of reinjury as the athlete returns to competition.
TESTING SEQUENCE
Currently the researchers are collecting data on the testing sequence discussed in this manuscript regarding reference values for number of taps, reaction time, and errors for each test. Presented in this manuscript is the current data to date consisting of 143 subjects, 73 high school and 70 collegiate athletes (106 baseball and 37 softball). The study was approved by the Institutional Review Board (IRB) and all subjects consented to participate in the study.
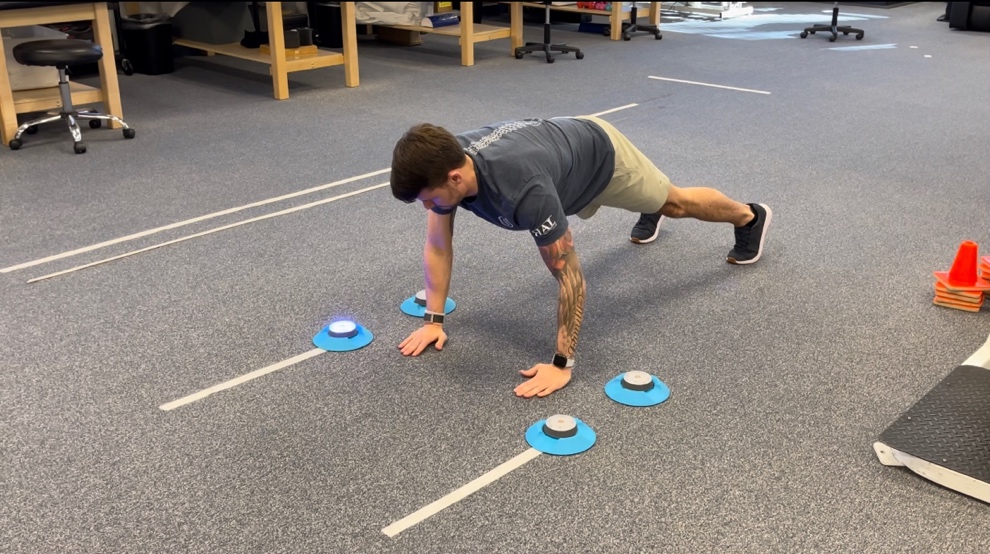
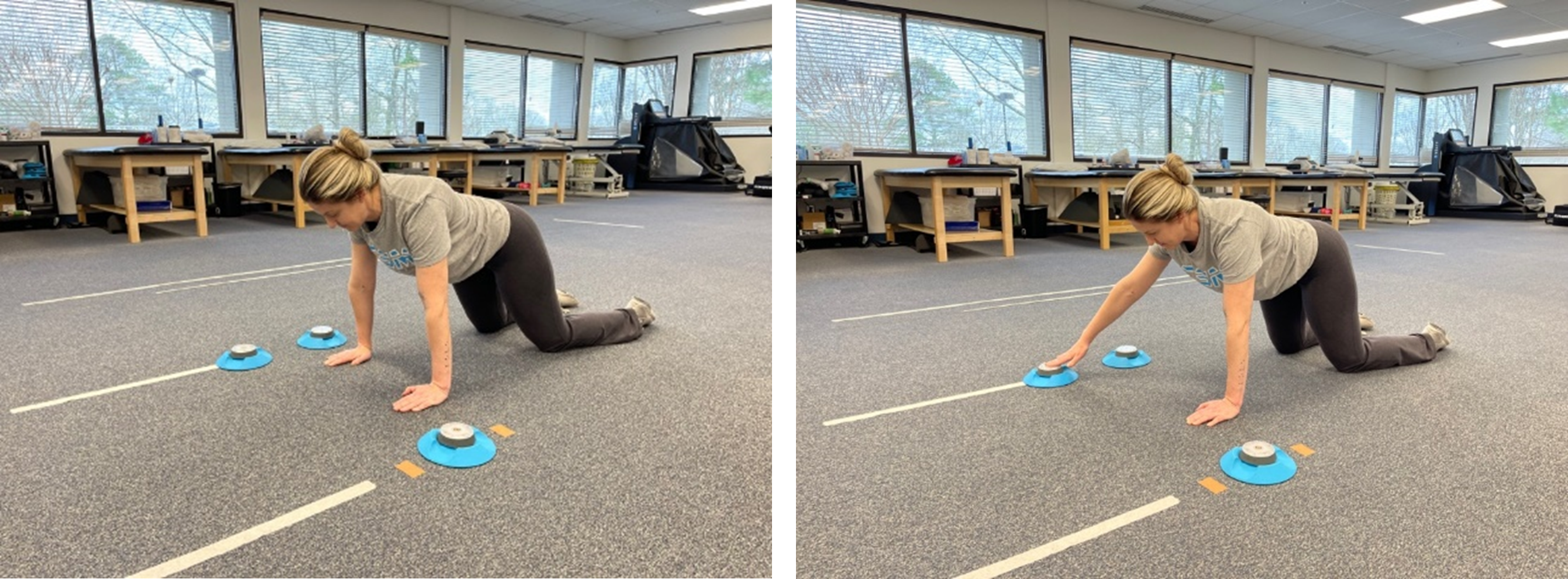
The UE neurocognitive testing sequence currently employed consists of 4 different tests utilizing the Blaze Pod light system. The four tests included in the protocol are (1) reactive CKCUEST+ (Figure 1), (2) reactive triangle CKCUEST+ (Figure 2), (3) reactive right vs. left CKCUEST+ (Figure 3), and (4) reactive OKC 90/90 wall throws (Figure 4). Refer to Appendix 1 for a QR code consisting of a video of each test described. The Blaze Pod system is synchronized with an application-based system which provides real time feedback regarding number of taps, reaction time, and errors for each participant following each test. Athletes are provided a fifteen second rest between sets of the same test and one minute rest prior to initiating the next test in the sequence. As an alternative, these tests may be performed standing with the Blaze Pods mounted on the wall for those athletes that may not be able to maintain a plank. For individuals who are unable to hold a full plank position due to strength and/or pain/discomfort, a modified testing position shown in Figures 5 and 6 may be utilized. Tables 2 through5 describe the reference values collected for each test thus far including number of taps, reaction time, and errors. For each test, the data has been separated by sport (Tables 2a-5a, baseball or softball) and by level of competition (Tables 2b-5b,high school or college).
Test 1: Reactive CKCUEST+
Testing description:
-
15 second test, completed twice bilaterally
-
Three Blazepods positioned 36" apart with two of the three on the same side being 12" apart
-
Single pod is positioned so that it is centered between the two on the opposite side
-
Blazepods configured in a home base pattern
-
Lights are set to transition on a hit and with zero-time delay
-
Target color (blue) selected for the two pods on the same side with the other target color on the opposite side being red
-
The athlete begins in a high plank position with their hands directly medial to the individual pod and between the other two with their feet shoulder-width apart
-
Instruct to stabilize on a single arm and hit the pod that lights blue first followed by red and repeat, going back and forth with one hand
-
The goal is to tap as many lights as possible in the time allocated
-
Total number of taps as well as average reaction time are calculated following completion of the test
-
Limb symmetry index (affected extremity/un-affected extremity x 100) (LSI) is calculated to compare side-to-side differences
._blazepods_are_positioned_36_inches_.jpeg)
Test 2: Reactive Triangle CKCUEST+
Testing description:
-
15 second test, completed 2x bilaterally
-
Three Blaze Pods positioned 36" apart with two of the three on the same side being 12" apart
-
Single pod is positioned so that it is centered between the two on the opposite side
-
Blazepods configured with the focus sequence - one will illuminate the predetermined target color (blue) and the other two will be random distracting colors
-
Lights are set to transition on a hit and with zero-time delay between each
-
The athlete begins in a high plank position with their hands directly medial to the individual pod and between the other two with feet shoulder-width apart
-
Instruct to stabilize on a single arm and hit the pod which illuminates the target color (blue) utilizing the opposite hand as many times as possible in the allocated time
-
The goal is to tap as many lights as possible in the time allocated
-
Total number of taps, errors, as well as average reaction time are recorded
-
Limb symmetry index (LSI) is calculated to compare side-to-side differences
._pods_are_positioned_36.jpeg)
Test 3: Reactive Right vs. Left CKCUEST+
Testing description:
-
15 second test, completed twice
-
Four Blazepods positioned in a rectangle 36" in length and 12" in width with two on each side
-
Blazepods configured in a randomized pattern so that any of the four can illuminate with only one at a single point in time
-
Lights are set to transition on a hit and with zero-time delay between each
-
Both blue and red are set as the target colors which represents the color in which the single pod will illuminate
-
The athlete begins in a high plank position with their hands between the two pods on each side and feet shoulder-width apart
-
If the pod illuminates blue they are instructed to hit it with their left hand and if red, then hit it with their right hand
-
The goal is to tap as many lights as possible in the time allocated
-
Total number of taps, errors, as well as average reaction time are recorded
._pods_are_positioned_.jpeg)
Test 4: Reactive OKC 90/90 Wall Throws
Testing description:
-
15 second test, completed twice bilaterally
-
Six Blazepods
-
Three pods are positioned in a vertical line on a wall separated 12" apart from each other, 6" from the corner and with the middle pod 5’ from the floor
-
Remaining three pods are positioned in the same manner on the opposite door frame or side of the corner
-
Blazepods configured with the focus sequence in that one will illuminate the predetermined target color (blue) and the other two will be random distracting colors
-
Lights are set to transition on a hit and with zero-time delay between each
-
The athlete begins facing the wall with their arm in 90 degrees abduction & 90 degrees elbow flexion holding a 2lb plyoball
-
Instruct to complete continuous wall throws, maintaining adequate shoulder and elbow positioning, while tapping the pod which illuminates the target color utilizing the opposite hand as many times as possible in the allocated time
-
Total number of taps, errors, as well as average reaction time are recorded
-
Limb symmetry index (LSI) is calculated to compare side to side differences
._middle_pod_is_positioned_5.jpeg)
_in_a.png)
_in_a_modified_testing_position.png)
LIMITATIONS AND FUTURE RESEARCH
Although these are examples of some of the tests that are currently being used clinically because of ecological validity, we must acknowledge the limitations of these tests. The tests are currently being tested for reliability and validity regarding follow-up effectiveness for athletes to RTP, return to performance or prevention of reinjury, therefore, there is no data currently to report for these outcomes. Future research is still needed looking at sport specific testing for other UE athletes, validity and relaiability of the current testing protocol, and the ability to predict/access reinjury or return to play rates.
CONCLUSION
Upper extremity injuries in overhead athletes have continued to increase over the years particularly in the younger athletes. There are several of factors that may be contributing to the rise in injury such as the lack of RTP criteria, year-round pitching, early sport specialization, and the pursuit of higher velocity. The current state of RTP testing following UE injuries is inadequate and does not reflect the unpredictable, dynamic environment athletes are returning to. Not only is there a need for better utilization of RTP testing for predicting readiness, the significant incidence of reinjury must also be reduced. Following injury, neuroplastic changes lead to increased reliance on reactive cognitive function and focus to complete a task that one time required minimal cognitive demand. These needs require both an improvement in the type of tests utilized and the overall use of subjective, objective, and functional RTP testing in determining readiness to resume unrestricted activity. By presenting this theoretical model, our hope is that more critical thought will be utilized when determining the application of reactive neurocognitive testing in assessing athletic readiness and RTP for UE athletes.
